What is
osteopathic cranial manipulative medicine?
A system of diagnosis and treatment by an osteopathic practitioner using the primary respiratory mechanism and balanced membranous tension.
What is primary respiratory mechanism
Primary Respiratory Mechanism = motion that is perceptable throughout the body
- Primary = Fundamental life process
- Respiratory = Motions of head are the breath of life
- Mechanism = Movement of tissue and fluid for a purpose
5 components of PRM
- Inherent mobility of the brain and SC
- Fluctuation of the CSF
- Mobility of the intracranial and intraspinal membranes (fascial mobility and continuity significaly impact PRM)
- Articulatory mobility of the cranial bones
- Involuntary mobility of the sacrum between the ilia
The inherent mobility of the brain and SC is due to what?
Inherent mobility = force acts on brain to cause it to move.
The force = Glial cells, contractile elements in the brain: support cranial motion structurally and physiologically by regulating BF.
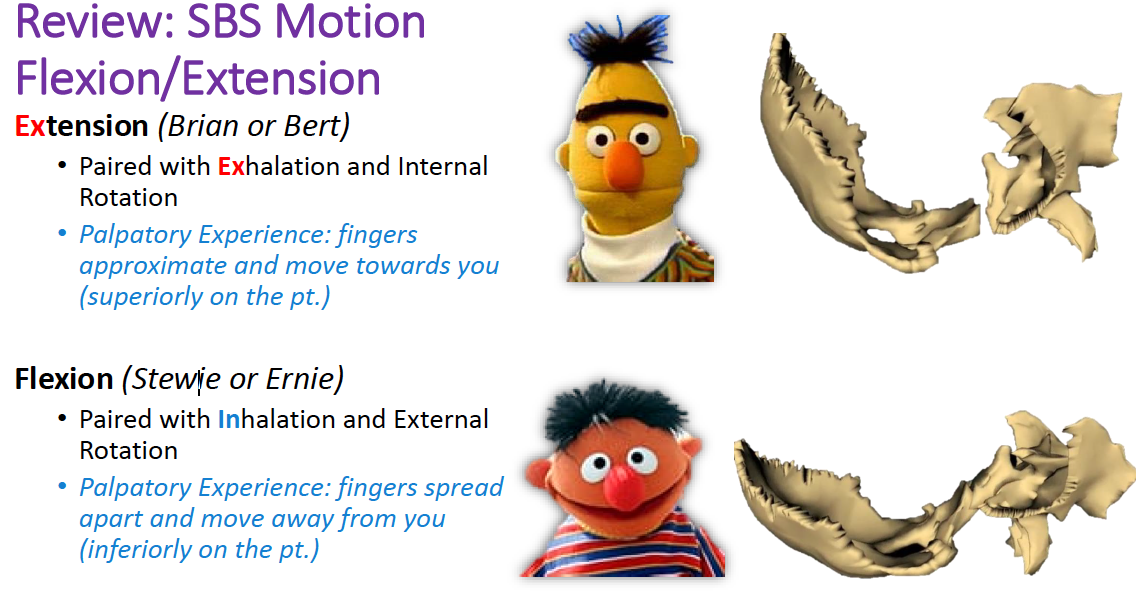
- During the inhalation (flexion) the brain (and bony cranium) => shorter and wider.
- During the exhalation phase (extension) the brain (and bony cranium) gets taller and narrower.
Glial cells job in supporting cranial motion structually and physiologically by regulating blood flow is seen by what evidence?
Traube-Hering Wave: changes in velocity of blood flow
What is the cranial rhythmic impulse (CRI)?
rhymic impulses the skull exhibits
Average = 10 - 14/ minute (ranges 6-14)
how do you find the CRI?
- Palpation: contact the head very light => perform a layer palpation (head => skin => subcutaneous tissue => bone)
- Must be palpated, cannot see.
How does the CRI relate to respiratory and/or circulatory physiologic mechanisms?
Separate, but influenced by them.
If a patient holds their breath => CRI is still palpable
Motion characteristics of CRI
R-RADS
R-RADS
- Rate = 10 -14 bpm
- Rhythm = regular, subtle like the tide of the ocean.
- Amplitude: ⬇︎with SD
- Direction = in healthy ppl = longitudinal and symmetric, but SD => asymmetic.
- Strength = SD and vitality of pt impacts strength
What is the fascia continuity between the head and sacrum, allowing the mobility of intracranial and intraspinal membranes?
Reciprocal tension membrane (RTM) = dural membranes (tentorium, falx cerebelli and cerebri =sutherland fulcrum) that act as a unit and are held under constant tension bc attached to the bones of the vault and base and SC, serving as the “core-link” between the cranium and S2 of the sacrum.
Allows but limits motion: allows for vault to change shape, but holds constant volume
Dura attaches to the occiput and ANTERIOR part of S2 of sacrum
What creates the reciprical tension membrane (RTM) and what does it do?
Tentorium + falx cerebri + cerebellum.
Function as a unit and attaches the the bones of the vault and base, holding them under constant tension => lets for change of shape of the vault, while maintaing a contant volume. Allows, but limits motion
Main poles of attachment for RTM
- Anterior/superior pole
- Anterior/inferior pole
- Lateral pole
- Posterior pole
- Anterior/Superior pole – crista galli
- Anterior/inferior pole – clinoid processes of sphenoid
- Lateral pole – mastoid angles of parietals and petrous ridges of temporal bones
- Posterior pole – internal occipital protuberance and transverse ridges
What is a Sutherland fulcrum?
- A point of function/stillness (straight sinus), where motion occurs around.
How does the RTM affect motion?
allows, but limits motion
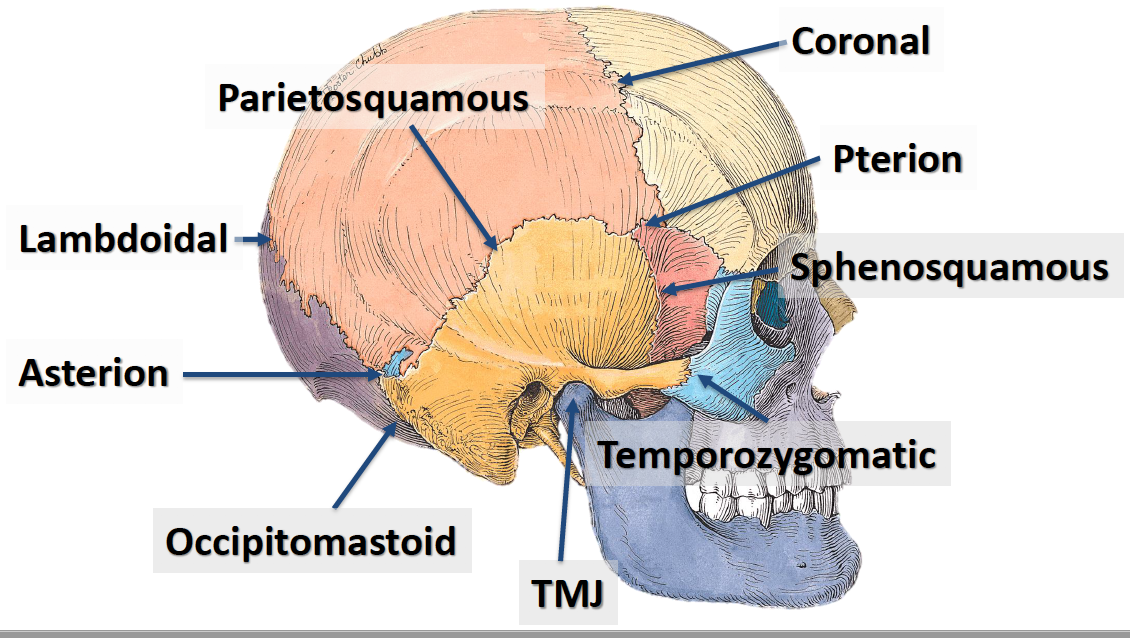
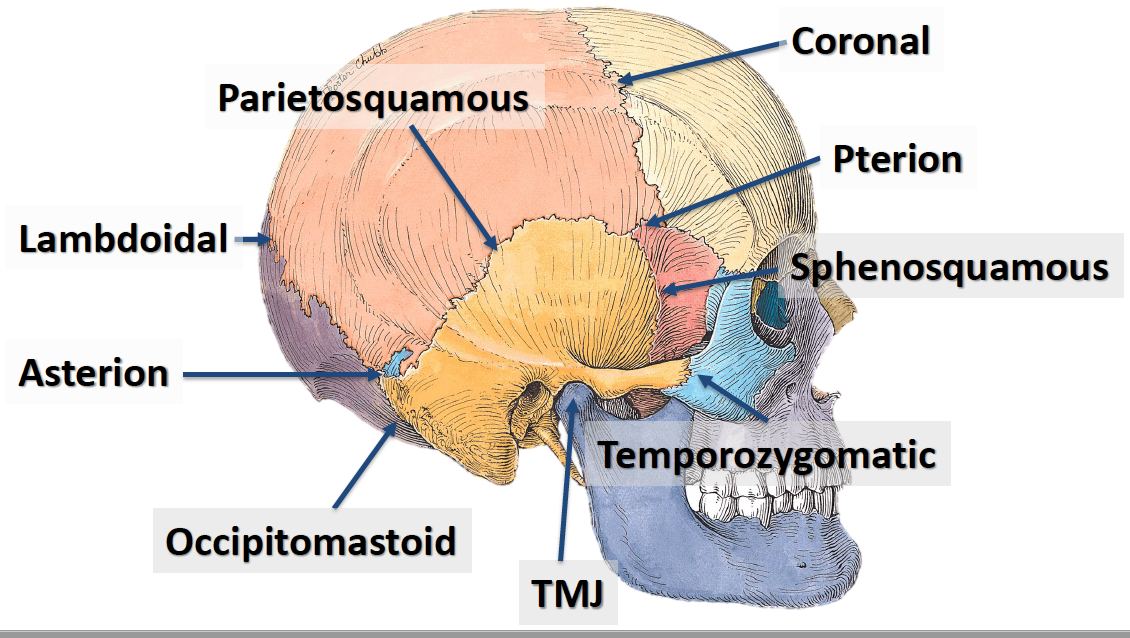
Coronal suture
– from R => L, separates the frontal bone from the parietal bones
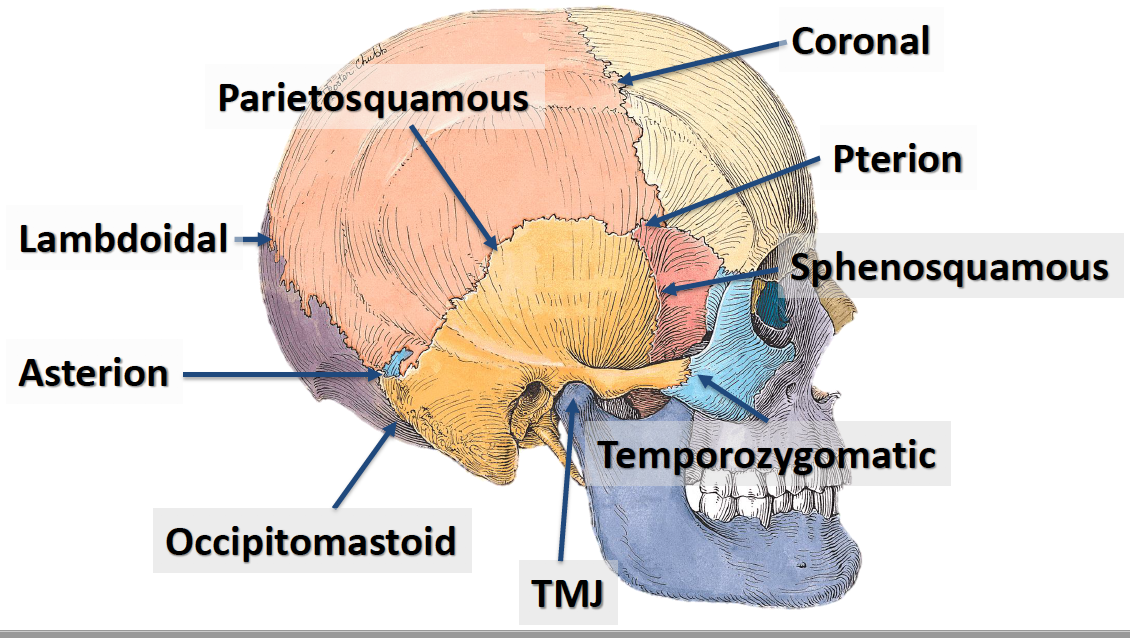
Lambdoidal suture
– from R=> to L, separates the parietal bones from the occipital bone
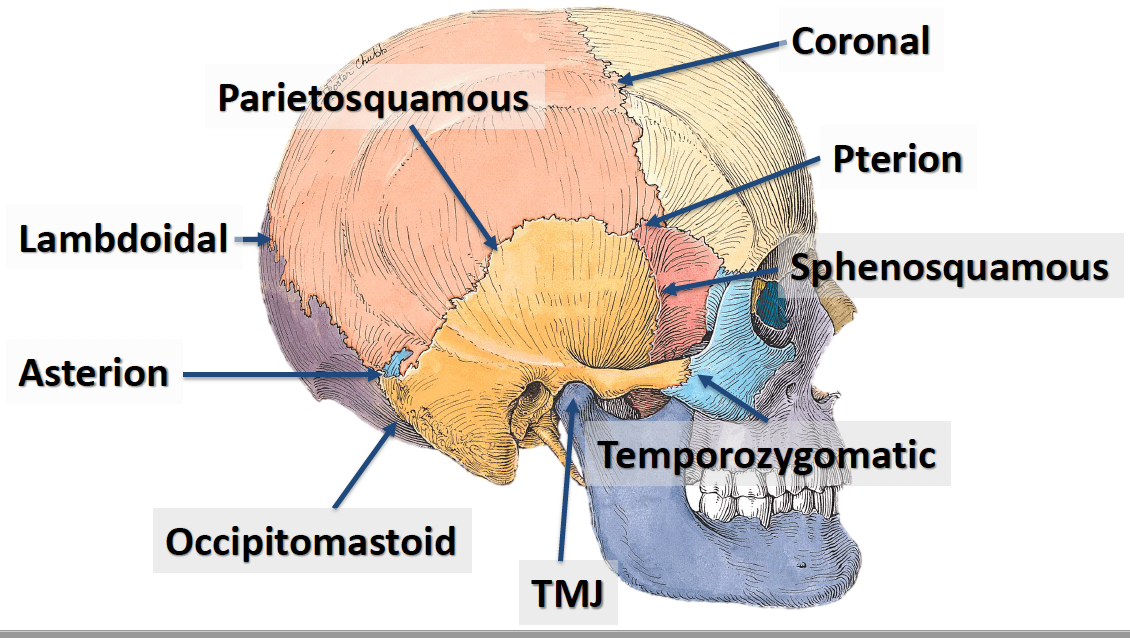
Asterion
where parietal, occipital and temporal bones meet (A is found in the posterior)
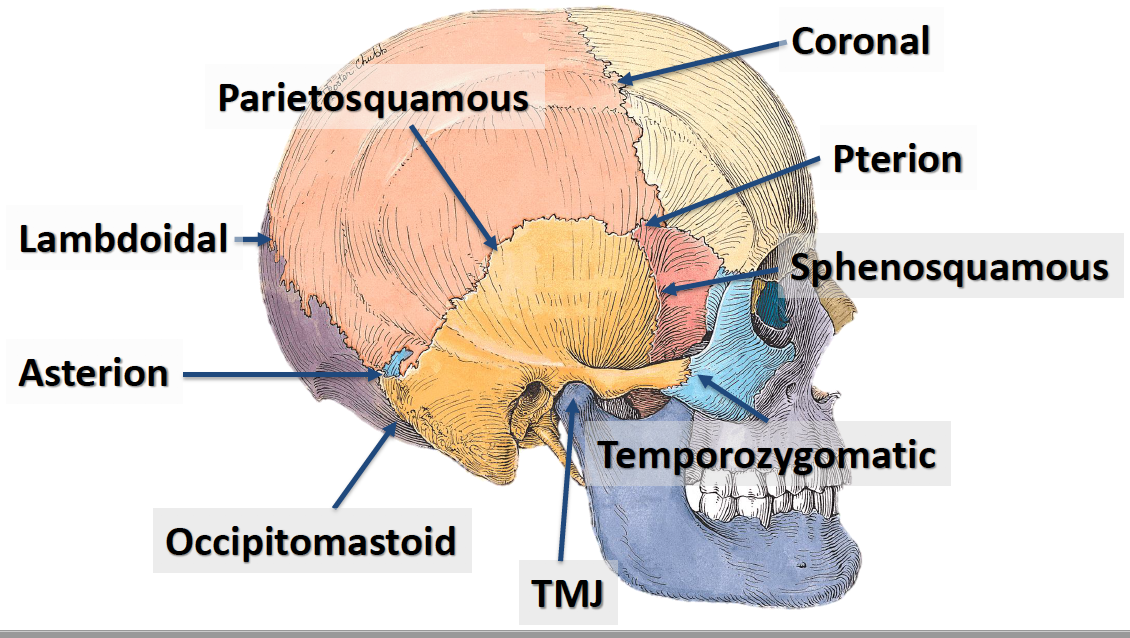
Occipitomastoid suture
– separates the occipital bone from the temporal bone
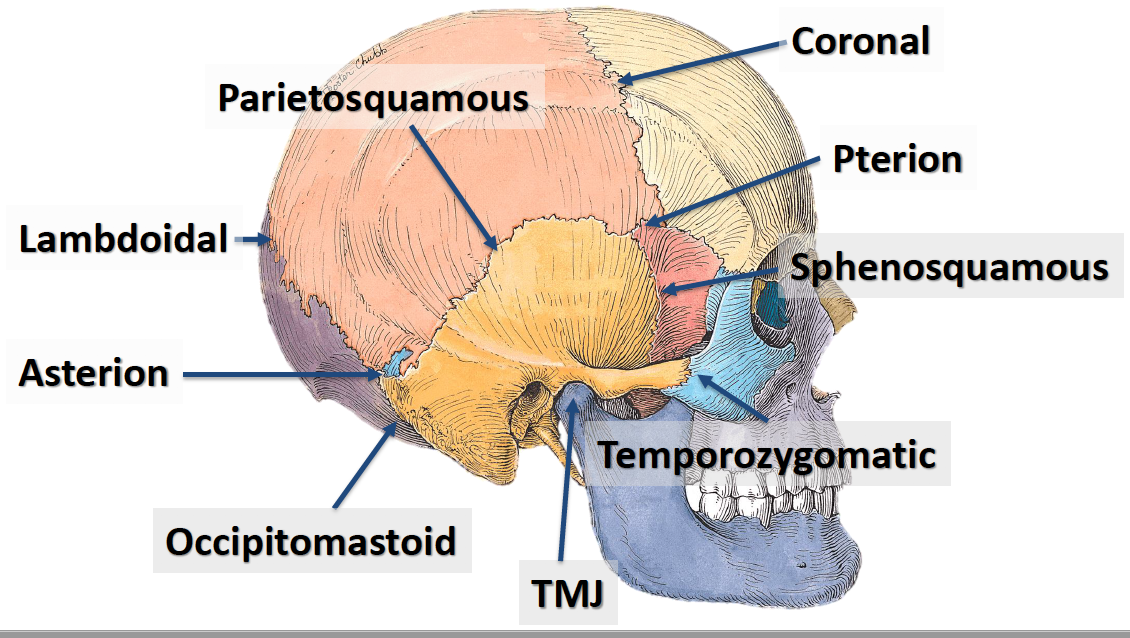
Parietosquamous suture
from anterior to posterior, separates the parietal bones from the temporal bone and sphenoid bone
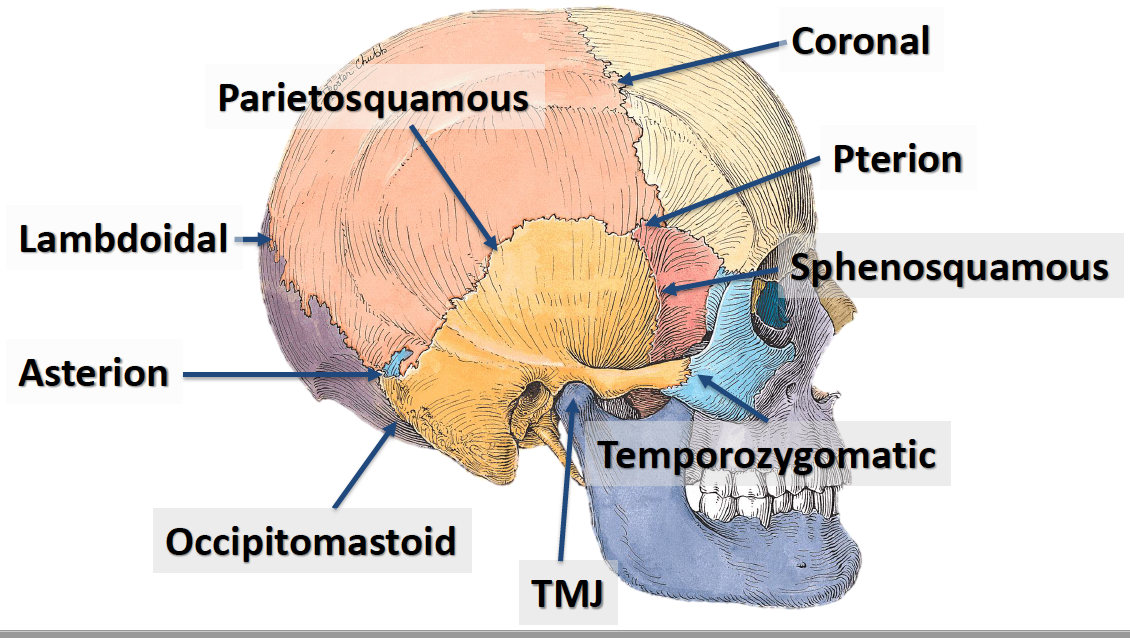
Sphenosquamous suture
from inferior to superior, separates the sphenoid bone from the temporal bone
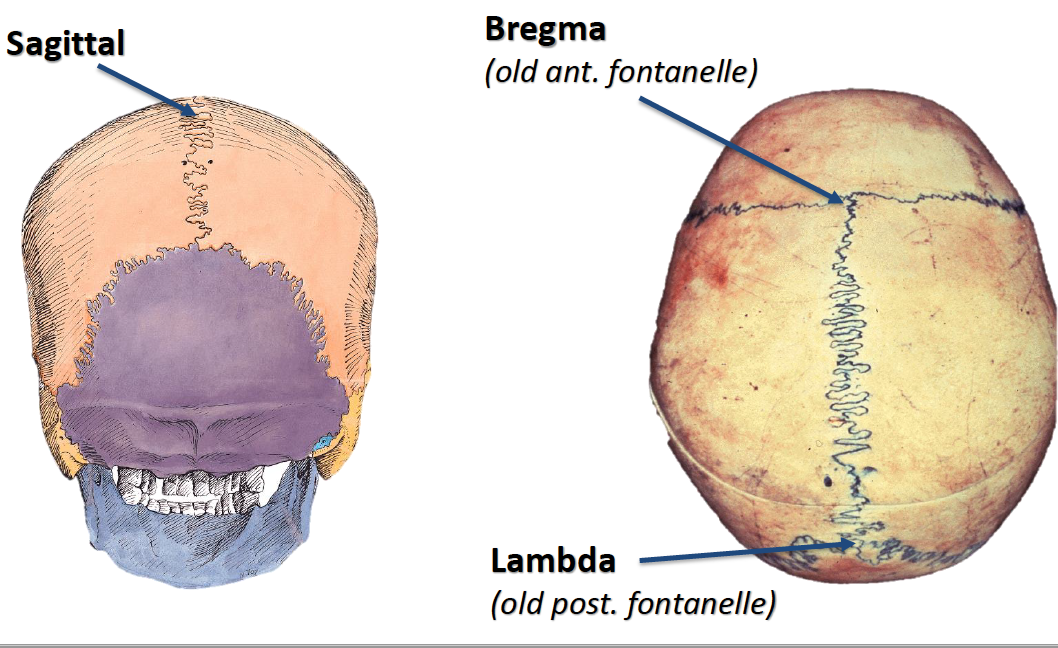
Sagittal suture
– anterior to posterior, separating the parietal bones
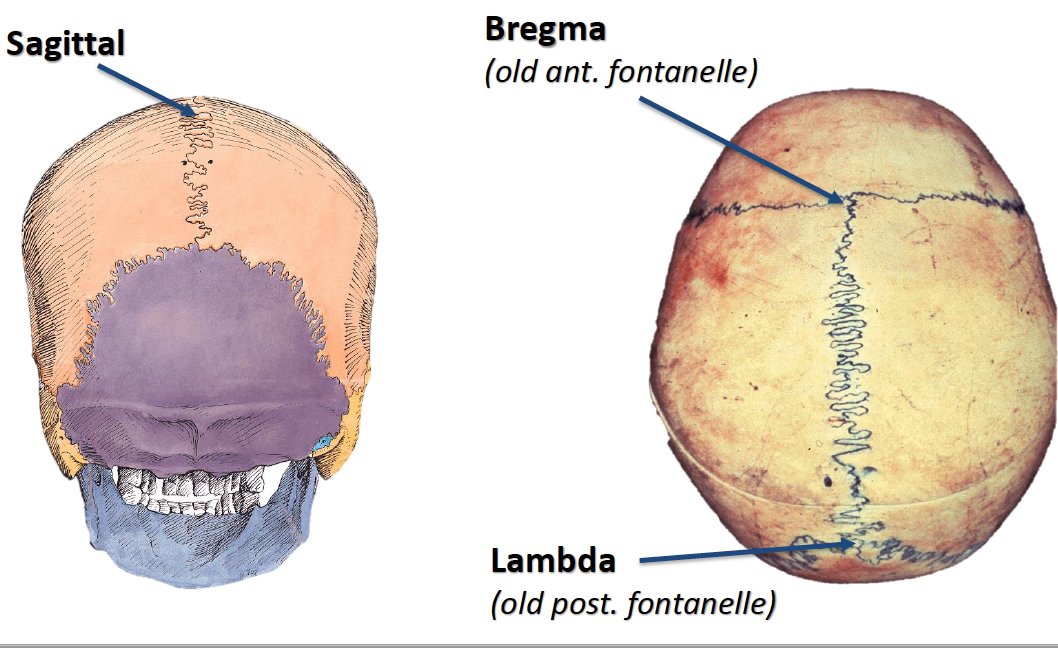
Bregma
where the coronal and sagittal sutures meet, anterior of skull
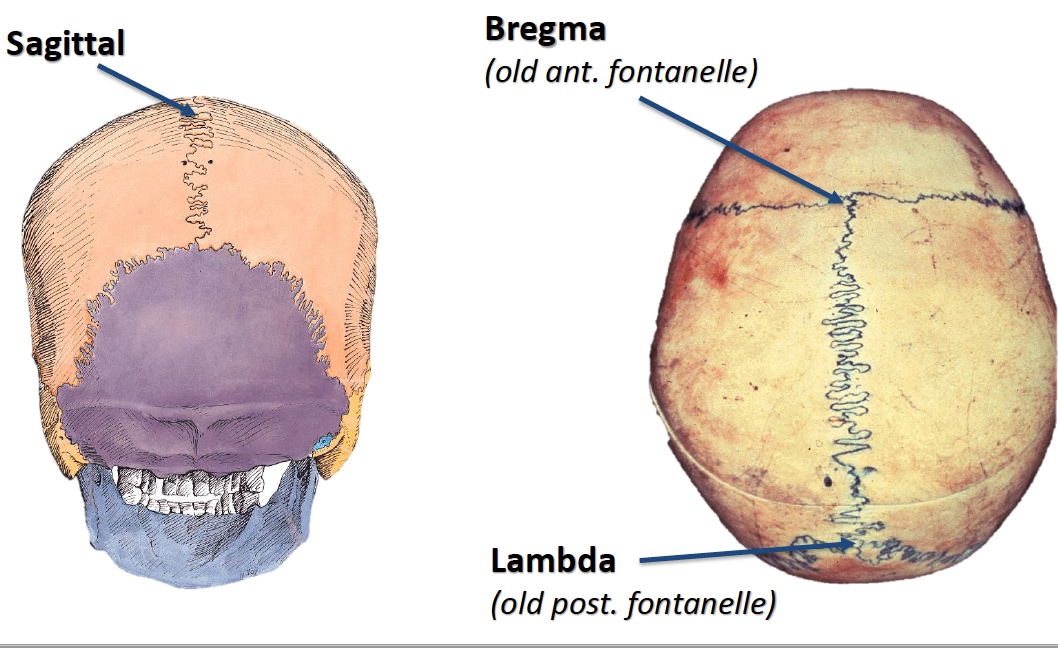
Lambda
where the sagittal and lambdoidal sutures meet, posterior of skull
Pterion
–where frontal, parietal, sphenoid and temporal bones meet (P is found in the anterior)