What’s penetrance?
Penetrance - proportion of people with particular genetic change (mutation) who exhibit signs
and symptoms of a genetic disorder
*if some people with the mutation do not exhibit particular features of a disorder -> incomplete
penetrance
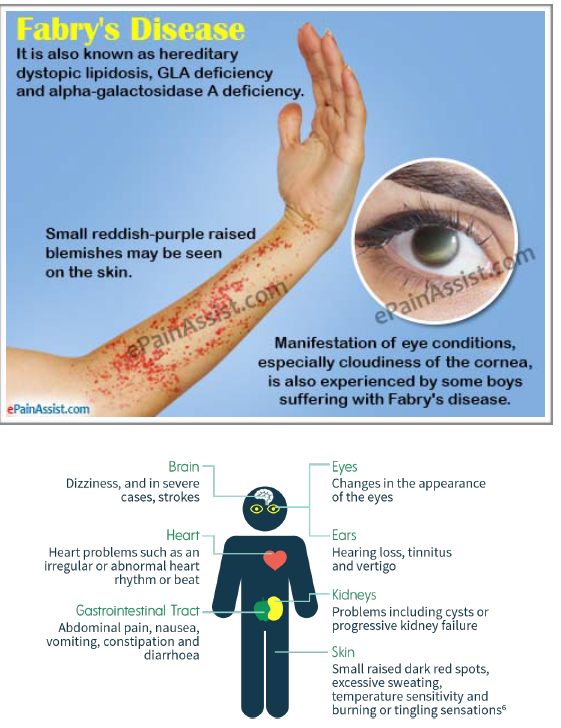
Genetics behind Fabry’s disease
- deficiency of enzyme alpha-galactosidase A -> part of group of lysosomal storage disease
- hereditary - gene for the enzyme located in X chromosome
- X-linked manner
- affects many organs: skin, heart, kidneys
Pathology of Fabry’s disease
Pathology: enzyme alpha - galactosidase A deficiency -> sphingolipids cannot be
processed -> intracellular accumulation of sphingolipids (biomolecules) in the walls of the
vessels and organs
Treatment of Fabry’s disease
• Replacement of an enzyme -> not a cure but can prevent progression of the disease and
potentially reverse some symptoms
- Trials for gene therapy are undergoing
- Treatment of pain associated with Farby’s disease -> analgesics, anticonvulsants
- Kidney failure -> haemodialysis
- Cardiac complications e.g. arrhythmias -> pacemakers, implantable cardioverter-defibrillator
- Diuretics for restrictive cardiomyopathy
Investigations for Fabry’s disease (2)
- blood test -> measures the activity of alpha-galactosidase A
- genetic testing
Signs (auscultation) of cardiomyopathy
*murmur is crescendo-decrescendo (similar to the one in aortic stenosis) > intensity may change (depends how big the obstruction is
* two pulses (bifid pulse) > mitral valve moving towards enlarged wall of septum > blockage to the outflow tract in mid systole
* often S4 sound heard > as blood from atria goes towards stiff ventricle
Treatment of cardiomyopathy
*what med is contraindicated
Medications: beta blockers > to slow down HR; Ca channel blockers (if Beta blockers ineffective)
* Digoxin should not be used (as it increases force of contraction > more obstruction would be induced)
• Surgery
What’s Marfan Syndrome (in general)
- genetic disorder of connective tissue
- autosomal dominant
- affects: eyes, joints, heart and blood vessels, lungs, skeleton
Fibrillin
- what’s that
- role
Physiology:
- microfibrils for connective tissue (giving it strength and integrity)
- fibrillin ~ main component of microfibrils
Roles of fibrilin:
• fibrilin sometimes serves as a connector to the elastin (being laid between different
microfibrils)
Tissues with elastin: arteries, skin and lungs
Tissues without elastin: tendons, ciliary zonules (holds lens of eyes in place) > less stretcheble
• regualation of tissue growth: as it removes TGFbeta (which stimulates tissue growth) ~
so regulation of TGF beta availability for stimulation of growth
Pathology of Marfan Syndrome
- Autosomal dominant mutation of fibrillin1 gene (chromosome 15) > fibrilin 1 protein is dysfunctional or less abundant > less functioning microfibrils > less tissue integrity and elasticity
- Result:
• less/dysfunctional fibrilin > as affects connective tissue > it can affect every body
system
• TGF beta is not suppressed > excessive tissue growth
What’s Marfanoid Body Habitus?
Marfanoid body habitus ~ characteristic physical appearance:
tall, long limbs, thin and long fingers and toes (arachnodactyly), chest abnormalities,
scoliosis, inability to extend the elbow fully, flexible joints, slant eyes /skosne/,
narrow palate (teeth are crowded)
Organ-specific features of Marfan syndrome
- skin
- lungs
- eyes
- skin: stretch marks
- lungs: bulla > pneumothorax (large spaces replace normal lung architecture > lung collapse)
- eyes: risk factor for retinal detachment and lens dislocation
Cardio-vascular features of Marfan Syndrome
- aortic dilation > aortic valve insufficiency > blood back to the L ventricle during diastole
- cystic medial necrosis of aorta > degeneration of tunica media (central portion of aortic wall)
The above weakens the aorta > prone to aneurysm/dissection/rupture > may be fatal
- mitral valve prolapse: mitral valve pouches into the L atrium during systole
Management of Marfan Syndrome
A. No treatment
B. Symptoms treatment:
e.g. dislocated lens > replaced by artificial one
Aorta:
- surgical repair of aorta (to prevent rupture)
- Beta blockers ~ to slow aortic dilation
- Angiotensin receptor blocker
What are the commonest CHD in Down’s syndrome?
40% of newborns with Down’s syndrome have Congenital Heart Disease
- 80% of those have atrioventricular septal defect or ventricular septal defect
- mitral valve problems -> common as people age
- possible TOF and patent ductus arteriosus
