sinus brady
<50 and symptoms
1) initial resus - id and treat underlying causes IV, monitor, pulse ox and O2, 12 lead EKG
2) persistent brady and sxs (hypotension/shock, AMS, chest pain, acute heart failure, poor perfusion or heart is not working) - atropine 0.5 mg bolus q 3-5min (3.0 mg max) –> transcutaneous pacing OR dopamine or epi infusions –> consult and transvenous pacing
sinus brady can be nl (young, athletes, sleeping elderly), other causes - sick sinus, myocardial ischemia/infarct, osa, hypothyroid, cushings response, meds (bblockers)
- IV glucagon - reverse bblocker or CCB tox
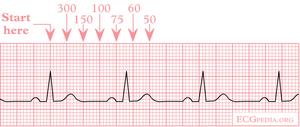
counting rate - see picture
pulmonary HTN
P art pressure > 25 mm Hg at rest (nl < 20 mm Hg)
causes - HF, chronic lung disease, chronic thromboembolism
- primary pulm HTN - women, 40-50s
- treat based on etiology - ACEi and diuretics for HF, O2 and bronchodilators for chronic lung disease
- endothelin antagonists and PDEi for idiopathic PH
- graded exercise traning for all
sick sinus syndrome
SA node dysfunction
- fatigue, lightheadedness, palpitations, pre-syncope/syncope
- brady on EKG, can have brady with alternating tachys
anti-HTNs
ACEi/ARB - post-capillary venodilation
- normalize increased hydrostatic pressure
- angioedema
b-blockers - worsening of CHF, brady, increased airway resistance in asthmatics, generalized fatigue, sexual dysfunction
- OD* - bradycardia, AV block, hypotension, diffuse wheezing
- cardiogenic shock
- other effects - hypoglycemia, broncospasm, delirium, seizures
- tx - 1) IV atropine, 2) IV glucagon (increases intracellular levels of cAMP, helps reverse b-blockers and CCB tox)
CCB - peripheral edema is a common side effect
- preferential dilation of precapillary vessels –> increased capillary hydrostatic pressure –> fluid extravasation into interstitium
- amlodipine and nifedipine > dilt and verapamil
- other side effects - headache, flushing, dizziness
- CCB + ACEi/ARB reduces risk of peripheral edema
digoxin
action - blocks Na/K ATPase (3Na out, 2 K in) …. intracellular Ca increased
- bradyarrhythmias in young
- enhanced automaticity and tachyarrhythmias in elderly (who have underlying cardiac disease)
tox - fatigue, anorexia, nausea, diarrhea, blurred vision and disturbed color perception, arrhythmias (acute GI, chronic neuro and visual sxs)
- arrhythmia - atrial tachy with AV block
- inciting event is a volume depletion event - viral illness, excess diuretic use
- renally cleared, narrow therapeutic index, many DDIs (amiodarone, verapamil, etc.)
- hypokalemia (with loops) - potentiates digoxin
- check level, EKG (r/o arrhythmias)
WPW
px - palpations or (often) asx
depolarization from atria to ventricles that bypasses the AV node (AV node slows heart rate) - short PR (<0.12), wide QRS, delta wave (of QRS)
- if there is retrograde conduction from ventricles to atria –> can get re-entrant SVT
- afib occurs 10-30% of the time –> can deteriorate to afib
- for hemodynamically stable pts - immediately cardiovert
- stable - procainamide
- DONT use AV node blockers (adenosine, bblockers, CCBs, dig) - because this may promote increased conduction across accessory pathway
afib
afib with RVR (no P waves, narrow QRS) - symptoms are due to fast rate (rather than arrhythmia itself)
- ectopic foci is the pulmonary veins - normally cardiac tissue extends into the pulmonary veins and functions like sphincter to prevent backflow
- stable - b-blockers, dilt, verapamil, digoxin for rate control
- if hemodynamically unstable - cardiovert
- attempting cardioversion in pts with afib for unknown duration or for >48hrs without adequate anticoagulation increases risk of TE event
MANAGEMENT: rate vs rhythm control and need for chronic anticoagulation
CHA2DS2-VASc score for risk assessment in nonvalvular AF
- 2 points - age >75, stroke/TIA/TE
- CHF, HTN, DM, vascular disease, age 65-74, female sex
lone AF - afib in a person over 60 (no major heart disease, mild atrial dilation not considered major heart disease), CHA2DS2VASc 0
- risk of embolization is very low and anticoagulation is not needed
score 1 - oral anticoagulant preferred (or ASA) - rivaroxaban
score 2 - warfarin or oral anticoagulants (rivaroxaban, apixaban, dabigatran)
rate control long term - amiodarone, flecainide
IVDA and heart disease
IVDA infective endocarditis
tricuspid regurg - systolic murmur (accentuated with inspiration)
- S aureus is the most common org
- septic embolic - round lesions in lungs, but will have fewer peripheral IE manifestations (like splinter hemorrhages, Janeway lesions)
- conduction abnormalities are uncommon
- another reason you can get tricuspid regurg - complication of implantable pacemaker
- 1 lead in RA, other lead passes through tricuspid and implants in RV
- can lead to damage to tricupsid leaflets –> TR
perivalvular abscess
- aortic regurg (early diastolic murmur), AV conduction block (abscess extending into conduction pathways)
wide complex tachy
AV dissociation, fusion/capture beats?:
yes - Vtach
- 1) stabilize pt
- 2) underlying cause? - electrolyte imbalance (diuretics cause hypoK and hypoMg), digoxin (side effects include arrhythmias, potentiated by hypok)
no - SVT with aberrancy
PAD
majority of patients with intermittent claudication
- 70-80% are stable at 5 yrs, 10-20% have worsening sxs
- 1-2% progress to critical limb ischemia (rest pain, nonhealing ulcer, gangrene)
pts with PAD and intermittent claudication are at high risk for MI and stroke
meds - cilostazol (PDEi, used for pts with intermittent claudication), smoking cessation is first-line tx
RAAS
ang 2 - vasoconstrictor, also promotes aldosterone production
remember feedback loops
decreased renal perfusion in CHF –> SNS RAAS activation
- ang 2 causes vasoconstriction of afferent and efferent arterioles –> increased renal vascular resistance –> decreased RBF
- preferential vasoconstriction of efferent renal arterioles to maintain GFR - increases intraglomerular pressure
- stimulation of Na reabsorption in proximal tubules and aldosterone secretion - decreased Na delivery to distal tubule
paroxysmal SVT
narrow complex tachy
- use adenosine to slow AV node conduction and interrupt re-entrant rhythm
- adenosine short acting
- can use carotid sinus massage - slows AV node
amiodarone
class 3 antiarrhythmic - used for ventricular arrhythmias, can also be used for pts with afib with LV systolic dysfunction
Side effects
cardiac - sinus brady, heart block, QT long and torsads
pulm - chronic interstitial pneumonitis (within mo - cough, fever, dyspnea, pulmonary infiltrates, restrictive lung disease)
endo - high or low thyroid
GI/hepatic - elevated transaminases, hepatitis
ocular - corneal microdeposits, optic neuropathy
derm - blue-gray skin
neuro - p neuroapthy
shock
low MvO2 when there is high CO - because of hyperdynamic circulation and inability of tissues to adequately extract to O2
septic shock - elderly with septic shock will NOT mount a fever
decreased cardiac afterload means low SVR
neurogenic shock - bradycardia
systolic heart failure
Chronic/clinic pxs
dilated cardiomyopathy - myocardial damage by toxic, metabolic, and/or infectious agents
- viral myocarditis (Coxsackie B)
- due to alcohol consumption (doe) - stop alcohol, LV function will normalize over time
- tx - supportive
concentric hypertrophy - due to increased afterload
eccentric hypertrophy - due to increased volume
Acute decompensated HF
- diuretics, inotropes
- avoid b-blockers - can worsen HF
Long-term management - b-blockers, ACEis/ARBs, spironolactone, and hydralazine + nitrates (in AAs) have shown mortality benefits in LV systolic dysfunction
rheumatic heart disease
immigrants
mitral stenosis - loud S1, mid-diastolic rumble, increased LA pressure
- sxs are usu precipitated by conditions that cause tachy (exercise, fever, anemia, pregnancy)
- OS and low pitched diastolic rumble (apex, pt lying on left in held expiration)
- over the course of years – L atrial enlargement –> L mainstem bronchus displacement, compression of recurrent laryngeal nerve, cough, hoarseness
- CHF sxs, afib, thromboembolism
- afib causes a lack of atrial kick - acute worsening of mitral stenosis
- mimics can be ILD (reticular or nodular markings on CXR)
aortic stenosis or insufficiency - occurs but less frequently
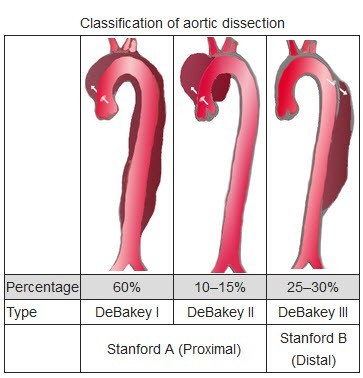
aortic dissection
RFs - HTN, Marfans (young pts), cocaine
features - sharp tearing back pain, >20 mm Hg BP variation in between arms
- may not present classically - look for chest/neck pain, syncope, mediastinal widening
- many pts have sudden spike in BP that is associated with dissection
complications - stroke (carotid arteries)
- acute aortic regurg
- Horners
- acute MI/ischemia (coronary artery)
- pericardial effusion/cardiac tamponade - ascending aortic rupture into pericardial space (type A, surgical emergency) –> if pt was in cardiac tamponade/cardiogenic shock - urgent pericardiocentesis
- hemothorax
- LE weakness/ischemia (spinal or common iliacs)
- abd pain (mesenteric artery)
dx - CT angio in stable pts
- TEE in pts with hemodynamic instability or renal insufficiency
tx - pain control (morphine), IV b-blockers (labetalol, reduce SBP to 100-120, benefits of b-blocker include HR and contractility reduction), sodium nitroprusside for SBP > 120 (vasodilator), urgent surgical repair for ascending dissection
- note hydralazine is a vasodilator like Na nitroprusside - can cause reflex sympathetic tachy
syncope
syncope = LOC with loss of postural tone, followed by spont and complete recovery
vasovagal (neurally mediated) - nausea, diaphoresis, pallor, young women
- prodrome
- occurs in response to stress, pain, urination
- clinical dx
- tx - reassurance, avoidance of triggers, counterpressure techniques for recurrent episodes (supine position with leg raising, leg crossing with tensing of muscles, hand grip and clenched fists all increase venous return
exertional syncope - v arrhythmias, LVOT (blood flow obstruction)
- pts with fixed LVOT cant increase CO in response to exercise-induced vasodilation –> hypotension, cerebral hypoperfusion
- for valvular obstruction - preceding hx of exertional dyspnea, chest pain, fatigue
orthostatic hypotension - elderly, autonomic neuropathy, hypovolemic, diuretics, vasodilators, adrenergic-blockers, prolonged recumbence
carotid sinus hypersensivity - carotid sinus massage with reproduce the sxs
situational - triggers are cough, micturition, defecation
- prodrome
- alteration of autonomic response –> cardioinhibitory, vasodepressor, or mixed response
- increased PS tone (bradyarrhythmia), decreased SNS tone (vasodil, hypotension, syncope)
sick sinus syndrome, bradyarrhythmias, AV block - sinus pauses, long PR or long QRS
Torsades (acquired long QT) - hypokalemia, hypoMg, meds
- congenital long QT - FHx of sudden death, long QT with triggers (exercise, startle, sleeping)
CHF
signs - bibasilar crackles, pleural effusions (decreased breath sounds), wheezing (cardiac asthma)
BNP - elevated BNP, sensitivity >90% of heart failure (>400 pg/ml maybe 500 pg/ml rules in, <100 rules out)
- for systolic and diastolic HF
- can also get PCWP
physical exam findings - low sensivity
myocardial ischemia/infarct
- angina - stable and unstable
- MI and treatment
- complications
Stable angina - px - can occur with strong emotion
- triad: substernal, worse with exercise (or emotion), relieved with rest (or nitro) (atypical is 2/3 characteristics)
- ACS - S4 can be heard in most pts during acute MI or in ischemia-induced myocardial dysfunction
- RFs - CAD (SLE leads to accelerated atherosclerosis)
- prinzmetal angina - young pts, cigarette smoking is known RF, occurs at rest or during sleep, spont resolution in <15 min; ambulatory EKG will show ST elevation; tx with CCB and sublinguinal nitro
- dilt is a potent coronary vasodilator (weak systemic vasodilator)
- avoid ASA in pts with vasospastic angina - ASA inhbits prostacyclin production, worsens vasospasm (same with non-selective b-blockers like propranolol)
Stress testing
- EKG - want pt to reach tHR of 85% of 220-age (contraindicated in LBBB, pacemaker)
- dobutamine stress echo - B1 agonist, increases HR and BP, use in reactive airway disease, DONT use in tachyarrhythmias
- EKG and dobutamine - increased myocardial demand
- pharm stress test with adenosine and dipyridamole - dilates coronary arteries with no increase in HR or BP (NOT for pts with reactive airway disease or pts on dipyridamole or theophylilne)
- blood flow in stenosed arteries does not increase as much as blood flow in normal arteries - difference in blood flow ~ ischemia (this is also the closest to the physiologic mechanism for angina)
Coronary angio for pts with high pre-test probability - men 40+ or women 60+ with typical angina
- and as a f/u to pts with high risk findings on stress testing
Meds
- b-blockers - first- line, decreases contractility and HR (O2 demand), alternative is nondihydropyridine CCBs (verapamil, dilt)
- dihydropyridine CCBs - add if needed, coronary artery vasodilation, decreased afterload by systemic vasodilation (monotherapy can result in reflex tachy)
- (long-acting) nitrates - decreased preload (dilates veins, decreased myocardial O2 demand), sx relief is immediate
- ranolazine - for refractory angina, decreased myocardial calcium influx
*********************************************************************
MI
first signs are T wave inversions
- trops dont rise fro 6-12hrs
immediate steps
1) restoration of coronary blood flow - PCI or fibrinolysis (goals are PCI within 90 min or 120 min if transfer is required), M&M benefits
Types
STEMI:
- inferior MI* - inferior leads are 2, 3, AVF
- -* RCA occlusion - 50% chance of involving the RV –> impaired RV filling –> hypotension and autonomic signs (diaphoresis, vomiting, increased vagal tone can lead to transient brady or AV block)
- avoid nitroglycerin (and diuretics and opiates) - venodilates –> will decrease preload and lead to profound hypotension
- JVD will be low - nl < 3cm
- give NS bolus (then inotropes)
Management - dual antiplt therapy (ASA and clopidrogrel), statin, anticoagulation, urgent revascularization
- PCI - within 12hrs of sx onset, 90 min from first medical contact
- O2, nitrates (caution in pts with hypotension, RV infarct, or severe aortic stenosis)
- following MI - ventricular remodeling occurs –> dilatation of LV and thinning of ventricular walls - ACEi have been shown to limit remodeling
–> start ACEi within 24hrs of MI
- statin therapy (possibly beta-blockers) - long-term management
Complications
stent thrombosis - localized ST elevation
- pt has to take ASA and plavix even if they have a drug-eluting stent placed
IV rupture vs free wall rupture - IV rupture will have holosystolic murmur at left sternal border, free wall rupture can present with PEA (low voltage EKG)
papillary muscle rupture and acute MR (can occur with inferior infarct) - murmur at apex
ventricular aneurysm - weeks-mo, will see localized ST elevation and deep q waves
- may present with HF, refractory angina, arrhythmias, embolism
acute pericarditis (in general, not just post-MI) - viral, idiopathic, uremia, autoimmune, early post-MI (risk factor is delayed coronary reperfusion), late post- MI (Dressler, weeks, elevated ESR)
- pericardial friction, diffuse ST elevation and PR deprssion (can have depression in aVR), pericardial effusion
- tx
- early post-MI - supportive, avoid anti-inflammatories (will disrupt collagen deposition…)
- late, Dressler - NSAIDs
- viral - NSAIDs and colcichine
pericarditis
diffuse ST elevation, positional pain
causes - viral (most common), bacterial
- surgery, trauma, radiation, drugs
- CT disease - RA, SLE
- Cardiac - Dressler
- uremic - BUN >60 (but degree of pericarditis does not always correlate with degree of elevation), doesnt have classic EKG findings, tx dialysis
- malignancy - cancer or chemorads
- for idiopathic or viral - NSAIDs and colchicine
pericardial effusion secondary to pericarditis (preceding URI, etc.)
- hypotension, syncope (decreased CO)
- tachy, distended neck veins, pulsus paradoxus, muffled heart sounds
- electrical alternans - variation in QRS amplitudes = specific not sensitive
- dx/tx 1) echo (if stable), 2) pericardiocentesis
cardiac tamponade
Becks triad: hypotension, elevated JVP, muffled heart sounds
large pericardial effusion - most often occurs from a viral illness (other causes include post-MI, trauma, uremia, autoimmune diseases, hypothyroidism)
- volume overload, clear lung fields, water bottle heart - inability to palpate PMI
- distinguishing between viral myocarditis - pts will have an audible S3 and pulmonary vascular congestion
hypertriglyceridemia
causes - familial, DM, obesity, hypothryoid, nephrotic syndrome, alcohol abuse
150-500
- lifestyle modifications (weight loss, moderate alcohol intake, exercise)
- add high-intensity statin for pts are high risk of CVD
>1000 - initial goal is pancreatitis prevention
- fibrates, fish oil, abstinence from alcohol
- fibrates are the most effective pharmacotherapy for lower TG levels - have increased adverse effects and no proven CV benefit (so they are not first line like statins)
statin: HMG-CoA reductase inhibitor - RLS, inhibits intracellular biosynthesis of cholesterol - decreased hepatic cholesterol –> activates LDL receptors on liver cell membranes –> circulating LDL is removed
- adverse effects - mild transaminitis, myalgias (2-10%)
- when to start statin - for 10 yr-ASCVD risk >7.5 (or pts with known MI, stroke, DM, CKD, or LDL > 190 indicative of familial hypercholesterolemia)
- high intensity v low depends on age and % risk
vitamin supplementation - has NOT demonstrated a benefit in lipid disorders of CVD
niacin - side effects are cutaneous flushing and generalized pruritis (usu improve in 2-4wks of therapy) - due to PG-induced vasodilation
- often prescribed with low dose ASA - counteracts PG-induced vasodilation
- used in hypertriglyceridemia
murmur and maneuvers
Manuevers
valsalva, standing, nitro - decrease preload
- HCM and MVP get louder with valsalva and standing, softer with other maneuvers
sustained hand grip - increases after load
squatting - increases afterload and preload
passive leg raise - increases preload
diastolic and continuous murmurs are always pathologic - get echo
- mid-systolic murmur by itself is benign in healthy, young adults
HCM - AD, sarcomere gene mutations, offer genetic testing to first degree relatives
- exertional sxs
- crescendo-decrescendo murmurs, biphasic pulse
- mitral valve leaflet moves abnormally and contacts thickened anterior septum –> LVOT
- EKG - LVH (tall R in aVL + deep S in V3), repolarization changes in anterolateral leads (1, avL, V4-V6)
bicuspid aortic valve
- ejection click and mid-systolic murmur
aortic stenosis - prolonged asx period, can present with syncope
- delayed carotid pulse (pulsus parvus and tardus)
- mid-late peaking systolic mumur that radiates to carotids - the later the murmur, the more severe the aortic stenosis
- soft single S2 - due to reduced mobility of aortic valve that closes at the same as the P2 (loud S2 is due to sudden aortic valve)
- most common causes - senile calcific (70 yo), biscuspid aortic valve, rheumatic disease
aortic regurg - causes are aortic root dilation (Marfans, syphilis), post-inflammatory, congenital biscupid aortic valve (fhx, will cause AR in young pts and aortic stenosis in older pts)
- best heard with expiration and leaning foward, waterhammer pulses, diastolic decrescendo murmur
- when it is due to root disease - best heard on RSB
- when it is due to valve disease - best heard on LSB
mitral stenosis - age-related calcification, asx or diastolic rumble
- rheumatic heart disease
- chronic mitral stenosis - RVH secondary to pulmonary HTN mitral regurg
- holosystolic, radiates to L axilla, loud S1
- decreases with decreased preload
MVP - myxomatous degeneration of mitral valve
- non-specific sxs - atypical CP, panic disorder…
- nonejection click and mid-to-late systolic murmur - murmur disappears with squatting - when LV is more filled –> delay in prolapse of valve
VSD - holosystolic murmurs
pulmonic stenosis - congenital (rarely acquired)
- severe will present in childhood, mild in adulthood
- crescendo-decresendo murmur that increases with inspiration (very specific for R-sided murmurs) (ASD is wide and fixed split S2)
- dx with echo
- tx - perc balloon valvulotomy, sometimes surgical repair


