Initial Treatment of Stable COPD
What Group & What Drug(s)?
0-1 Moderate Exacerbations
not leading to hospital admin
&
mMRC 0-1 // CAT <10
modified MRC Dyspenea Scale (QOL) // COPD Assessment Test (Symptoms)
Group A
ANY BRONCHODIALATOR
Initial Treatment of Stable COPD
What Group & What Drug(s)?
0-1 Moderate Exacerbations
not leading to hospital admin
&
mMRC > 2 // CAT > 10
modified MRC Dyspenea Scale (QOL) // COPD Assessment Test (Symptoms)
Group B
LONG ACTING BRONCHODIALATOR
LABA = -TEROLs
Indaca-terol // Oloda-terol // Salme-terol // Formo-terol // Arfomo-terol
LAMA = -IUMs
+Glycopyrrolate // Tiotropium // Aclidinium // Umeclidinium
Initial Treatment of Stable COPD
What Group & What Drug(s)?
> 2 Moderate Exacerbations OR > 1 leading to Hospitilization
&
mMRC 0-1 // CAT <10
modified MRC Dyspenea Scale (QOL) // COPD Assessment Test (Symptoms
Group C
- *LAMA = -IUMs**
- *+Glycopyrrolate** // Tiotropium // Aclidinium // Umeclidinium
Initial Treatment of Stable COPD
What Group & What Drug(s)?
> 2 Moderate Exacerbations OR > 1 leading to Hospitilization
&
mMRC > 2 // CAT > 10
modified MRC Dyspenea Scale (QOL) // COPD Assessment Test (Symptoms
Group D
LAMA or LAMA + LABA or ICS + LABA
- *LAMA = -IUMs**
- *+Glycopyrrolate** // Tiotropium // Aclidinium // Umeclidinium
- *LAMA + LABA**
- *-IUMs** + -TEROLs
- *ICS + LABA**
- *-SONE** + -TEROLs
Acute COPD Exacerbation
TREATMENT
Short Burst Corticosteroids
- *PREDNISONE**
- *40mg for 5-7 days**
Improves:
- *spirometry / ABGs / Symptoms**
- reduced RELAPSE rates @ 30 days*
Risk Factors for COPD
Modifiable Risks
- *TOBACCO Smoke**
- *Occupational Dust // Air Pollution**
NON-modifiable Risks
ASTHMA
Impaired lung growth // Infections
Genetics - a1-antitrypsin Deficiency
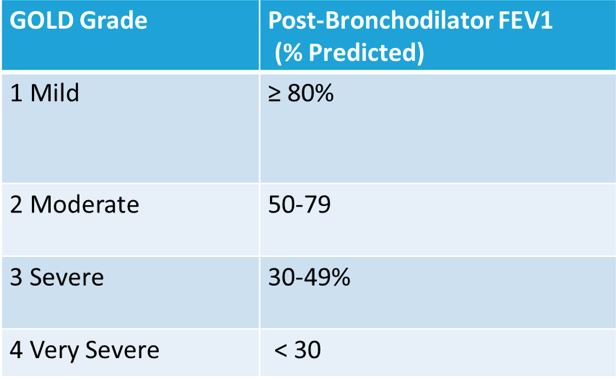
Diagnosis of COPD
SPIROMETRY
- *Symptoms**
- *Cough / Sputum** (Mucus) / Dyspnea SOB
Exposure to Risk Factors
Tobacco / Occupation / Pollution
A-1 Antitrypsin Levels
Assessment of COPD Exacerbation Risk
“Acute Worsening of respiratory symptoms that result in ADDITIONAL THERAPY”
Mild vs Moderate vs SEVERE
- Blood Eosinophil Count** may also _predict_ *exacerbation rates
- -> for those patients treated with LABA w/o ICS
Mild = SABD ONLY
Moderate = SABDs + AntiBiotics +/- Oral Corticosteroids
SEVERE = requires HOSPITILIZATION or visits emergency room
Important Health Maintenance for COPD
IMMUNIZATIONS
Flu Vaccine –> reduces Serious Illness + Death
ALL SMOKERS SHOULD RECEIVE
–> PNEUMOCOCCAL 23 VACCINE
if 65 y/o+ –> prevnar 13 then 1 year for PCV23
SUBQ or IM
Protects against 85% of INVASIVE Pneumococcal strains
Important Health Maintenance for COPD
PULMONARY REHABILITATION
EXERCISE / STRENGTH Training
Education + Adequate Nutrition
Important Health Maintenance for COPD
SMOKING CESSATION
MOST EFFECTIVE intervention STOPS & REDUCES progression of COPD
Varenicline
Renal Dosing, CrCL < 30 = 0.5mg QD, MAX 0.5mg BID
Bupropion SR
150mg f3d –> 150mg BID
CI with SEIZURES – Good for Weight Gain + Depression
Hepatic = 150mg QOD // Elderly or Renal = 150mg QD
- *NRTs**
- not covered by insurance typically*
Albuterol - Levalbuterol
Type / ADR
SABA
Short Acting B2 AGONIST
not completely selective
ADRs:
↑HR & Contraction
HypoKalemia –> leg cramps
Ipratropium
Type / ADRs
SAMA
Short-Acting Muscarinic ANTAGONIST
Atrovent HFA MDI
also comes in inhalation solution - 15 min onset of action
ADR:
DRY MOUTH / ↑CV Events
Metallic taste / Blurred Vision
Urinary Retention / Tachycardia
Which LAMA is considered the GOLD STANDARD?
LAMA = -IUMs + Glycopyrrolate
TIOTROPIUM
Spiriva Respimat
Glycopyrrolate –> Improved FEV1 > Tiotropium
LAMA
Tiotropium / Aclidinium / Umeclidinium / +Glycopyrolate
USES
Effects on Exacerbations?
LAMA
- *PREVENTS_ & _TREATS**
- *Exacerbations**
Relieves symptoms / prevents hospitalizations
LAMA
Tiotropium / Aclidinium / Umeclidinium / +Glycopyrolate
ADR / PRECAUTIONS
ADR’s are the SAME as SAMA = Ipatropium
Dry mouth / blurred vision / constipation / urinary retention / glaucoma
EXCEPT:
does NOT show increase in CV EVENTS
CI:
Glaucoma / Prostatic HYPERplasia / Renal Impairment CrCl <50 mL/min
Combination SABA/SAMA
Advantages
Albuterol + Ipratropium = Combivent
Combo provides greater change in spirometry than either agent alone.
Improved adherence & Cost
disadvantage
FIXED DOSE
Which LABAs are INHALATION SOLUTIONS?
FORMO-TEROL** & **ARFORMO-TEROL
both 1 vial BID
Salmeterol is DPI dosed BID
Which LABAs are
ULTRA-LONG-ACTING
“Dosed DAILY”
- *INDACATEROL**
- *1 CAP for inhalation DAILY,** ArCAPta Neohaler DPI
- *OLODATEROL**
- *2 Inhalers DAILY**, Striverdi Respimat
Salmeterol is DPI dosed BID
LABA = -TEROLs
Indaca-terol // Oloda-terol // Salme-terol // Formo-terol // Arfomo-terol
USES - Effect on exacerbations?
- *Prevent Exacerbations ONLY**
- does NOT TREAT* compared to LAMA
Prevent Hospilizations / Relieve Symptoms
LABA = -TEROLs
Indaca-terol // Oloda-terol // Salme-terol // Formo-terol // Arfomo-terol
SIDE EFFECTS
DPI - DRY COUGH
BLACK BOX WARNING
increased risk of ASTHMA-related deaths
never used ALONE for ASTHMA patients
Insomnia / Tremors / Palpitations
TachyCardia / QT Interval Prolongation / HypoKalemia
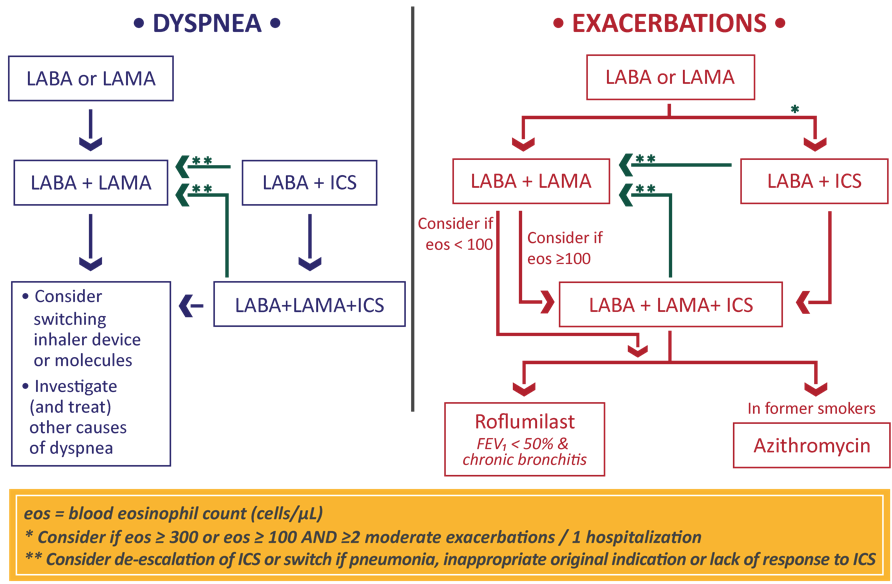
When would we ADD an ICS for COPD?
LABA + ICS
for EXACERBATIONS:
EOS > 300
or EOS > 100 + > 2 moderate exacerbation / 1 hospitilization
Since:
COPD during EXACERBATIONS = EOSINOPHILIC INFLAMMATION
Eosinophils & COPD
COPD is mainly NEUTROPHILIC Inflammation,
EXCEPT:
During EXACERBATIONS –> EOSINOPHLIC
&
pt with ASTHMA + COPD
Eosiniphils are associated with:
↑Risk of COPD exacerbations
↓Lung Function
Which LABA/ICS combination is dosed DAILY?
- *Fluticasone Furoate / Vilanterol**
- *Breo Ellipta DPI**
1 Inhalation DAILY



-
1/2 - Innate & Adaptive Immune System41
-
3 - Antigens22
-
4/5 - Antibodies33
-
6 - B-cell Biology16
-
7 - Complement38
-
8 - MHC39
-
9 - T-Cell Bio39
-
10 - T-Cell38
-
11 - B-Cell30
-
Lec 1-11 - Coico Q's63
-
Week 6 Recitation - Allograft Recognition26
-
12 - Cytokines52
-
13 - Tolerance and Autoimmunity44
-
14 - Hypersensitivity36
-
15 - Drug Allergies49
-
16 - Intro to HIV/AIDS21
-
17 - Immunity to Tumors16
-
18 - Cancer Immunotherapies24
-
19 - Immunity to Pathogens0
-
20 - Immunizations25
-
21 - Immuno Medchem23
-
22/23 - Transplant Therapeutics52
-
24 - DMARDS26
-
25 - Rheumatoid Arthritis46
-
26 - SLE Lupus41
-
27 - Psoriasis53
-
27 - IBD Medchem30
-
29/30 - IBD62
-
31 - MS Medchem15
-
32/33 - MS40
-
34/35 - COPD38
-
36/37/38 - Asthma55
-
39 - Allergic Rhinitis35
-
40 - Pulmonary Medchem40
