Question to ask before giving IVF
- is my patient, euvolaemic, hypovolaemic (dehydrated) or hypervolaemic (fluid overload)
- Does my patient need IVF
- How much?
- What type do they need?
Types of Fluid
Hypotonic Fluid: (fluid→ cells, cells swell)
Hypertonic Fluid: (Fluid → out of cells, cells shrink)
Isotonic Fluid: Keep everything the same
How do you assess volume status (fluid overload or dehydrated)
Fluid Overload:
- Weight gain
- Swollen ankles
- High BP
Dehydration:
- Weight loss
- Dry mouth
- Low BP
- Dizziness
When DOESN’T the patient need IV fluids
Drinking enough, on enteral feed, already fluid overloaded
What are the IV fluids for?
- Maintenence: to maintain normal fluid balance (in patients not drinking/eating etc)
- Replacement of losses: replace lost body fluids + electrolytes (vomiting, poops etc)
- Rescuscitation: hypotensive, very very sick and need heaps of fluid to get system up.
How much is maintenence fluid?
~2-3L
To counteract loss from pee, poo, sweat and breathing
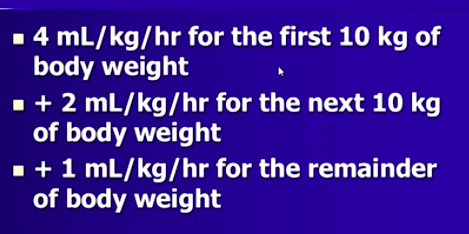
What is the 4:2:1 rule for paediatric IVF
Babies don’t need the same amount of fluid as adults (1L bag over 8hrs = 3L/day)
Replacement Fluid: What might you be replacing? How do you know what to replace
Vomiting, post-surgery drainage, poops!
Replacing loss + continue maintenence fluid!
- Careful assessment of fluid status (weight and JVP helpful)
- Patient record of losses (fluid balance charts)
What do we need to do if a patient is SHOCKED
Rescuscitation: give them a lot of fluid really quickly to bring the BP up
When do you give Isotonic fluid?
Generally give this (safest). Unless your giving maintanence fluid and your overloaded (give hypotonic), or have a high serum Sodium (give hypotonic)
Plasmalide or saline
When do you give hypotonic fluid?
Rarely, when the patient needs maintenence fluid but already overloaded or with a high serum Na+.
Use 5% dextrose: start as isotonic but metabolised bu cells to → free water
When do you give Hypertonic Fluid?
For very low serum Na+
What is Hyponatraemia (low serum sodium)?
due to water excess (not low Na+).
Where is the IV fluids going?
Extracellularly
Na+ loss is from?
- GI loss (vomiting, diarrhoea)
- Hypo-aldosterone (less Na+ reabsorbed)
- Sweat
- Diuretics
What is Pseudohyponatremia??
When lab tests say you have low Na+ but you don’t!!
Very high triglycerides or protein
When do you get water excess?
Syndromes with water overload:
- Cirrhosis
- Heart Failure
- Nephrotic Syndrom
SIADH
Polydipsia
Whats the serum osmolality like in hyponatremia?
Low! (most of osmo from Na+)
Water Excess with euvolaemia
No signs of dehydration, oedema, JVP not elevated.
No evidence of fluid overload, so it’s probably
-SIADH
-Polydipsia
-Overhydration with low Na IVF
Diuretics
How do you know the hyponatraemia is due to Polydipsia?
The patient will have a unusually low urine osmolarity
(usually hyponatraemic patients have high serum osmolarity)
SIADH
Usually in response to low BP or dehydration (sensed via baroreceptors and osmoreceptors)
ADH release despite neither of these occuring
Causes: tumors, CNS, drugs, lung disease
Diuretics
Commonest tohave low Na+ with Thiazides
- Increase ADH
- cause decreased Na+
Like SIADH but due to a drug
Correction of Hyponatraemia
- Saline* for a dehydrated patient with sodium loss
- Fluid restriction* for patients with water excess
-
Renal Histology24
-
Renal Phys: Body Fluid Comp PART 112
-
Renal Phys: Body Fluid comp PART 218
-
Glom and Tubular Function 131
-
Glom and Tubular Function 225
-
Kidneys, Ureter, Bladder and Posterior Abdominal Wall38
-
Clinical Renal Failure and tests32
-
Haematuria Proteinuria31
-
Inguinal Canal and Spermatic Cord21
-
Radiology Imaging of the Renal Tract14
-
Imaging the Female and Male Pelvis0
-
Child Birth27
-
Integration of Salt and Water Balance14
-
Pelvic Contents27
-
Perineum23
-
Acid-base Balance #119
-
Acid-Base Balance #217
-
Integration of Salt and water Balance 216
-
Clinical Problems: Kidney Failure20
-
Clinical Problems: Electrolytes23
-
Clinical Gynaecology22
-
Male and female Genitalia27
-
Testes and Penis pathology23
-
Carcinoma of the prostate18
-
Sexual Function and Dysfunction30
-
Pathology of the ovary and uterus0
-
Cervical screening and pathology31
-
Sexually Transmitted Diseases27
