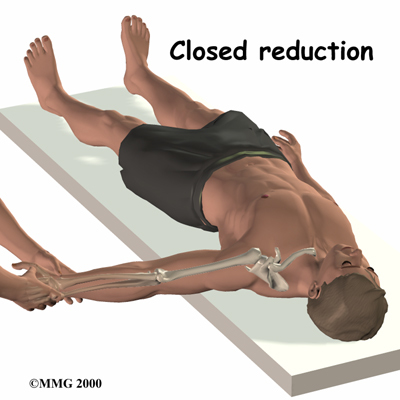
Injury to the upper chest can create a palpable defect in the region of the sternoclavicular joint, with posterior dislocation of the clavicular heads and upper airway obstruction. How do you reduce this injury?
1/ Closed reduction by extending the arm.
2/ Grasping the clavicle with a pointed instrument (e.g. a towel clamp) and manually reducing it.
What major thoracic injuries should be picked up on and addressed during the primary survey?
- Tension pneumothorax
- Open pneumothorax
- Flail Chest
- Pulmonary Contusion
- Massive haemothorax
What type of shock is a tension pneumothorax?
Obstructive shock
How does a tension penumothorax develop?
- A “one way valve” air leak occurs from the lung or through the chest wall.
- Air is forced into the pleural space without any means to escape.
- The mediastium is displaced to the opposite side, decreasing venous return and compressing the opposite lung.
After intubation what is one of the common reasons for loss of breath sounds in the left thorax?
A right mainstem intubation.
(Be aware that this can happened and don’t mistake it for a pneumothorax/haemothorax)
What are some causes of a tension pneumothorax?
1) Mechanical ventilation with positive-pressure ventilation in patients with a visceral pleural injury. (Most common)
2) Blunt/penetrating chest trauma where the lung parenchyma injury fails to seal.
3) Post subclavian/Internal jugular venous catheter insertion.
4) Traumatic defects in the chest wall.
What signs and symptoms are seen with a tension pneumothorax?
- Chest pain
- Air hunger
- Respiratory distress
- Tachycardia
- Hypotension
- Tracheal deviation away from the side of injury
- Unilateral absence of breath sounds over hemithorax.
- Elevated hemithorax w/o respiratory movement.
- Neck vein distension
- Cyanosis (late manifestation)
How does one manage a tension pneumothorax?
1/ Immediate decompression.- a large bore needle is inserted into the second intercostal space in the midclavicular line.
2/ Definition treatment - insertion of a chest tube into the fifth intercostal space (usually at the nipple level) just anterior to the mixaxillary line.
What size needle should you use and what percentage chance will it be effective in chest decompression?
A 5cm needle will reach the pleural space >50% of the time.
An 8cm needle will reach the pleural space >90% of the time.
In what circumstances does an open pneumothorax occur?
It occurs when there is a large defect in the chest wall which allows atmospheric air to rush into the pleural space, thus equalizing atmospheric and intrathoracic pressure.
How is an open pneumothorax managed?
Temporary- A sterile occlusive dressing is placed over the wound with 3 sides taped down to provide a flutter valve.
As the patient breathes in the dressing occludes the wound and thus the lung expands. On breathing out, the open end of the dressing allows air to escape.
Definitive - surgery

Describe how a flail chest occurs and its management.
1/ Trauma causing multiple rib fractures in two or more adjacent ribs in 2 or more places.
2/ Initial management -
- Adequate ventilation
- Administration of humidified oxygen
- Fluid resuscitation. (But fluid resuscitation should be used carefully so as not cause overload)
- IV morphine or intercostal blocks.
3/ Final management - surgery
What is the definition of a massive haemothorax?
A rapid accumulation of more than 1500mL of blood or 1/3 or more of the patient’s blood volume in the chest cavity .
What are the common causes of a massive haemothorax?
1/ A penetrating injury that disrupts the systemic or hilar vessels.
2/ Blunt pulmonary trauma
What are the signs of a massive hemothorax?
Shock associated with the abscence of breath sounds or dullness to percussion on one side of the chest.
How should a massive haemothorax be managed?
- A 36 or 40 French chest tube is inserted in the nipple line just anterior to the midaxillary line.
- Continue to early thoracotomy if 1,500mL of fluid is immediately evacuated.
- If patients continue to bleed or they require persistent transfusions, then they may also require a thoracotomy.
What is the most common cause of cardiac tamponade?
Penetrating injury.
How do you diagnose a cardiac tamponade?
Using Beck’s Triad of 1/ Venous pressure elevation 2/ Decline in arterial pressure 3/ Muffled heart tones.
ECG - PEA is suggestive.
FAST Scan
How accurate is a FAST scan in finding pericardial fluid? (if used by an experienced user)
90-95%
How is a cardiac tamponade managed?
1/ Temporarily - pericardiocentisis
2/ Surgery - Pericardiotomy via thoracotomy.
What are some complications of a chest tube insertion?
- Laceration or puncture of intrathoracic organs or abdominal organs.
- Infection
- Intercostal nerve damage
- Incorrect tube position
- Chest tube kinking or clogging
- Persistent pneumothorax - leak around the skin, leak in the underwater seal.
- Subcutaneous emphysema
- Recurrence of penumothorax upon chest drain removal.
- Lung fails to expand due to plugged bronchus.
- Anaphylactic or allergic reaction to prepartion.
What are some complications of pericardiocentesis?
- Aspiration of ventricular blood instead of pericardial blood.
- Laceration of ventricular epicardium/myocardium
- Laceration of coronary artery or vein.
- New hemopericardium secondary 2-3.
- Ventricular fibrillation (VF)
- Pneumothorax
- Puncture of esophagus with subsequent medistinitis.
- Puncture of peritoneum with peritonitis.
- Puncture of great vessels
What does a “current of injury” mean?
In a pericardiocentesis, in the needle is advanced too far then on the ECG monitor one can see an extreme ST-T wave changes or widened & enlarged QRS complex.
If the myocardium is irritated then premature ventricular contractions can occur.
What maneuvers can be effectively accomplished with a resuscitative thoracotomy?
1/ Evacuation of pericardial blood causing tamponade
2/ Direct control of exsanguinating intrathoracic hemorrhage.
3/ Cross-clamping of the descending aorta to slow blood loss below the diaphragm and increase perfusion to the brain and heart.

