Which type of thyroid cancer is associated with each of the below characteristics?
- Tumor arises from parafollicular C cells
- Pathology reveals psammoma bodies and Orphan Annie nuclei
- Pathology shows amyloid deposition
- Tumor secretes calcitonin
- Prognosis based on local invasion rather than stage
- Tumor arises from parafollicular C cells: Medullary thryoid carcinoma
- Pathology reveals psammoma bodies and Orphan Annie nuclei: Papillary thyroid cancer
- Pathology shows amyloid deposition: Medullary thryoid carcinoma
- Tumor secretes calcitonin: Medullary thryoid carcinoma (may be useful to monitor calcitonin levels for disease recurrence)
- Prognosis based on local invasion rather than stage: Papillary thyroid carcinoma
What is the best time to perform a thyroidectomy on a pregnant patient?
2nd trimester
[This has the lowest risk of teratogenic events and premature labor.]
What are the expected lab values (high or low) in Graves’ disease?
- TSH
- T3
- T4
- LATS
- 123I uptake (thyroid scan)
- TSH: Decreased
- T3: Increased
- T4: Increased
- LATS: Increased
- 123I uptake (thyroid scan): Diffusely increased
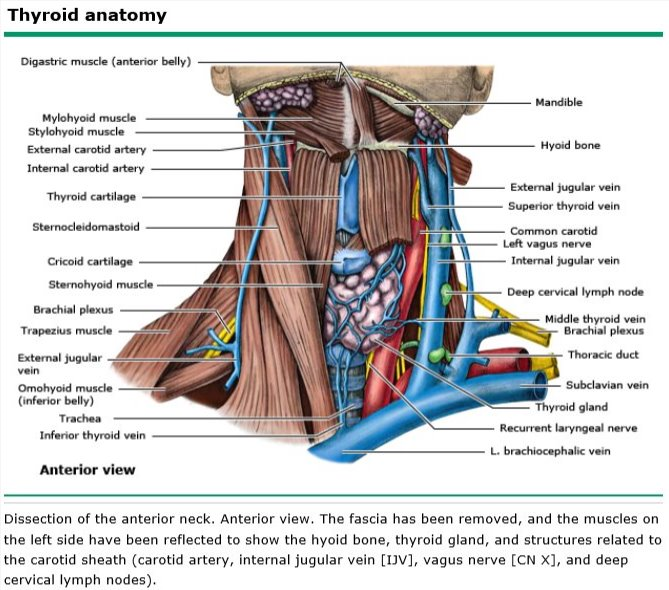
What are the 3 thyroid veins and to where do they drain?
- Superior thyroid vein: Drains into the internal jugular vein
- Middle thyroid vein: Drains into the internal jugular vein
- Inferior thyroid vein: Drains into the innominate vein
What do parafollicular C cells produce?
Calcitonin
What is the most common cause of hypothyroidism in adults and what is the pathogenesis of that cause?
- Hashimoto’s disease
- Caused by both humeral and cell-mediated autoimmune disease (microsomal and thyroglobulin antibodies)
[Goiter occurs secondary to lack of organification of trapped iodide inside the thyroid gland. It can cause thyrotoxicosis in the early stages of the disease.]
What is the treatment approach to papillary or follicular cell thyroid cancer with metastases?
Total thyroidectomy followed by 131I 4-6 weeks after surgery
[Total thyroidectomy needs to be performed first to facilitate uptake of 131I to the metastatic lesions, otherwise it will all get absorbed by the thyroid gland.]
What is the treatment for Hashimoto’s disease?
- Thyroxine is first line therapy
- Partial thyroidectomy if continues to grow despite thyroxine therapy, if nodules appear, or if symptoms of compression occur
[Frequently, no surgery is necessary for Hashimoto’s disease.]
What is the treatment for a toxic multinodular goiter?
- Most consider surgery (subtotal or total thyroidectomy) the preferred initial treatment
- Trial of 131I should be considered, especially in the elderly and frail
[If compression or a suspicious nodule is present then surgery is the necessary treatment.]
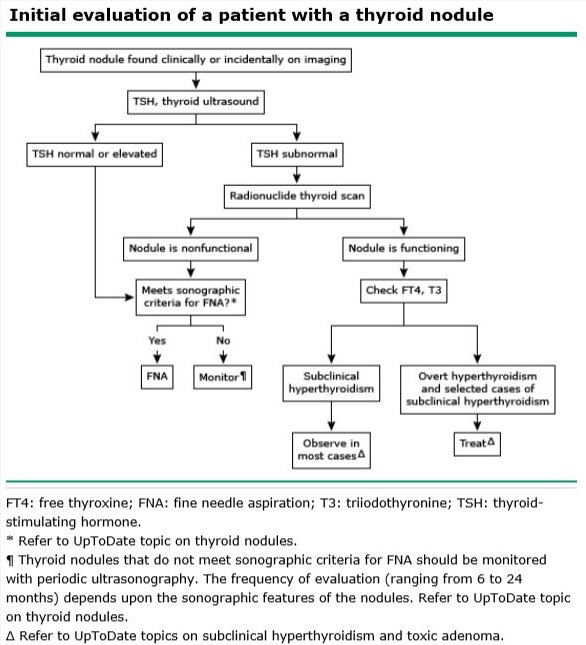
What is the appropriate next in step working up a patient with an asymptomatic thyroid nodule with indeterminant findings on fine needle aspiration?
Radionuclide study
[UpToDate: The initial evaluation in all patients with a thyroid nodule (discovered either by palpation or incidentally noted on a radiologic procedure, such as carotid ultrasonography, neck computed tomography [CT], or positron emission tomography [PET]) includes a history, physical examination, neck ultrasonography, and measurement of serum thyroid-stimulating hormone (TSH).
Thyroid scintigraphy should be performed in patients with a subnormal serum TSH concentration.
If the serum TSH concentration is normal or elevated and the nodule meets sonographic criteria for sampling (table 3), palpation or ultrasound-guided fine needle aspiration (FNA) biopsy should be performed (algorithm 1). FNA biopsy is the most accurate method for evaluating thyroid nodules and selecting patients for thyroid surgery. Nodules that do not meet sonographic criteria for FNA should be monitored. The frequency of evaluation depends upon the sonographic features of the nodules.
Solid hypoechoic nodules and nodules with suspicious sonographic appearance (irregular margins, microcalcifications, taller than wide shape, rim calcifications, or evidence of extrathyroidal extension) should be biopsied when ≥1 cm (as determined by largest dimension). Nodules with sonographic appearance suggesting a low risk for thyroid cancer can be biopsied when larger (≥1.5 to 2 cm). Spongiform nodules ≥2 cm could also be evaluated by FNA, although observation without FNA is an alternative option.
FNA biopsy of thyroid nodules is commonly performed under ultrasound guidance. Ultrasound-guided FNA biopsy should be performed for nonpalpable nodules and for nodules that are technically difficult to aspirate using palpation methods alone, such as predominantly cystic or posteriorly located nodules. In patients with large nodules (>4 cm), ultrasound-guided FNA directed at several areas within the nodule may reduce the risk of a false negative biopsy.
Where available, we suggest using an mRNA classifier system (gene expresser classifier), mutational analysis (using a broad next-generation sequencing assay with an expanded panel of point mutations and gene fusions), or combined testing for further evaluating FNA aspirates with indeterminate cytology (follicular lesion/atypia of undetermined significance [FLUS/AUS]) or follicular neoplasm.]
What is the appropriate treatment for a patient with an asymptomatic thyroid nodule and the following finding on fine needle aspiration?
- Follicular cells
- Thyroid cancer
- Cyst fluid
- Colloid tissue
- Normal thyroid tissue
- Follicular cells: Lobectomy (10% cancer risk)
- Thyroid cancer: Thyroidectomy or lobectomy (further treatment dependent on cancer type and stage)
- Cyst fluid: Drain fluid (lobectomy if it recurs or is bloody)
- Colloid tissue: Thyroxine (lobectomy if it enlarges)
- Normal thyroid tissue: Monitor (PTU and 131I if symptomatic)
Colloid tissue on FNA is most likely a colloid goiter with a low chance (< 1%) of malignancy.]
[UpToDate: For patients with FLUS or AUS (nodules with atypical cells or nodules with both macrofollicular and microfollicular features), we perform repeat FNA after a three to six-month interval or earlier. If repeat aspirates continue to show FLUS/AUS and thyroid scintigraphy does not show an autonomous nodule, we perform molecular testing (as for follicular neoplasm immediately below). If molecular testing is unavailable, we suggest surgical resection if repeat aspirates continue to show atypical cells (Grade 2C). For patients with nodules that are greater than 50% macrofollicular, we suggest monitoring, unless they are clinically suspicious or present in patients with a higher risk of cancer (Grade 2C).
For patients with nonautonomous (cold) follicular neoplasms (microfollicular adenomas), we send the FNA aspirate for molecular testing (if available) using a gene expresser classifier or mutational analysis with an expanded panel of point mutations and gene fusions or combined testing. If molecular testing is not available, we suggest diagnostic lobectomy rather than observation (Grade 2B). In the absence of capsular or vascular invasion (on surgical histology), the lesion is classified as a benign adenoma and no further treatment is required. For patients whose surgical histology shows follicular thyroid cancer (or follicular variant papillary thyroid cancer), completion thyroidectomy may be necessary.
For patients with indeterminate FNA cytology who have a benign molecular pattern on molecular testing, we suggest observation (Grade 2C). However, the decision to observe a patient with a benign profile should be reassessed as more data become available. Diagnostic lobectomy remains an alternative option for patients with a benign molecular pattern, depending upon the nodule’s clinical characteristics and patient preference. For patients with a suspicious molecular pattern using these techniques, diagnostic lobectomy or total thyroidectomy is indicated.
Patients with cytology suggesting cancer or suspicious for cancer should be referred for surgery.
For patients with nondiagnostic palpation or ultrasound-guided biopsies, we perform repeat FNA using ultrasound-guidance. For patients with solid nodules and nondiagnostic cytology after repeated biopsies, we typically perform an ultrasound-guided core needle biopsy. Careful clinical follow-up, repeat FNA biopsy, and surgical resection are alternative options. For cytologically nondiagnostic nodules that are predominately cystic, we suggest careful clinical follow-up with ultrasound monitoring rather than surgical resection (Grade 2C).]
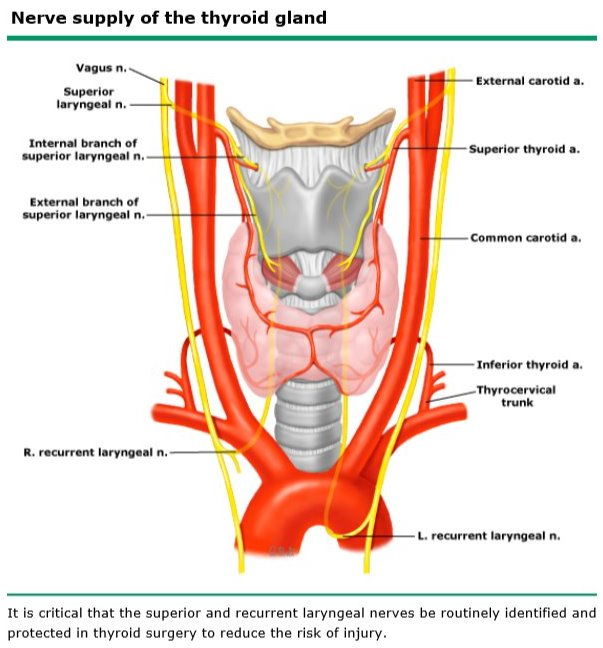
What are the below characteristics of the superior laryngeal nerve?
- Provides motor innervation to what?
- Runs where in relation to the thyroid lobes?
- Tracks close to which artery?
- Injury results in what?
- Provides motor innervation to what? Cricothyroid muscle
- Runs where in relation to the thyroid lobes? Lateral
- Tracks close to which artery? Superior thyroid artery
- Injury results in what? Loss of voice projection and voice fatigability
What is the treatment for a patient with an asymptomatic thyroid nodule with indeterminant findings on fine needle aspiration and the following finding on radionuclide study?
- Hot nodule
- Cold nodule
- Hot nodule: Monitor (PTU and 131I if symptomatic)
- Cold nodule: Lobectomy (more likely malignant than a hot nodule)
[UpToDate: For patients with FLUS or AUS (nodules with atypical cells or nodules with both macrofollicular and microfollicular features), we perform repeat FNA after a three to six-month interval or earlier. If repeat aspirates continue to show FLUS/AUS and thyroid scintigraphy does not show an autonomous nodule, we perform molecular testing (as for follicular neoplasm immediately below). If molecular testing is unavailable, we suggest surgical resection if repeat aspirates continue to show atypical cells (Grade 2C). For patients with nodules that are greater than 50% macrofollicular, we suggest monitoring, unless they are clinically suspicious or present in patients with a higher risk of cancer (Grade 2C).
For patients with nonautonomous (cold) follicular neoplasms (microfollicular adenomas), we send the FNA aspirate for molecular testing (if available) using a gene expresser classifier or mutational analysis with an expanded panel of point mutations and gene fusions or combined testing. If molecular testing is not available, we suggest diagnostic lobectomy rather than observation (Grade 2B). In the absence of capsular or vascular invasion (on surgical histology), the lesion is classified as a benign adenoma and no further treatment is required. For patients whose surgical histology shows follicular thyroid cancer (or follicular variant papillary thyroid cancer), completion thyroidectomy may be necessary.
For patients with indeterminate FNA cytology who have a benign molecular pattern on molecular testing, we suggest observation (Grade 2C). However, the decision to observe a patient with a benign profile should be reassessed as more data become available. Diagnostic lobectomy remains an alternative option for patients with a benign molecular pattern, depending upon the nodule’s clinical characteristics and patient preference. For patients with a suspicious molecular pattern using these techniques, diagnostic lobectomy or total thyroidectomy is indicated.
Patients with cytology suggesting cancer or suspicious for cancer should be referred for surgery.
For patients with nondiagnostic palpation or ultrasound-guided biopsies, we perform repeat FNA using ultrasound-guidance. For patients with solid nodules and nondiagnostic cytology after repeated biopsies, we typically perform an ultrasound-guided core needle biopsy. Careful clinical follow-up, repeat FNA biopsy, and surgical resection are alternative options. For cytologically nondiagnostic nodules that are predominately cystic, we suggest careful clinical follow-up with ultrasound monitoring rather than surgical resection (Grade 2C).]
What are the following characterstics of thyroid cancer?
- Most common type of thyroid cancer
- Least aggressive type of thyroid cancer
- Second least aggressive type of thyroid cancer
- Second most aggressive type of thyroid cancer
- Most aggressive type of thyroid cancer
- Risk of malignancy with follicular cells on thyroid FNA
- Most common type of thyroid cancer: Papillary
- Least aggressive type of thyroid cancer: Papillary (95% 5-year survival)
- Second least aggressive type of thyroid cancer: Follicular (70% 5-year survival)
- Second most aggressive type of thyroid cancer: Medullary (50% 5-year survival)
- Most aggressive type of thyroid cancer: Anaplastic (0% 5-year survival)
- Risk of malignancy with follicular cells on thyroid FNA: 5-10% risk of malignancy (FNA is unable to differentiate between follicular cell adenoma, follicular cell hyperplasia, and follicular cell cancer)
- What is the mechanism of action of propylthiouracil (PTU) and methimazole?
- What is are the side effects of propylthiouracil (PTU)?
- What is are the side effects of methimazole?
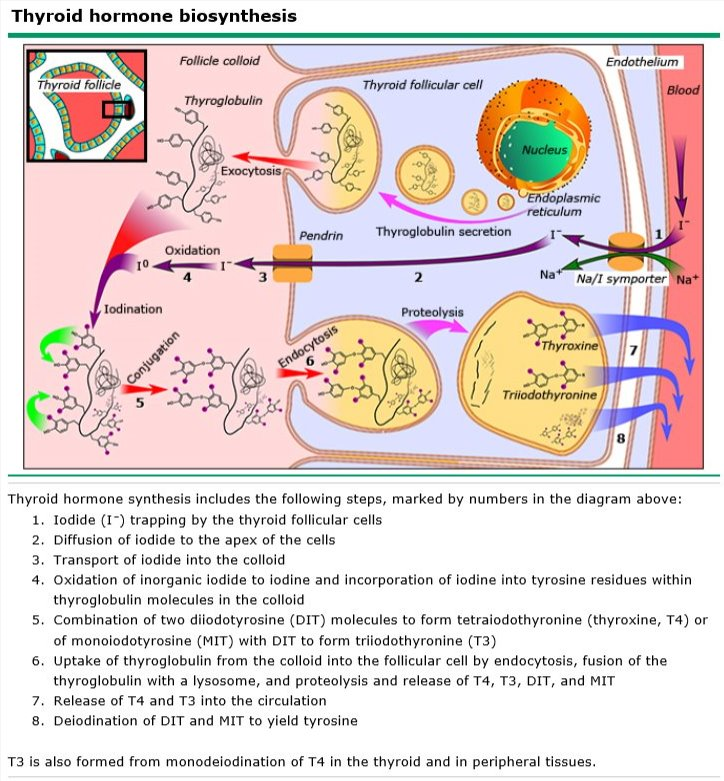
- Mechanism of action of propylthiouracil (PTU) and methimazole: Inhibition of peroxidases and prevention of iodine-tyrosine coupling
- Side effects of propylthiouracil (PTU): Aplastic anemia, agranulocytosis (rare)
- Side effects of methimazole: Cretinism in newborns (crosses placenta), aplastic anemia, and agranulocytosis (rare)
[UpToDate: In addition to intellectual disability, cretinism is accompanied by other neurologic and somatic defects. This has led to cretinism being subdivided into neurologic and myxedematous types:
- Neurologic cretinism is characterized by intellectual disability, deaf mutism, gait disturbances, and spasticity but not hypothyroidism. It is thought to result from hypothyroidism in the mother during early pregnancy but a euthyroid state postnatally due to adequate iodine intake in the newborn.
- Myxedematous cretinism is characterized by intellectual disability, short stature, and hypothyroidism. It is thought to result from iodine deficiency and thyroid injury predominantly late in pregnancy and continuing after birth.
These two syndromes overlap considerably, and attributing them to specific developmental periods is undoubtedly overly simplistic. Both can be prevented by adequate maternal and infant iodine intake.]
What are the following characteristics of thyroglobulin?
- What is the T4:T3 ratio?
- Which is the more active form?
- Where is most T3 produced?
- T4:T3 ratio: 15:1
- More active form: T3
- T3 production: Peripheral conversion of T4 to T3 by deiodinases
[Deiodinases separate iodine from tyrosine.]
What is the treatment for a single toxic thyroid nodule?
- Thioamides and 131I (95% effective)
- Lobectomy if medical treatment is ineffective
[20% of hot nodules eventually cause symptoms.]
What are the following characteristics of thyroid storm?
- Most common cause of death
- Treatment
- Most common cause of death: High-output cardiac failure
- Treatment: Beta-blockers (first line), propylthiouracil (PTU), Lugol’s solution, cooling blankets, oxygen, glucose
What is the treatment for hyperthyroidism in the below patients?
- Young patient with small goiter and mild T3/T4 elevation
- Pregnant patient
- Poor surgical risk patient unresponsive to PTU
- Young patient with small goiter and mild T3/T4 elevation: Propylthiouracil (PTU) and methimazole
- Pregnant patient: Propylthiouracil (safe in pregnancy)
- Poor surgical risk patient unresponsive to PTU: 131I (should not be used in children or during pregnancy)
[Thyroidectomy is indicated for cold nodules, toxic adenomas or multinodular goiters not responsive to medical therapy, pregnant patients not controlled with PTU, compressive symptoms.]
What is the most common cause of a goiter and what is the treatment?
- Iodine deficiency
- Treatment: Iodine replacement
[A nontoxic colloid goiter is a diffuse enlargement without evidence of functional abnormality. Does not usually require an operation unless the goiter is causing airway compression or there is a suspicious nodule.]
- Which rare cause of hypothyroidism has woody and fibrous components that can involve the adjacent strapy muscles and carotid sheath, can resemble thyroid cancer or lymphoma, and is associated with sclerosing cholangitis, fibrotic diseases, and retroperitoneal fibrosis?
- What is the treatment?
- Reidel’s fibrous struma
- Steroids and thyroxine
[May need isthmectomy or tracheostomy for airway symptoms. Impotant to look carefully for recurrent laryngeal nerve if resection is needed.]
UpToDate: Riedel’s thyroiditis (fibrous thyroiditis) was originally described in 1896 by Riedel as a “specific inflammation of mysterious nature producing an iron hard tumefaction of the thyroid.” This disorder is a fibrotic process associated with a mononuclear cell inflammation that extends beyond the thyroid into the perithyroidal soft tissue. The perithyroidal fibrosis can involve the parathyroid glands causing hypoparathyroidism, the recurrent laryngeal nerves causing hoarseness, the trachea causing compression, the mediastinum, and the anterior chest wall. In contrast, other infiltrative and inflammatory conditions of the thyroid do not extend beyond the thyroid capsule.
Riedel’s thyroiditis is extremely rare, with an outpatient incidence of 1.06/100,000 and prevalence of 0.05% or less of surgical thyroid diseases. Women are four times more likely than men to be affected, and it most commonly occurs between the ages of 30 and 50 years.
Etiology — The etiology of Riedel’s thyroiditis is not known. Although Riedel’s disease is often believed to be the local involvement of the thyroid in a systemic disease, multifocal fibrosclerosis, there is limited evidence suggesting that Riedel’s thyroiditis is associated with autoimmune disease or a primary fibrotic process. The presence of mononuclear cells and vasculitis within the fibrous tissue and of high serum antithyroid antibody concentrations in many patients support the concept of an autoimmune mechanism. However, the elevated thyroid antibodies may be a reaction to antigens released from destroyed thyroid tissue.
No etiologic relationship to drugs has been identified in patients with isolated Riedel’s thyroiditis. It seems likely that multifocal fibrosclerosis is a primary fibrotic disorder, with fibroblast proliferation induced by cytokines produced by B or T lymphocytes. Riedel’s thyroiditis may occur with other fibrosing conditions such as retroperitoneal fibrosis, fibrosing mediastinitis, sclerosing cholangitis, pancreatitis, lacrimal fibrosis, orbital pseudotumor fibrosis, and tumefactive fibroinflammatory lesions of the head and neck.
Riedel’s thyroiditis may occur as part of IgG4-related systemic disease. The hallmarks of IgG4-related systemic disease are lymphoplasmacytic tissue infiltration of mainly IgG4-positive plasma cells and small lymphocytes accompanied by fibrosis, obliterative phlebitis, and elevated serum levels of IgG4. Excessive numbers of IgG4-positive plasma cells have been identified in thyroidectomy samples from three patients with Riedel’s thyroiditis.]
Wha its the most common cause of hyperthyroidism and what is the pathogenesis of that cause?
- Graves’ disease (toxic diffuse goiter)
- Caused by IgG antibodies to TSH receptor (long-acting thyroid stimulator (LATS)), thyroid stimulating immunoglobulin (TSI)
What are the indications for 131I treatment in thyroid cancer?
Papillary or follicular thyroid cancer with any of the following characteristics
- Tumor > 1cm
- Extrathyroidal disease
- Primary inoperable tumor
- Recurrent cancer
[131I can cure bone and lung metastases. It is given 4-6 weeks after surgery when TSH levels are highest. Do not give thyroid replacement until after treatment with 131I as it would suppress TSH and uptake of 131I.]
What is the appropriate treatment for the following types of thyroid cancer?
- Papillary thyroid cancer
- Follicular thyroid cancer
- Medullary thyroid cancer
- Anaplastic thyroid cancer
- Hurthle cell carcinoma
- Papillary thyroid cancer: Lobectomy for lesions < 1cm, total thyroidectomy for bilateral lesions, multicentricity, hisotry of XRT, positive margins, or lesions > 1cm, 131I 4-6 weeks after surgery for metastatic disease, residual local disease, positive lymph nodes, or capsular invasion
- Follicular thyroid cancer: Total thyroidectomy for lesions > 1cm or if there is extrathyroidal disease, 131I 4-6 weeks after surgery
- Medullary thyroid cancer: Total thyroidectomy with central neck node dissection, XRT may be useful for unresectable local and distant metastatic disease
- Anaplastic thyroid cancer: Total thyroidectomy for the rare lesion that can be resected (usually beyond surgical management at diagnosis)
- Hurthle cell carcinoma: Total thyroidectomy
[Need modified radical neck dissection for extrathyroidal tissue involvement or clinically positive nodes. 131I is only effective for papillary and follicular thyroid cancer.]









-
25: Thoracic138
-
26: Cardiac76
-
27: Vascular235
-
28: Gastrointestinal Hormones48
-
29: Esophagus122
-
42: Orthopedics194
-
30: Stomach167
-
31: Liver178
-
32: Biliary System148
-
33: Pancreas148
-
1: Cell Biology23
-
2: Hematology138
-
3: Blood Products18
-
4: Immunology46
-
5: Infection111
-
6: Antibiotics57
-
7: Medicines and Pharmacology29
-
8: Anesthesia68
-
9: Fluids and Electrolytes31
-
10: Nutrition34
-
11: Oncology28
-
12: Transplantation38
-
13: Inflammation and Cytokines46
-
14: Wound Healing15
-
16: Critical Care112
-
15: Trauma93
-
17: Burns25
-
18: Plastics, Skin, and Soft Tissue124
-
19: Head and Neck46
-
20: Pituitary11
-
21: Adrenal29
-
22: Thyroid41
-
23: Parathyroid29
-
24: Breast179
-
34: Spleen38
-
35: Small Bowel35
-
36: Colorectal62
-
37: Anal and Rectal19
-
38: Hernias, Abdomen, and Surgical Technology38
-
39: Urology30
-
40: Gynecology35
-
41: Neurosurgery25
-
43: Pediatric Surgery125
-
44: Statistics and Patient Safety32
-
TrueLearn #1274
-
True Learn #2135
-
Scoring Systems11
