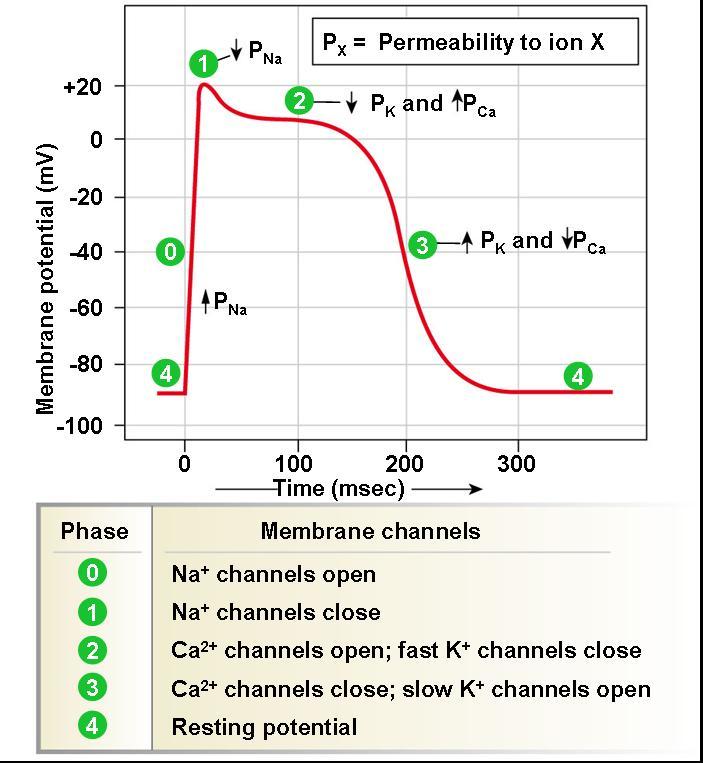
Discuss the phases of the action potential of myocardial cells
Phase 0 - Rapid depolarisation (influx of Na+) Phase 1 - Partial repolarisation (deactivation of Na+ influx and eflux of K+) Phase 2 - Plateau (slow influx of Ca2+, equals the efflux of K+) Phase 3 - Repolarisation (deactivation of Ca2+ influx, K+ eflux) Phase 4 - Pacemaker potential (slow influx of Na+ which slows the eflux of K+, “autorhythmicity”) Refractory period - Phases 1-3
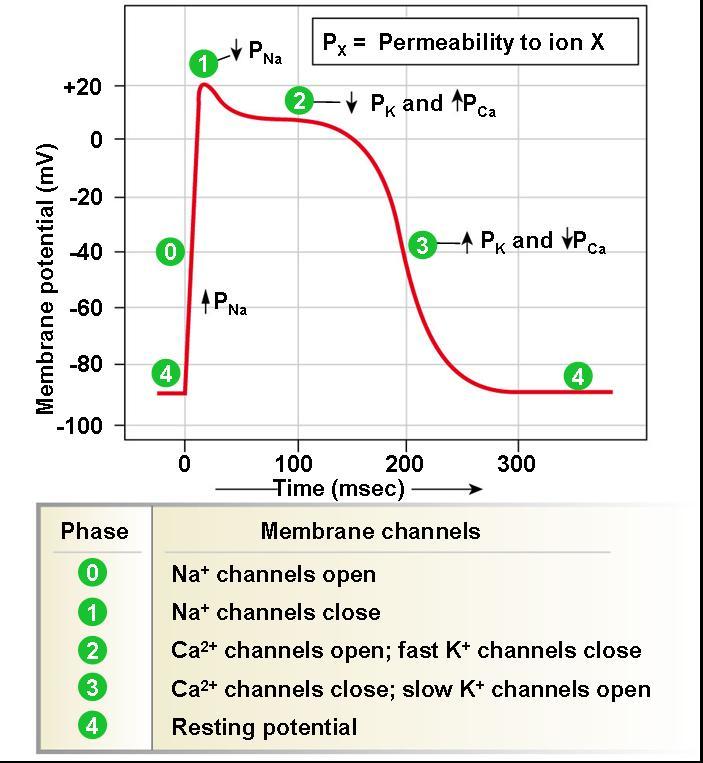
Discuss the sodium cycle in the myocardial cells
-.The sodium pump is responsible for the initiation of the action potential - It is voltage dependant and thus sodium moves rapidly - These channels are open during phase 0, allowing for the rapid influx of sodium ions - This influx causes an increase in the membrane potential4 - As the membrane potential increases the sodium channels close again - During this inactivation state sodium cannot pass through the membrane ( this is relevant for the absolute refractory period phases 1-3)
Discuss the calcium cycle in myocardium cells
.- There is an influx of Calcium in phase 2 which is steady and equals the potassium out, resulting in a plateau - the influx of calcium is largely responsible for contraction of the muscle - there are 2 types of calcium channels T and L type channels - T channels act faster and contribute to depolarisation, phase 0, and L channels are active in phase 2, plateau phase, and allow for a slow influx of calcium
Discuss depolarisation, repolarisation and resting membrane potential of myocardial cells
.Depolarisation - phase 0 (action potential triggered by neighbouring cells through gap junctions, raises transmembrane potential, Fast Na+ channels open and rapid influx of sodium, increasing the voltage of the cell Repolarisation - Early repolarisation in phase 1 as som potassium leaks out of the cell, full repolarisation in phase 3 as the calcium channels are closed and potassium continues to leak out bringing the voltage back down to -90mv
Discuss the absolute, effective and relative refractory periods of myocardial cells as well as supra
.Absolute refractory period (ARP): the cell is completely unexcitable to a new stimulus. Phase 2. Effective refractory period (ERP): ARP + short segment of phase 3 during which a stimulus may cause the cell to depolarize minimally but will not result in a propagated action potential (i.e. neighbouring cells will not depolarize). Relative refractory period (RRP): a greater than normal stimulus will depolarize the cell and cause an action potential. Phase 3. Supranormal period: a hyperexcitable period during which a weaker than normal stimulus will depolarize the cells and cause an action potential. Cells in this phase are particularly susceptible to arrhythmias when exposed to an inappropriately timed stimulus, which is why one must synchronize the electrical stimulus during cardioversion to prevent inducing ventricular fibrillation.
Define axis deviation
The electric axis of the heart is the net direction in which the wave of depolarisation travels.
Discuss how to identify left and right axis deviation
RAD: Lead I - negative avF/III - positive LAD: Lead I - positive avF/III - negative
Discuss the causes of left/right axis deviation
Right axis deviation (RAD): Right ventricular hypertrophy Acute right ventricular strain, e.g. due to pulmonary embolism Lateral STEMI Chronic lung disease, e.g. COPD Hyperkalaemia Sodium-channel blockade, e.g. TCA poisoning Wolff-Parkinson-White syndrome Dextrocardia Ventricular ectopy Secundum ASD – rSR’ pattern Normal paediatric ECG Left posterior fascicular block – diagnosis of exclusion Vertically orientated heart – tall, thin patient Left Axis Deviation (LAD): Left ventricular hypertrophy Left bundle branch block Inferior MI Ventricular pacing /ectopy Wolff-Parkinson-White Syndrome Left anterior fascicular block – diagnosis of exclusion Horizontally orientated heart – short, squat patient Extreme axis deviation: Ventricular rhythms – e.g.VT, AIVR, ventricular ectopy Hyperkalaemia Severe right ventricular hypertrophy
Outline the criteria to identify ST elevation (and lead groupings)
.o ≥2 mm of ST segment elevation in 2 contiguous precordial leads in men (1.5 mm for women) o ≥1mm in other leads (2 contiguous) o An initial Q wave or abnormal R wave develops over a period of several hours to days.
Outline the ECG lead groupings
Inferior - Lead II, III, and avF Lateral - Lead I, avL, V5, V6 Anterior - V3, V4 Septal - V1, V2
Outline the criteria to identify 1st degree block
- PR interval > 200ms (five small squares) - ‘Marked’ first degree block if PR interval > 300ms - P waves buried in preceding T waves
Outline the criteria to identify 2nd degree block (Mobitz I) (Wenckebach)
- Progressive prolongation of the PR interval culminating in a non-conducted P wave - The PR interval is longest immediately before the dropped beat - The PR interval is shortest immediately after the dropped beat
Outline the criteria to identify 3rd degree block ( complete heart block)
- atrial and ventricular pacing is regular but completely unrelated to one another - two seperate, regular rates - .None of the atrial impulses appear to be conducted to the ventricles. - Rhythm is maintained by a junctional escape rhythm.
Outline the criteria to identify supraventricular tachycardia
- P waves are often hidden – being embedded in the QRS complexes. - Pseudo R’ wave may be seen in V1 or V2. - Pseudo S waves may be seen in leads II, III or aVF. - In most cases this results in a ‘typical’ SVT appearance with absent P waves and tachycardia
Outline the criteria to identify left bundle branch block
- QRS duration of > 120 ms - Dominant S wave in V1 - Broad monophasic R wave in lateral leads (I, aVL, V5-V6) - Absence of Q waves in lateral leads (I, - V5-V6; small Q waves are still allowed in aVL) - Prolonged R wave peak time > 60ms in left precordial leads (V5-6) - Appropriate discordance: the ST segments and T waves always go in the opposite direction to the main vector of the QRS complex - Poor R wave progression in the chest leads - Left axis deviation
Outline the criteria to identify right bundle branch block
- Broad QRS > 120 ms - RSR’ pattern in V1-3 (‘M-shaped’ QRS complex) - Wide, slurred S wave in the lateral leads (I, aVL, V5-6)
Outline the criteria to identify left anterior fascicular block (LAFB)
- Left axis deviation (usually between -45 and -90 degrees) - Small Q waves with tall R waves (= ‘qR complexes’) in leads I and aVL - Small R waves with deep S waves (= ‘rS complexes’) in leads II, III, aVF - QRS duration normal or slightly prolonged (80-110 ms) - Prolonged R wave peak time in aVL > 45 ms - Increased QRS voltage in the limb leads
Outline the criteria to identify left posterior fascicular block (LPFB)
- Right axis deviation (> +90 degrees) - Small R waves with deep S waves (= ‘rS complexes’) in leads I and aVL - Small Q waves with tall R waves (= ‘qR complexes’) in leads II, III and aVF - QRS duration normal or slightly prolonged (80-110ms) - Prolonged R wave peak time in aVF - Increased QRS voltage in the limb leads - No evidence of right ventricular hypertrophy - No evidence of any other cause for right axis deviation
Outline the criteria to identify a bifascicular block
- Bifascicular block is the combination of RBBB with either LAFB or LPFB. - Conduction to the ventricles is via the single remaining fascicle. - The ECG will show typical features of RBBB plus either left or right axis deviation. - RBBB + LAFB is the most common of the two patterns.
Outline the criteria to identify a trifascicular block
.Trifascicular block (TFB) refers to the presence of conducting disease in all three fascicles: - Right bundle branch (RBB) - Left anterior fascicle (LAF) - Left posterior fascicle (LPF) The most common is a combination of bifascicular block with 1st degree AV block. Incomplete trifascicular block: - Bifascicular block + 1st degree AV block (most common) - Bifascicular block + 2nd degree AV block - RBBB + alternating LAFB / LPFB Complete trifascicular block: - Bifascicular block + 3rd degree AV block
Outline the criteria to identify wolf parkinson white
- Wolff-Parkinson-White (WPW) Syndrome is a combination of the presence of a congenital accessory pathway and episodes of tachyarrhythmia - PR interval <120ms - Delta wave – slurring slow rise of initial portion of the QRS - QRS prolongation >110ms - ST Segment and T wave discordant changes – i.e. in the opposite direction to the major component of the QRS complex
Outline the criteria to identify an accelerated idioventricular rhythm
- Regular rhythm. - Rate 50-110 bpm. - Three or more ventricular complexes. - QRS complexes >120ms. - Fusion and capture beats.
Outline the criteria to identify accelerated junctional rhythm
- Narrow complex rhythm; QRS duration < 120ms (unless pre-existing bundle branch block or rate-related aberrant conduction). 0
- Ventricular rate usually 60 – 100 bpm.
- Retrograde P waves may be present and can appear before, during or after the QRS complex.
- Retrograde P waves are usually inverted in the inferior leads (II, III, aVF), upright in aVR + V1.
- AV dissociation may be present with the ventricular rate usually greater than the atrial rate.
- There may be associated ECG features of digoxin effect or digoxin toxicity.
Outline the criteria to identify dilated cardiomyopathy
. - The most common ECG abnormalities are those associated with atrial and ventricular hypertrophy — typically, left sided changes are seen but there may be signs of biatrial or biventricular hypertrophy. - Interventricular conduction delays (eg. LBBB) occur due to cardiac dilatation.
-
- HAEMODYNAMIC MONITORING -37
-
- EXTERNAL CARDIAC PACING -12
-
- ADVANCED ECG INTERPRETATION -51
-
DISASTER MANAGEMENT24
-
MENTAL HEALTH21
-
- ACUTE CORONARY SYNDROMES -29
-
ADVANCED LIFE SUPPORT14
-
- ALS DRUGS -30
-
AORTIC ANEURYSMS19
-
SHOCK62
-
ENDOCRINE EMERGENCIES45
-
- RENAL AND GENITOURINARY PRESENTATIONS -34
-
NON-ISCHAEMIC CARDIAC CONDITIONS18
-
PAEDIATRICS53
-
ALCOHOL AND OTHER DRUGS13
-
TEAMWORK AND LEADERSHIP12
-
RASH18
-
- CONCEPTS OF VENTILATION -35
-
- SEDATED AND PARALYSED PATIENT -39
-
- HEART FAILURE -15
-
RESPIRATORY EMERGENCIES38
-
- CXR INTERPRETATION -9
-
- ABG INTERPRETATION -12
-
- CAPNOGRAPHY -6
-
- OXYGEN THERAPY AND NIPPV -26
-
- INHALED ANALGESIA / PROCEDURAL SEDATION -8
-
- PATHOPHYSIOLOGIES -25
