What is delerium ?
It is a distrubance in attention, where there is a change in congnition e.g. memory deficit, disorientation, language disturbance, perceptional disturbance (ability to see, hear or become aware of something through the senses)
What are the hallmarks for the way the onset of delirium develops ?
Develops over a short period (usually hrs to days) & tends to fluctuates during the day
What is delirium usually caused by ?
By direct physiologic consequence of a general medical condition, an intoxicating substance (more in young people e.g. alcohol), medication use, or more than one cause.
Why is it important to know about delirium ?
15-60% of older people experience delirium prior to or during hospital admission but the diagnosis is missed in up to 70 % of cases
Patients who experience delirium:
- Need to stay longer in hospital or in critical care
- Have an increased incidence of dementia
- Have more hospital-acquired complications, such as falls and pressure sores
- Are more likely to need to be admitted to long-term care if they are in hospital
- Are more likely to die.
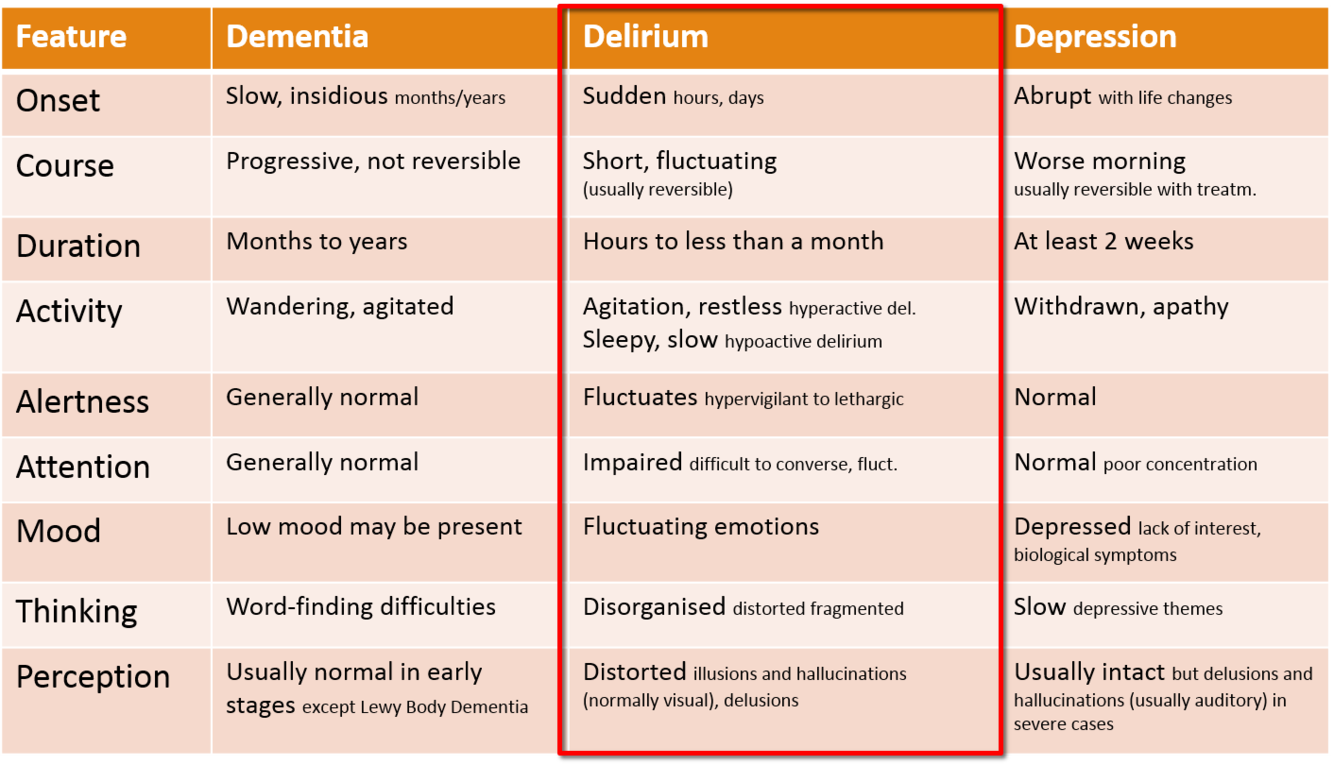
What are the features of delirium ?
- Onest - sudden hrs to days
- Course - short, fluctuating and is usually reversible
- Duration - hrs to usually less than a month but rarley > than a month
- Activity - agitation and restless in hyperactive delirium, sleepy and slow in hypoactive delirium
- Alterness - impaired, difficult to converse with, their alterness also fluctuates
- Mood - fluctating
- Thinking - disorganised, disordered, fragmented
- Perception - distorted, illusions and hallucinations (usually visual), delusions
Describe the pathophysiology of delirium ?
It is not well understood but their is variable derangement of multiple neurotransmitters esp ACh
What are some of the predisposing factors to developing delirium?
- Advanced age
- Pre-existing dementia
- Co-morbidity
- Post-operative period
- Terminal illness
- Sensory impairment (if you cant see or hear very well you are at more risk)
- Polypharmacy
- Depression
- Alcohol dependency (another drug affecting your neuronal function)
- Malnutrition
What are some of the precipitating factors for delirium?
- Infection e.g. UTI, pneumonia
- Change in environment
- Surgery
- Constipation
- Pain
- Dehydration
- Hip fractures
- Low sodium
- Hypoxia
- Medications - esp anti-cholingeric medications
What are the hallmarks of delirium?
- Acute and fluctuating
- Inattention
- Altered level of consciousness
- Disorganised thinking
What are the 2 main subtypes of delirium and describe there main differences for distinguishing them ?
- Hyperactive: Agitated, aggressive, wandering
- Hypoactive: Withdrawn, apathetic (no interest or concern), sleepy, coma
What subtype of delirium carries the greater mortality risk ?
Hypoactive - prob because its harder to diagnose
What are the investigations done to diagnose delirium?
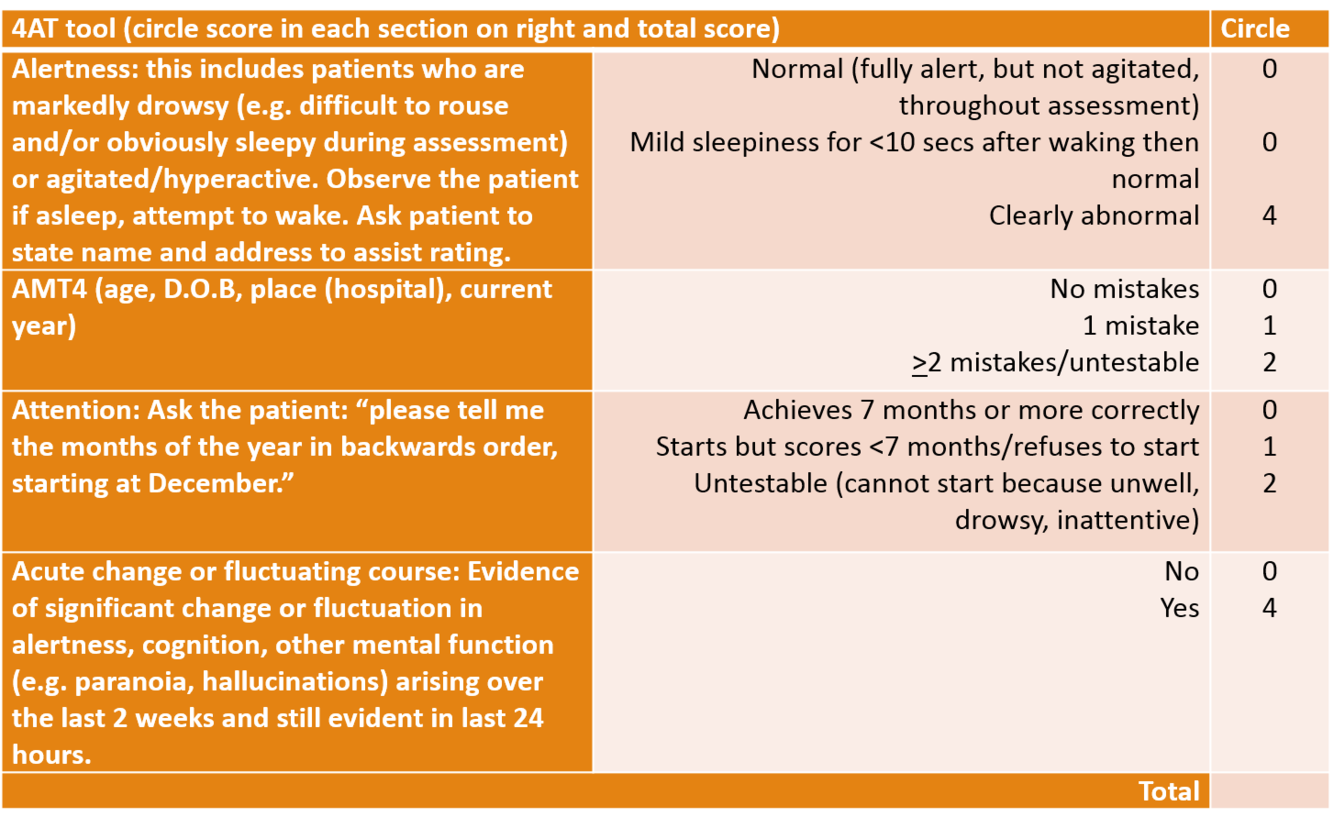
1st line = 4AT this is a rapid test for delirium which only takes 1-2mins and does not require special training (this is a screening test)
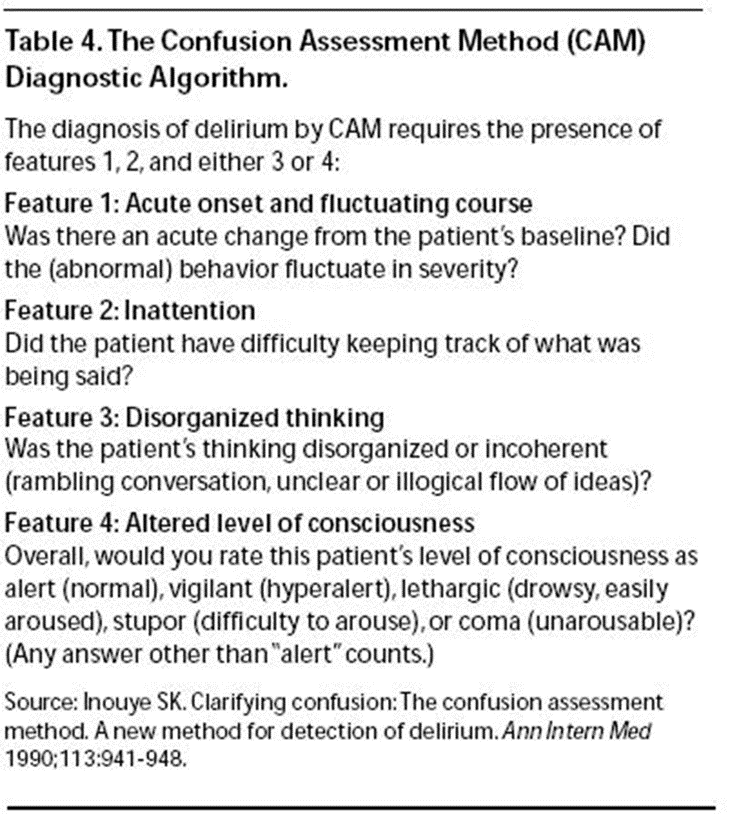
2nd line = short confusion assessment methos (CAM) to confirm delirium diagnosis this has to be carried out by a healthcare professional trained in the diagnosis of delirium
So do 4AT then confirm with CAM
What is the 4AT test also used to help assess?
Cognitive impairment
Describe what to do when carrying out the 4AT test
- Check alterness - this is helped when asking name and DOB
- Ask age, name, DOB, their current location, and the current year
- Check attention - ask patient to say months of the year backwards
- Assess if evidence of any acute changes - is there evidence of sig. change or fluctuation in alterness, cognition, other mental function e.g. paranoia, hallucinations
What are the features assessed in the CAM assessment method and what is required for diagnosis of delirium?
Required presence of features 1&2 + 3 or 4:
- Acute onset & fluctating course - change from patients baseline
- Inattention - patient has difficulty keeping track of whats being said
- Disorganised thinking - rambling, unclear or illogical flow of ideas
- Altered level of conciousness - hypo or hyperactive
What is the initial management of delirium ?
- Identify and manage possible underlying cause/combination of causes
- Check hydration and ensure hydrated
- Stop potential incrimination drugs (anti-cholinergics)
- Optimise BP and perfusion
- Look for intrinsic renal disease
- Tx any infections and correct electrolyte imbalances
- Ensure effective communication and reorientation - provide reassurance, considering involving family, friends and carers to help with this and provide a suitable environment (essentially make environment as familiar as possible)
If a patient is distressed/at risk to themselves or others with delirium what is the 1st and 2nd line management?
- 1st line = verbal and non-verbal techniques to de-escalte the situation
- 2nd line if 1st line ineffective and only if the patient is a danger to themselves or others = give haloperidol
If a patient has parkinsons/lewy body dementia, long QT syndrome, experiences seizures what should be used instead of haloperidol to treat delirium?
Lorazepam (or Quietiapine for parkisons/lewy body dementia - apparently you would use lorazepam 1st day then possibly switch to this in these cirumstances due to lorazepams quicker action first off)
If someone is experiencing alcohol/benzos withdrawl what should be given to prevent progression to delirium tremens ?
Describe what is used in lanarkshire and when you would use one over the other.
- 1st line = chlordiazepoxide
- 2nd line = lorazepam or diazepam
- Also would give IV pabrinex or PO thiamine depending on how they score on GMAWS
Note in lanarkshire they use the GMAWS protocol which uses benzos.
- Longer-acting benzodiazepines e.g. diazepam and chlordiazepoxide may be more effective in preventing delirium tremens and seizures, but there is a risk of accumulation in patients with liver disease or the elderly.
- Consideration should be given to using benzodiazepines with shorter half-lives e.g. lorazepam in liver disease, respiratory failure, elderly and those prescribed other CNS depressants.
What is a complication to be aware of when someone is given IV pabrinex ?
Anaphylaxis
If someone with a history of alcohol/benzo withdrawl develops either delirium tremens or delirium what should be used to treat this instead of haloperidol?
Lorazepam
Why should you follow up patients who have experienced delirium?
- Delirium is a risk factor for developing dementia
- At risk of further episodes of delirium
What are the environmental and general measures for someone experiencing delirium?
- Regularly reassure and re-orientate (use clocks & calendars)
- Ensure buzzer close to patient and respond promptly to calls
- Listen to the patient’s expression of needs
- Reduce noise (e.g. monitors and alarms) and background noise
- If language or hearing problems, consider an interpreter
What are some of the common drugs which can cause delirium and how ?
Opiods e.g. co-codamol can cause constipation resulting in delirium
Bendroflumethazide can cause low Na ==> delirium
Tolderine is an anticholingeric which can cause derangement of neurotransmitters ==> delirium



-
Aging and society a global perspective11
-
Comprehensive geriatric assessment & acute illness10
-
Immobility and rehabilitation27
-
Delirium29
-
Ageing and end of life care14
-
Older people and public health17
-
Aging process16
-
Falls29
-
Appropriate prescribing for older people8
-
Clinical pharmacology of older age20
-
Clinical pharmacology of older age 212
-
Clinical pharmacology 312
-
Stroke - ischaemic30
-
Formative assessment points10
-
Stroke - ischaemic 224
-
Stroke - ischaemic 313
-
Feeding workshop11
-
Haemorrhagic stroke/intracranial haemorrhage25
