A patient has malar flush and rumbling mid-diastolic murmur (loudest on exp on left side). What is the Dx?
Mitral stenosis
Pan systolic murmur following MI with features of heart failure - what is the murmur?
Mitral regurgitation - due to ischaemic to papillary muscles
Most common heart defect in Down’s?
AVSD (others - VSD, ASD, PDA, ToF)
How does a thrombolytic/fibrinolytic agent work? What different types exist?
Plasminogen activators - dissolve IV clots to Tx acute MI, DVT/PE, acute ischaemic stroke, occlusion of indwelling catheter etc.
During thrombosis platelets activate prothrombin to form thrombin. This converts fibrinogen to fibrin forming a matrix.
This is counterbalanced by plasmin derived from plasminogen. tPA is a natural fibrinolytic in epithelial cells. All thrombolytic agents are proteases cleaving plasminogen to plasmin.
Agent types:
1. Fibrin-specifc agents - need fibrin present for conversion and work best for STEMI/PE/acute ischaemic stroke. E.g. alteplase
2. Non-fibrin-specific agents - act systemically as don’t require fibrin present e.g. streptokinase (less efficacy but reduced risk of IC haemorrhage, increased risk of allergy, no repeat use for 6 months), urokinase (used for indwelling catheters/PV thrombosis)
TXA can be used to reverse action of these agents.

ECG findings based on electrolyte abn?
K:
* Hyperkalaemia - ECG tall tented T-waves, wide QRS, prolonged PR - causes cardiac toxicity/muscle weakness - caused by drugs (k-sparing diuretics, ACEi/ARB, digoxin), Addison’s.
* Hypokalaemia - ECG U-waves (V2/3), T-waves wide/flat, ST depression - causes muscle weakness/resp failure - caused by diarrhoea/vom, malnutrition, aldosteronism, drugs (insulin, corticosteroids)
Ca:
* Hypercalcaemia - ECG short ST, wide T-wave - causes thrones, stones, bones, grones, and psychic moans - caused by primary hyperparathryoidism, malignancy
* Hypocalcaemia - long ST, long QT - causes neuro Sx - caused by pancreatitis, rhabdomyolysis etc
Na - no effect on ECG:
* Hypernatremia - causes thirst/neuro Sx - caused by dehydration, diabetes insipidus, hyperaldosteronism
* Hyponatremia - causes neuro Sx - caused by diuretics, SIADH, heart/liver/renal disease, diarrhoea

Summarise ACS guidelines
- For all ACS (STEMI/NSTEMI/UA) - give aspirin life-long
- STEMI within 12hrs Sx-onset & can do PCI within 120 mins - corronary angio + PCI, if not:
- If within 12hrs - fibrinolysis
- If not within 12hrs but myocardial ischaemia/cardio shock - angio
- Otherwise add Ticagrelor (Clopidogrel if high bleed risk)
- After angio add prasugrel (if no previous anticoag, otherwise clopi), if done via radial route give unfr heparin, femoral give bivalirudin (either with bailout GPI) - NSTEMI/UA - give fondaparinux (if low bleed risk, CR >265 consider unfr heparin) –> do GRACE/HEART score:
- If low risk add Ticagrelor
- If high risk/young for angio - Secondary prevention - ACEi, DAPT (12m), B-blocker (12m or forever if rLVEF, if CI for diltiazem/verapamil), Statin
- IF heart failure with rLVEF start aldosterone antag e.g. spironolactone (3-14d post-MI, after ACEi)
Give an overview of pericarditis
- Inflam of pericardium
- Acute form - new onset inflam lasting under 6-weeks
- Triad - chest pain, pericardial friction rub on auscultation, ECG widespread ST elevation (other Ix - bloods inflam, echo - pericardial effusion)
- Tx - NSAIDs + Colchicine
- Complications - recurrence, tamponade, constrictive pericarditis
Give an overview of aortic dissection
- Seperation in aortic wall intima –> blood flow into false channel (inner & outer layers of media)
- > 50yrs, sudden tearing substernal/intrascapular pain (+/- syncope, heart/renal failure, mesenteric/limb ischaemia)
- Ix with CT/MRI/ECHO
- If ascending aorta/arch - URGENT repair, otherwise b-blocker (or surgery if complicated), needs lifelong surveillance
After how long do trop levels peak after MI? Other causes of raised trop?
- rise 2-4hrs, peak 18-24hrs, last several days
- PE, other heart issue, renal failure, sepsis, rhabdomyolysis
Driving rules for MI
- Cease for 1wk if - successful angioplasty (incl in STEMI)/PPM-insertion
- Cease 4wk if - CABG/MI
- Cease completely if unstable angina uncontrolled
- Notify DVLA if AAA ≥6cm (disqualified if ≥6.5cm) or arrythmia (incapacitated)
Other to note - no sex for 1/12, return to work after 2/12 (stop if pilot/air traffic control)
ECG changes depending on STEMI location? How long for ECG changes to resolve?
Lateral leads - left circumflex/LAD
Inferior leads (or posterior) - RCA/LCx
Anterior/septal - LAD
ST-T changes resolve in days-weeks (longer if ischaemia causes infarction)
QRS including pathological Q-wave - PERMANENT

What are the complications of MI by time period after the event?
- Arrythmias - VF/VT (20%), AF (15%)
- Ischaemia (high CK) - re-occlusion, postinfarct angina –> angio + corronary revasc
- Mechanical:
- LVSD/HF - Killip’s classification (severity of HF post-MI)
- 24h-7d: 1) Ventricular septal - angina/pul oedema, new pansystolic murmur LLSB -> surgery. 2) free wall rupture - bleeding into pericardium (-> tamponade) -> needs pericardiocentesis/surgery
NOTE: pseudoaneurysm = contained left ventricular free walk rupture - Acute MR (normally inf/posterior infarct from isch/necrosis/papillary muscle rupture) = pansystolic murmur
- L. vent aneurysm, R vent failure, L vent outflow obstruction
- Inflammatory - Dressler’s syndrome (pericarditis) - 2-4wks post-MI - self-limiting fever + pericardial/pleural pain –> Tx with NSAIDS/steroids/drainage
- Systemic - PE/DVT, mural thrombosis & systemic embolism
- Depression - suicide

Give an overview of chronic heart failure
Classification:
- LVEF (<40 low, 41-49 mild, 50 preserved)
- NYHC (1 - no limit on physical activity, 2 - slight, 3 - marked, 4 - Sx at rest)
NT-proBNP > 2000 - 2wk referral/echo, 400-2000 - 6wk referral/echo

Acute heart failure findings on CXR? Ix? Mx?
- Bat wing opacities 2. Kerley B lines 3. Cardiomegaly 4. Dilated upper lobe vessels 5. Pleural effusion
Sit upright and 15L NRM, consider IV dia/morphine, Furosemide IV (x2 oral dose), GTN IV 0.5mg/hr (only if BP >90), consider CPAP/NIV if acidotic
If BNP > 100 or NT-proBNP > 300 transthoracic echo
Acute severe MR - surgical replacement
Critical AS - surgical replacement/TAVI
LVSD - ACEi, Aldosterone antag, B-blocker (d/c after stable for 48hrs)
Hypertension Management
BP in clinic >140/90 —> repeat (both arms should be measured if >15 repeat then use measurement in higher arm)
BP 140/90-180/120 - AMBM (ambulatory - 2 measurements/hr requiring 14 measurements)/HBPM (Home - x2 measurements daily for 4-7d, discard 1st day) to confirm Dx
>180/120 with retinal haemorrhage/papilloedema/Sx - same day specialist R/V
Classification:
1 >140/90 with AMBM 135/85
2 >160/100 with AMBM 150/95
3 >180/120
Accelerated/malignant = signs of retinal haemorrhage/papilloedema
?secondary cause of HTN if: <40yrs, Low Na/High K, eGFR <60, Pro/Blood in urine
Most common secondary cause: Renal

Signs of cardiac tamponade? Possible ECG findings? Tx?
- Beck’s triad - JVP, low BP, reduced HS
- Pulsus paradoxus - >12mmHg/9% normal insp decrease in SBP (also caused by const pericarditis, restrictive CMO, severe obs pul disease, PE)
- Kussmaul sign - increased venous pressure/distension on inspiration
- Ewart/Pins sign - if large pericardial effusion, dullness/bronchial breath sounds/bronchophony below angle L scapula
ECG - sinus tachy, low voltage QRS, electrical alternans, PR segment depression
Pericardiocentesis
Mx of stable angina?
- B-Blocker and/or CCB (amlodipine/nifedipine)
- Add/switch to long-acting nitrate/nicorandil (risk of ulceration)
- Ivabradine/Ranolazine
Secondary prevention: consider Aspirin, Statins, ACEi
Cardiac tamponade - key finding on exam? Triad? Mx?
Pulsus paradoxus - BP variation between inspiration & expiration (≥10)
Beck’s triad (50%):
- Raised JVP
- Muffled heart sounds
- Hypotension
Mx:
- IV fluids (RV filling depends on venous pressure & effusion is constricting)
- Echo –> refer to cardiology for pericardiocentesis
- Coagulation profile (to prep for pericardiocentesis)
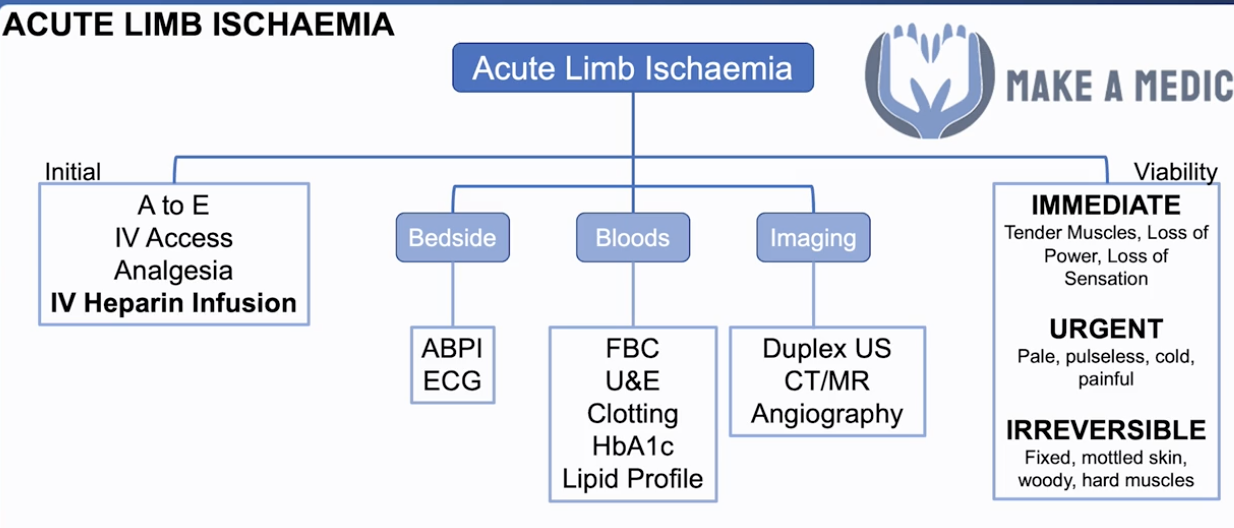
Acute limb ischaemia - Def? Presentation? Ix? Mx?
- Def: a sudden decrease in limb perfusion that threatens the viability of limb
- AF = major RF for acute limb ischemia
- Presentation - 6Ps:
- Pale
- Pulseless
- Painful
- Perishingly cold
- NOTE: need immediate vascularisation (<6hrs) if:
- Paralysis
- Paraesthesia (esp worrying)
- Ix (after initial Mx):
- Bedside: ABPI (PAD), ECG (AF)
- Bloods: FBC, U&E, clotting, HbA1c, lipid profile
- Imaging: duplex USS, CT/MR angiography
- Mx:
- Initial:
- A-E, IV access, analgesia
- IV heparin infusion - reduces the chance of the clot getting worse
- Limb viability:
- Immediate - tender muscles, loss of power, loss of sensation
- Urgent - pale, pulseless, painful, cold
- Irreversible - fixed, mottled skin, woody, hard muscles
- Refer to vascular surgery:
- Thrombotic - local intra-arterial thrombolysis, angioplasty, bypass
- Embolic - embolectomy/local intra-arterial thrombolysis/bypass
- Initial:
Peripheral vascular (arterial) disease - Def? RFs? Spectrum? Ix? Special test?
Def: limb ischemia (chronic) from atherosclerosis in lower limb vasculature
RFs: male, older, smoker, HTN, DM
Spectrum:
- Intermittent claudication (mild) - cramping leg pain after walking (& have to stop) + relieved by rest
- NOTE: the equivalent of stable angina (worse on exertion)
- Worse going uphill/upstairs
- Critical limb ischemia (severe) - ulcers, gangrene, night pain & rest pain
- NOTE: the equivalent of unstable angina (present at rest)
Ix:
- Bedside:
- Exam special test = Buerger’s angle - elevation pallor –> sudden drop feet down = sunset sign
- exercise-treadmill ABPI (ankle-brachial pressure index) - <0.8 (<0.3 = CLI)
- Bloods - FBC, U&E, LFTs, CRP, clotting
- Imaging:
- Arterial duplex USS
- CT/MR angiography
Mx: dealt with by vascular surgeons –> optimise meds + surgery (bypass)
- Conservative: smoking cessation
- Medical: ACEi, clopidogrel, statin, DM control
- Surgery: angioplasty/stent/bypass graft/amputation
Chronic venous insufficiency & varicose veins - presentation? Ix? Mx? Complications of varicose veins?
Presentation:
- Oedema, haemosiderin deposition, lipodermatosclerosis (inverted-champagne bottle), eczema, venous ulcers
- Varicose veins - dilated tortuous, superficial veins
- Pain, swelling, itching, restless legs, cramps
- Feel for thrombosis (hard = thrombophlebitis)
- Cough impulse at SFJ (for Saphena Varix - dilation of saphenous vein @junction w/ femoral vein)
- Trendelenburg test
- Lying flat, lift up leg & empty veins
- Compression over SFJ –> stand up (maintain pressure) - if do not fill = competent valves below SFJ
- If do fill = incompetent valves below SFJ (blood flow from deep to superficial vein via perforating veins)
- Repeat with pressure lower down until filling stops
- Perthe’s test - apply tourniquet to mid-thigh + walk for 5-mins –> compresses superficial vein
- Less distended - normal deep veins as calf compression pushes blood into deep venous system
- Remain distended - impaired deep veins
- Doppler US for reflux
- Warfarin - previous DVT
- Abdo mass with compression
Ix: duplex USS (allow DVT to be ruled out)
Venous insufficiency Mx:
- ABPI > 0.8 –> Compression bandaging
- Varicose veins:
- Conservative - weight loss, avoid standing for prolonged periods
- Minimally invasive procedures - injection sclerotherapy, endovenous radiofrequency ablation
- Surgical - vein ligation
Varicose Veins complications:
- thrombophlebitis - Tx for superficial: NSAIDs
- Eczema
- Bleeding
- Haemosiderin deposition
- Lipodermatosclerosis (champagne bottle)
- Ulceration
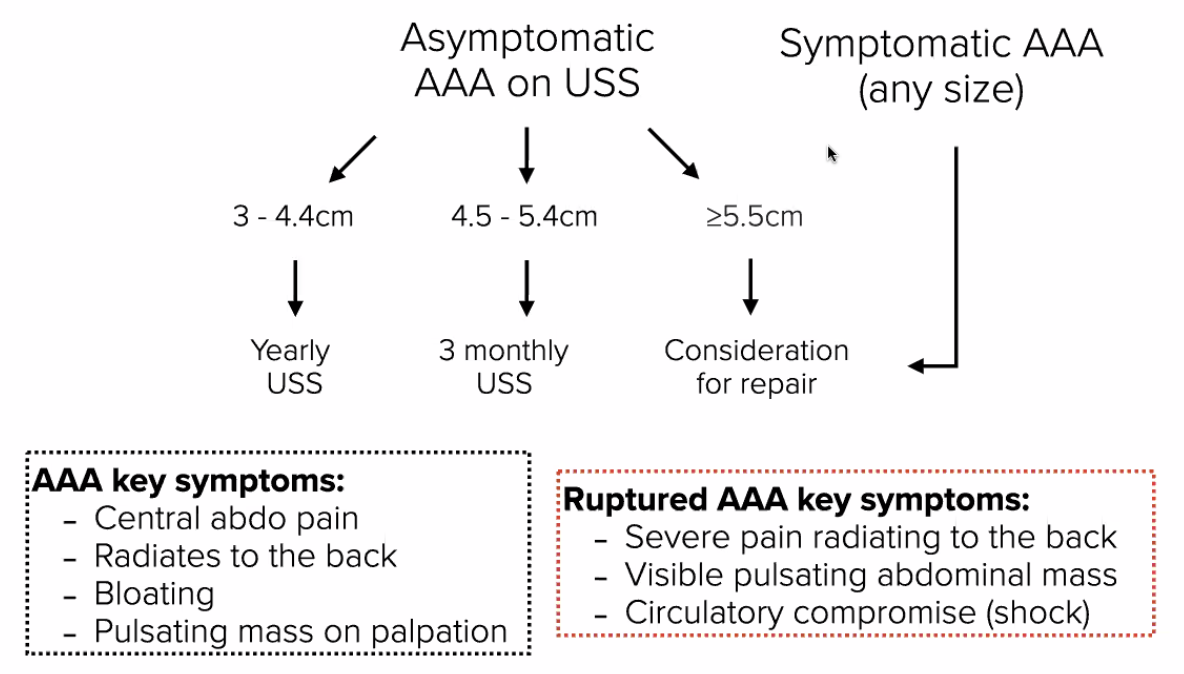
AAA key Sx & ruptured Sx? Ix? Mx?
Sx:
- Central abdo pain
- Radiates to back
- Bloating
- Pulsatile mass on palpation (expansile - moves to sides)
- NOTE: always consider if abdo pain + RFs (male, >65yrs, HTN, smoking etc.)
Ruptured AAA Sx:
- Severe pain radiating to back
- Visible pulsating abdo mass
- Shock (circulatory compromise)
Ix:
- Abdo duplex USS if part of national screening - male age 65yrs
- CT angiography if stable but suspicious of rupture
Mx:
- <5.5cm –> Conservative: monitor w/ USS + RF modification
- <4.5cm –> yearly USS
- 4.5≤x<5.5com –> 3 monthly USS
- Medical: optimise BP control, statin, aspirin
- Sx/>5.5cm/expanding >1cm/yr –> Surgical: endovascular (catheter into aorta to insert stent)/open repair
How to calculate ABPI? ABPI value range?
- BP cuff above ankle with leads upwards – find dorsalis pedis pulse with doppler
- Inflate cuff until signal disappears – let down cuff until signal reappears = ankle pressure
- Repeat procedure in arm using brachial artery signal to record the brachial pressure
- ABPI = ankle pressure/brachial pressure
Range:
- 0.8-1 = normal
- 0.6-0.8 = claudication (may only drop to this with exercise)
- Below 0.6 = critical limb ischaemia
Aortic dissection - def? Sx? Ix? Mx?
Def: tear in tunica intima (inner layer of BV) –> blood collection between tunica intima and tunica media –> false lumen (can occlude blood flows through aorta) –> AR, myocardial ischaemia, stroke
Sx: sudden onset, central tearing chest pain –> radiating to between shoulder blades
- Hx of intermittent claudication
- Haemodynamic instability (high HR, low BP)
- Before left subclavian artery - left arm smaller than right arm
- After left subclavian artery - lower body less developed than upper body
Ix:
- BP in both arms - radio-radial delay
- ECG, CXR (widened mediastinum)
- Gold-standard: CT-aortogram w/ contrast
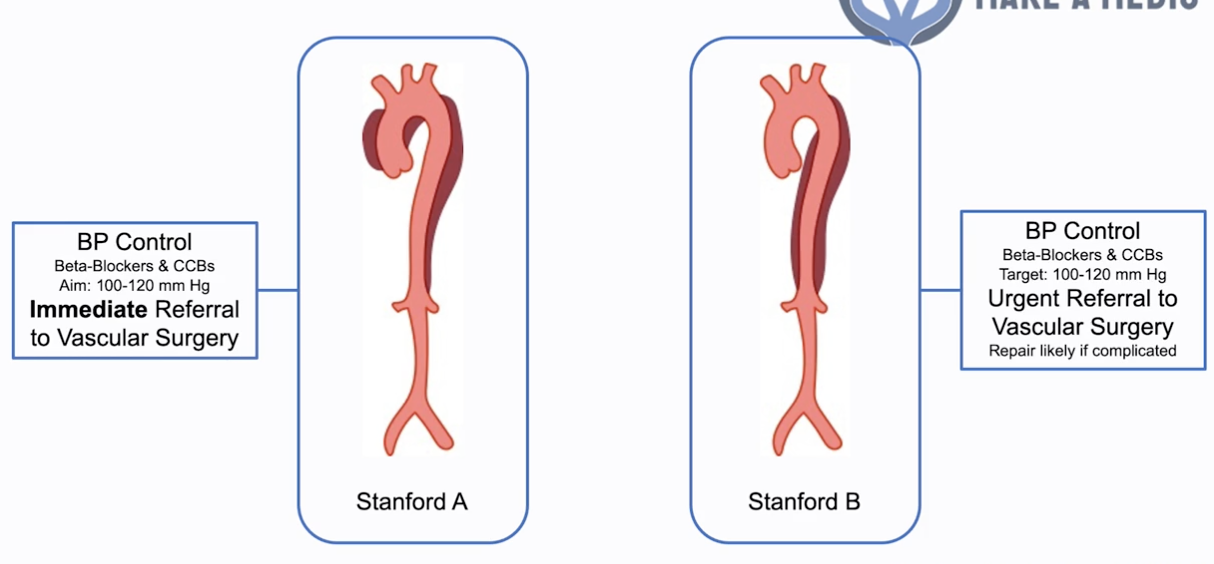
Mx:
- Stanford A (ascending aorta) - more WORRYING (compromise blood to brain, cause aortic regurg):
- BP control - B-blockers & CCB (aim 100-120mmHg)
- Immediate referral for vascular surgery
- Stanford B (descending aorta)
- BP control - B-blockers & CCB (aim 100-120mmHg)
- Urgent referral to vascular surgery (repair likely if complicated)