What is anaemia?
Haemoglobin outside the reference range for the normal population.
What are the signs and symptoms of anemia?
Symptoms: shortness of breath tiredness, cardiac failure, palpitations, headache
Signs: pallor, tachycardia, tachypoea, hypotension
What are some specific signs of amemia?
Koilonychia (spoon nails)
Glossitis (inflammation of the tongue)
Oesophageal webs (webs along the oesophagus)
Angual stomatitis (inflammatory condition affecting the corners of the mouth)
Thalassaemia - Abnormal facial bone development.
What is the physiological life cycle of a RBC?
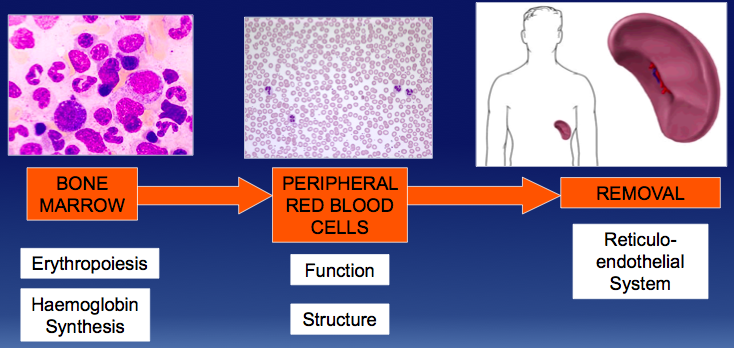
Why might anaemia develop?
Problems with:
- Erythropoiesis
- Haemoglobin synthesis
- Structure of red blood cells
- Metabolism of red blood cells
- Loss of red cells
- reticuloendothelial system
why would a patient have reduced erythropoiesis?
- Erythropoietin not produced by kidneys - This is an example of last of response in a haemostatic loop.
- Empty bone marrow - unable to respond to stimulus from epithropoietin after chemotherapy or toxic insult such as parvovirus infection in aplastic anaemia.
- Marrow infiltrated - by cancer cells or fibrous tissue (myelofibrosis) measn normal haemopoietic cells are reduced.
What is dyserythropoiesis?
This is anaemia of inflammation or anaemia of chronic disease.
Iron is not released for use in the bone marrow which leads to a reduced lifespan of red cells. This means the marrrow shows a lock of response to erythropoietin.
This is seen in renal disease. RA, SLE, inflamatory bowel diesease, or other chronic infections.
What could cause defcts in haemoglobin synthesis?
Deficiencies in things that are essential:
- Lack of iron in haem synthesis - this ieads to iron deficiency or anaemia of chronic disease.
- Lack of B12/folate: deficiencies in the building blocks for DNA synthesis - This leads to megoblastic anaemia.
- Mutations in the portiens encoding the globin chain - This leads to thalassaemia or sickle cell disease.
What inherited defects cause changes in the structure of red cells?
Abnormalities of the proteins making up the red cellmembrane can lead to anaemia.
- Hereditary spherocytosis
- Hereditary eliptocytosis
- Hereditary pyropoikilocytosis
The cells in there conditions are less flexible and are damaged more easy. This means they break up and are removed from circulation.
What can cause aquired defects in the red cell membrane structure?
Mechanical damage to red cells including:
- Heart valves
- Vasculitis
- MAHA (microangiopathies)
- DIC - disseminated intravascular coagulopathy.
Heat damage
- Burns
Osmotic change
- Drowning
How can defects in red cell metabolism lead to anaemia?
Red cell enzyme defects can lead to haemolytic anaemia. The best recognised defects are:
- Glucose-6-phosphate dehydrogenase (an enzyme in pentose phosphate pathway)
- Pyruvate kinase deficiency
How does the reticuloendothelial system lead to anaemia?
The RES removes an excess of damaged red cells.
The spleen removes damaged or defective red cells in a variety of causes of amaemia (membrane, enzyme and Hb disorders). In haemolytic anaemia, red cells are destroyed more quickly as they are abnormal or damaged.
This removal can be intravascular or extravascular.
What are the causes of incresed reticulocytes?
Acute blood loss
Splenic sequestration
Haemolysis (immume or non immune mediated)
What are the causes of low reticulocute count?
Low MCV
TAILS!
High MCV
Vit B12, Folate, Myelodysplasia, Liver disease, Hypothyroidism, Alcohol
Normal MCV
Primacy bone marrow failure (rare) -aplastic anaemia and red cell aplasia
Secondary bone marrow failure - anaemia of chroic disease, Combined haematinic deficiencies, Uraemia, Endocrine abnormalities, HIV infection.
MCV = mean cell volume.
What does vit B12 or folate deficiency cause?
Vitamin B12 and/or folate deficiency causes deficiency in building blocks for DNA synthesis.
The causes megaloblastic anaemia.
This is the most common cause of macrocytic anaemia.
Where is B12 found?
Animal products
- Meat
- Fish
- Eggs
- Cheese
How does B12 get absorbed?
B12 binds with haptacorrin which is secreted by the salivary glands.
The B12-Haptacorrin pretects the B12 in the stomach.
In the stomach, the patietal cells produce HCl and intrinsic factor.
Then, B12 and haptacorrin and intrinsic factor both pass into the small intestine.
In small intestine, haptacorrin B-12 complex breaks apart and the B-12 binds to intrinsic factor.
B-12 intrinsic factor complex move into theterminal ilium.
Here, B-12 is absorbed into the portal blood though the wall and IF gets distroyed.
In the blood, it binds to a protein called transcobalamine II.
This is the mainly stored in the liver then carried to the places required.
How long would body stored of vitamin B-12 last?
We have body stores of B-12 as eat lots of meat, fish eggs and cheese. These stores could last 3-6 years. This means that it takes a long time to become B-12 deficient.
What are the causes of B-12 deficiencies?
- Dietary deficiencies - eg vegan diet or poor diets (alcoholics).
- Lack of intrinsic factor (IF) = Perinicious anemia. This is an autoimmune disease affecting the gastric parietal cells causing lack of intrinsic factor. Also caused if had gastrectomy.
- Disease if the ileum - Crohns disease, ileal resection, tropical sprue.
- Lack of transcobalamin - Congenical deficiency. (Not able to carry from gut to where its needed).
What is folate?
Folate is present in most foods, year, liver and leafy greens are an especially rich source.
Stores can only last for about 3-4 months.
Absorbtion occurs in the duodenum and jejunum.
What could cause folate deficiency?
- Dietary deficiency: Poor diet.
- Increased use: pregnancy, increased erythropoiests e.g. haemolytic anaemias, severe skin diseases e.g. psoriasis or exfoliative dermatitis.
- Diseases of the duodenum or jejunum: proximal small bowel diseased e.g. coeliac disease or Crohns disease.
- Functional folate deficiency causes by lack of methyl THF: dirgs that inhibit dihydrofolate reductase enzyme (e.g. methotrexate) means folate cannot be absorbed.
- Alcoholism
- Urinary loss of folate in liver disease and heart failure
- Other drugs e.g. anticonvulsants
What do B-12 and folate do?
Dietary folates are all converted to methytetrahydrofolate (methylTHF) which is the ‘functional form’
B-12 removes the methy groupt from methylTHF to form THF.
THF is essential for a variety of reactions but, most importantly, it is essential for synthesising thymidylate (thymidine/thymine) which is essential for synthesising DNA.
So, if no B-12, you can’t remove the methyl group and therefore make thymidine.
This means that lack of B-12 results in a functional folate deficiency but lack of folate results in an actual folate deficiency.
Why do B-12 ad folate deficinecy cause megaloblastic anaemia?
- Both folate and B-12 deficiencies lead to thymidylate deficiencies.
- In the absence of thymine, uracil is incorporated into DNA instead.
- DNA repair enzymes detect the error and DNA strands are destroyed.
- This causes asynchronous maturation between the nuceus and the cytoplasm.
- The nucleus (lacking DNA) does not fully mature
- The cytoplasm in which RNA production and haemoglobin synthesis continues, matures at a normal rate.

-
Alcohol Metabolism14
-
Protein And Amino Acid Metabolism51
-
Oxidative Stress29
-
Energy Storage43
-
Lipid Transport42
-
Haemapoesis52
-
Full Blood Count35
-
Anaemia27
-
Haemolytic Anaemia And Haemoglobinopathies21
-
Wrong Haemopoiesis27
-
Haematology In Systemic Disease30
-
Introduction And Apetite Control41
-
From metabolism and micolytic anaemia42
-
HPA Axis and Growth Hormone30
-
Pituitary Disorders25
-
The Endocrine Pancreas30
-
Diabetes20
-
The Adrenal Glands28
-
Adrenal Disorders24
-
The Thyroid Gland57
-
Calcium Regulation and its Role in Clinical Practice31
-
Special Circumstances39
