definition of COPD
Chronic, progressive lung disorder characterized by airflow obstruction (FEV1<80% predicted; FEV1/FVC<0.7), with little or no reversibility; with the following:
chronic bronchitis: Chronic cough and sputum production on most days for at least 3months per year over 2 consecutive years, symptoms improve if stop smoking, no excess mortality if lung function is normal ; and/or
Emphysema: Pathological diagnosis of permanent destructive enlargement of air spaces distal to the terminal bronchioles, destruction of alveolar walls - defined histologically but often seen on CT
aeitiology of COPD
bronchial and alveolar damage from env toxins eg cigarette smoke
rare cause is a1-antitrypsin deficiency (<1%) - should be considered in young/people never smoked
overlaps and may co-present with asthma
chronic bronchitis: narrowing of airways from bronchiole inflammation (bronchiolitis) and bronchi with mucosal oedema, mucous hypersecretion and squamous metaplasia
emphysema: destruction and enlargement of the alveoli = loss of elastic traction that keeps small airways open in expiration, progressively larger spaces develop called bullae (diameter >1cm)
epidemiology of COPD
very common - prevalence up to 8%
middle age/later
more common in males, likely to change with increase in female smokers
10–20% of the over-40s; 2.5≈106 deaths/yr worldwide
presenting symptoms of COPD
chronic cough with sputum production
breathlessness
wheeze
reduced exercise tolerance
usually pts have COPD or asthma - not both. COPD more likely in:
- >35yrs at presentation
- sputum production
- smoking or pollution related
- chronic dyspnoea
- minimal diurnal or day-day FEV1 variation
signs of COPD
inspection
- resp distress
- tachypnoea
- use of accessory muscles
- barrel-shaped overinflated chest
- reduced cricosternal distance (<3cm)
- cyanosis
- hyperinflation
- reduced expansion
percussion
- hyper-resonant chest
- loss of liver and cardiac dullness
auscultation
- quiet breath sounds eg over bullae
- prolonged expiration
- wheeze
- rhonchi and crepitations sometimes present
signs of CO2 retention
- bounding pulse
- warm peripheries
- flapping tremor of hands (asterixis)
- in late stages
- signs of RHF eg R ventricular heave, raised JVP, ankle oedema
cor pulmonale
pink puffers COPD
increased alveolar ventilation, a near normal PaO2 and a normal or low CO2
breathless but not cyanosed
may progress to type 1 resp failure
blue bloaters COPD
low alveolar ventilation
low O2 and high CO2
cyanosed but not breathless
may go on to develop cor pulmonale
respiratory centres are relatively insensitive to CO2 and they rely on hypoxic drive to maintain respiratory eff ort - supplementary oxygen should be given with care
investigations for COPD
spirometry and pulmonary function tests
- obstructive picture = low PEFR, low FEV:FVC ratio (mild, 60–80%; moderate, 40–60%; severe,<40%), increased lung volumes and CO gas transfer coefficient reduced when significant alveolar destruction
- air trapping
- FEV1<80% of predicted, FEV1 : FVC ratio <70%, high TLC, high RV, low DLCO in emphysema
CXR
- may appear normal or show hyperinflation (>6 ribs visible anteriorly, flat hemi-diaphragms)
- reduced peripheral lung markings
- elongated cardiac silhouette
- large central pulmonary arteries
- bullae
blood
- FBC (high HB and PVC as a result of secondary polycythaemia)
ABG
- may show hypoxia - low ox
- normal or high co2
ECG and echo
- for cor pulmonale
- RA and RV hypertrophy
sputum and blood cultures
- in acute exacerbations for treatment
Considera1-antitrypsin levels in young patients or minimal smoking history.
CT
- bronchial wall thickening
- scarring
- air space enlargement
clinical signs/symptoms of infective exacerbation of COPD
smoker
high temp
high RR
clubbing
wheeze and crepitation
productive cough
haematopsis
management plan for COPD
stop smoking
exercise
diet advice +- supplements
mucolytics may help chronic productive cough
bronchodilators - short acting B2-agonists (salbutamol) and anticholinergics (ipratropium) delivered by inhalers/nebulizers. Long acting bronchodilators should be used if >2 exacerbations per yr
steroids
- Inhaled beclometasone should be considered for all with FEV1<50% predicted or those with>2 exacerbations per year.
- regular oral steroids should be avoided but may be necessary for maintenance
pul rehab
oxygen therapy - only for those who stop smoking
- long term home ox therapy shown to improve mortality
- indications:
- PaO2<7.3 kPa on air during a period of clinical stability.
- PaO27.3–8.0 kPa and signs of secondary polycythaemia, nocturnal hypoxaemia, peripheral oedema or pulmonary hypertension.
- ox concentrations are more economical if used for >8hr/day
prevention of infective exacerbations
- pneumococcal and influenza vaccination
diuretics for oedema
treatment of acute infectious exacerbations COPD
24% Ox via non-variable flow venturi mask
increase slowly if no hypercapnia and still hypoxic - measured by ABG
corticosteroids oral or inhaled
start empirical AB therapy if infection
resp physio to clear sputum
consider non-invasive ventilation in severe cases
bronchodilater therapy - symptom relief (wheeze from bronchial narrowing)
complications of COPD
acute resp failure
acute exacerbations +- infections - particularly streptococcus pneumoniae, haemophilius influenzae
pul hypertension and RHF
pneumothorax (from bullae rupture)
secondary polycythaemia
cor pulmonale - oedema, raised JVP
lung carcinoma
prognosis of COPD
75% if>60 years and FEV140–49% predicted.
severity assessment has implications for therapy and prognosis
- The BODE index (Body mass index, airflow Obstruction, Dyspnoea and Exercise capacity) helps predict outcome and number and severity of exacerbations.
- The Global Initiative for COPD (GOLD) categorizes severity of COPD into four stages (mild, moderate, severe, and very severe) based on post-bronchodilator FEV1% predicted, but it is not useful for predicting total mortality for 3 years of follow-up and onwards.
most likely dx and why
- demonstrates hyperinflated lungs with flattening of the hemi-diaphragms (>7 anterior, >9 posterior ribs seen in the lung fields
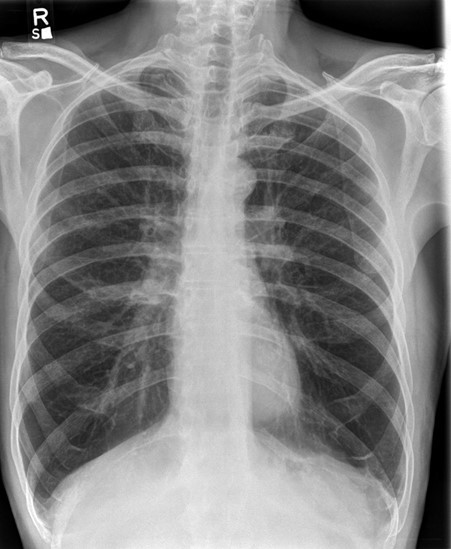
COPD
-
Bronchiectasis10
-
COPD14
-
pneumonia42
-
asthma42
-
ards18
-
ABG3
-
asbestos related lung disease19
-
aspergillus lung disease23
-
extrinsic allergic alveolitis22
-
idiopathic pulmonary fibrosis16
-
lung cancer29
-
obstructive sleep apnoea10
-
PE17
-
sarcoidosis24
-
pneumoconiosis8
-
tb25
-
pneumothorax18
-
bronchitis8
-
cystic fibrosis14
