Incontinentia Pigmenta
- This is typically lethal in males antenatally.
- X-linked In most patients, cutaneous manifestations are present at birth or occur within the first 2 weeks of life. The cutaneous manifestations usually appear in a characteristic, chronologic sequence.
- Other systemic manifestations, including ocular defects, CNS abnormalities, and dental abnormalities, may not be recognised until infancy or early childhood.
- Diagnostic criteria for incontinentia pigmenti have been proposed. In the absence of a family history, the presence of at least 1 major criterion is necessary. The presence of minor criteria supports the diagnosis of incontinentia pigmenti.
Major criteria are: typical neonatal vesicular rash with eosinophilia -typical blaschkoid hyperpigmentation on the trunk, fading in adolescence -linear, atrophic hairless lesions.
Minor criteria are:
- -dental anomalies,
- -alopecia,
- -wooly hair,
- -abnormal nails
With a definitive family history, the presence of any major criterion strongly supports the diagnosis of incontinentia pigmenti.
Ichthyosis
– the ichthyosiform dermatoses are a diverse group of hereditary skin disorders characterised by the accumulation of “fish-like” scales resulting from abnormal epidermal cell kinetics or differentiation.
- The severity of the individual disorders ranges from asymptomatic to life-threatening.
- Icthyosis vulgaris – mildest form. Presents during childhood, not apparent in the newborn.
- X-linked icthyosis – affects males, onset at 2-6 weeks of age, worsens with age. Large brown adherent scales.
- Lamellar icthyosis – affected patients present as a “collodian baby” at birth.
- CIE (congenital icthyosiform erythroderma) – also presents as a “collodian baby.”
- Epidermolytic ichthyosis – also known as bullous ichthyosis or bullous CIE. Presents with widespread blistering and erythema.
- Harlequin ichthyosis – the most severe form, often lethal perinatally.
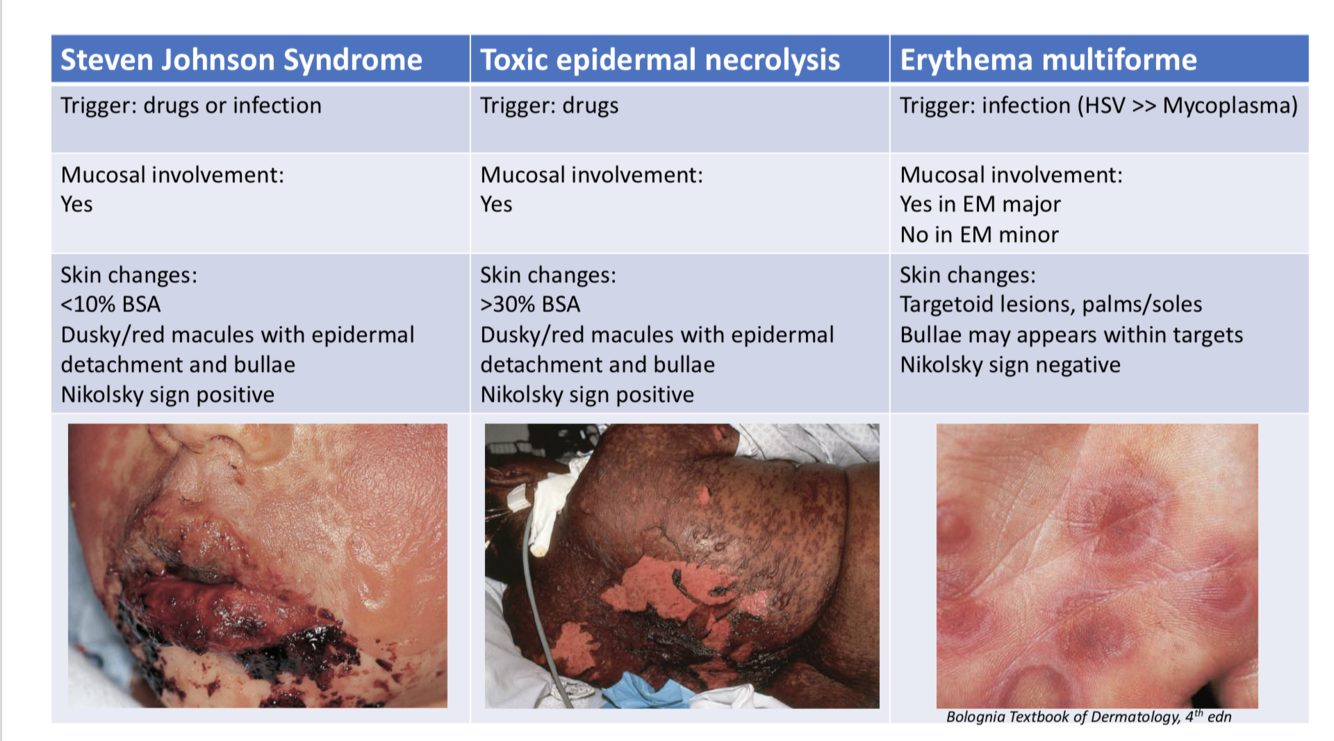
SJS/TEN
Severe adverse cutaneous drug reaction characterised by mucocutaneous tenderness, erythema & extensive exfoliation
- SJS <10% BSA detachment
- SJS-TEN overlap: 10-30% BSA detachment
- TEN >30% BSA detachment
Most common triggers:
- NSAIDs
- Antibiotics: sulfonamides, aminopenicillins, cephalosporins
- Anticonvulsants: carbamazepine, phenytoin, lamotrigine
- Checkpoint inhibitors: ipilimumab, nivolumab
- Allopurinol
Onset symptoms 7-21 days after initiation of drug
Aetiology: • In predisposed individuals, immune response to a drug leads to secretion of cytotoxic granulysin plus interaction of Fas-FasL apoptosis of keratinocytes leads to separation of skin at dermal-epidermal junction
Clinical features:
- Prodrome:URTIsx, fever,painful skin, pain on swallowing
- Skin: erythematous–dusky maculesstart on trunk, spread to head/limbs, coalesce casein epidermal detachment
- Mucosa:erythema,erosions, haemorrhagic crusting
HLA types - Carbamazepime HLA B1502 - Allopurinol HLA b5801
Rx • STOP culprit drug/s
- Admit ICU with MDT input • Supportive care • Gentle handling, barrier nursing
- Treat secondary infection
- Fluid/electrolyte management + nutritional support
- Skin + mucosal care: dressings, emollients, eye drops • Systemic treatment – controversial
SJS VS TEN VS Erythema multiforme
Morbilloform drug reaction
- Most common drug causes: penicillins, cephalosporins, sulfonamides, aromatic anticonvulsants, allopurinol
- Onset typically 7-14 days after initial drug administration
- Symmetrically distributed erythematous macules and papules trunk and proximal limbs - >confluent erythema
- No mucous membrane involvement
- Itch + low-grade fever
- Resolves without sequelae 1-2 weeks
- Viral infection + drug
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS)
DRESS diagnostic criteria
• Maculopapular rash developing > 3 weeks after drug initiation • Prolonged symptoms after discontinuation of causative drug
• Fever
• LFT abnormalities (ALT 100 U/L) or impaired renal function
- WCC abnormalities:
- Leukocytosis >11 x 109/L
- Atypical lymphocytes >5% • Eosinophilia >1.5 x 109/L
• Lymphadenopathy • HHV-6 reactivation
Commonly implicated drugs:
- Allopurinol
- Anticonvulsants
- Antibiotics – trimethoprim- sulfamethoxazole, minocycline, vancomycin, penicillins
- Antiretrovirals
- Ibuprofen, aspirin
- Onset after drug initiation: 2-6 weeks
- HLA-B*31:01 & carbamazepin
Mx: STOP drug, oral prednisolone tapered over 6-8 weeks
HLA typing associated with risk SJS with Carbamazepine
HLA B 1502
Fixed drug eruption
Well-defined round-oval erythematous patches -> purple/brown. May blister
Recurs at the same site/s each time drug is administered
• Mucosal & acral sites commonly affected
Onset: 30 minutes to 8 hours after taking drug
Typical agents: paracetamol, tetracyclines, sulfur antibiotics, NSAIDs
Variant: generalised bullous fixed drug
Serum sickness-like reaction
Clinical features:
- Fever, arthralgias, arthritis, rash (urticarial, morbilliform), lymphadenopathy
- Onset 1-3 weeks after drug exposure
- Most commonly due to cefaclor (1 in 2000 children)
- Other associated drugs: penicillins, NSAIDs, phenytoin, sulfonamides, minocycline, propranolol
Mx: STOP drug, NSAIDs, antihistamines ?prednisolone
HEREDITARY ANGIOEDEMA
Recurrent angioedema without wheals
Pathophysiology:
Types I & II: inadequate levels of functioning C1 inh - > excessive production of bradykinin -> inflammation with leakage of fluid through vessel walls –> oedema
Type III: (20% cases) mutation causes production of Factor XII which has increased activity. –> increased production of bradykininàoedema
Treatment:
• C1 inhibitor
• Icatibant
Congenital melanocytic Naevi
Size (projected adult size):
- Small:<1.5cmdiameter
- Medium:1.5-20cmdiameter
- Large/giant:>20cmdiameter
Giant CMN:
• 70%satellitenaevi
• 5-10% neurocutaneous melanosis
• MRI brain/spine(ideally<6/12age)
- Benign proliferative nodules common
- Increased risk of melanoma (CNS or skin)
Erythema toxicum neonatorum
Congenital pustular melanosis
Onset: birth
Clinical features: pustules without erythema -> collarettes of scale –> hyperpigmented macules (persist
for months). Skin changes can occur any region, including palms/soles
More common in infants of African descent
Diagnostic studies: Wright’s stain:
Neonatal cephalic pustulosis
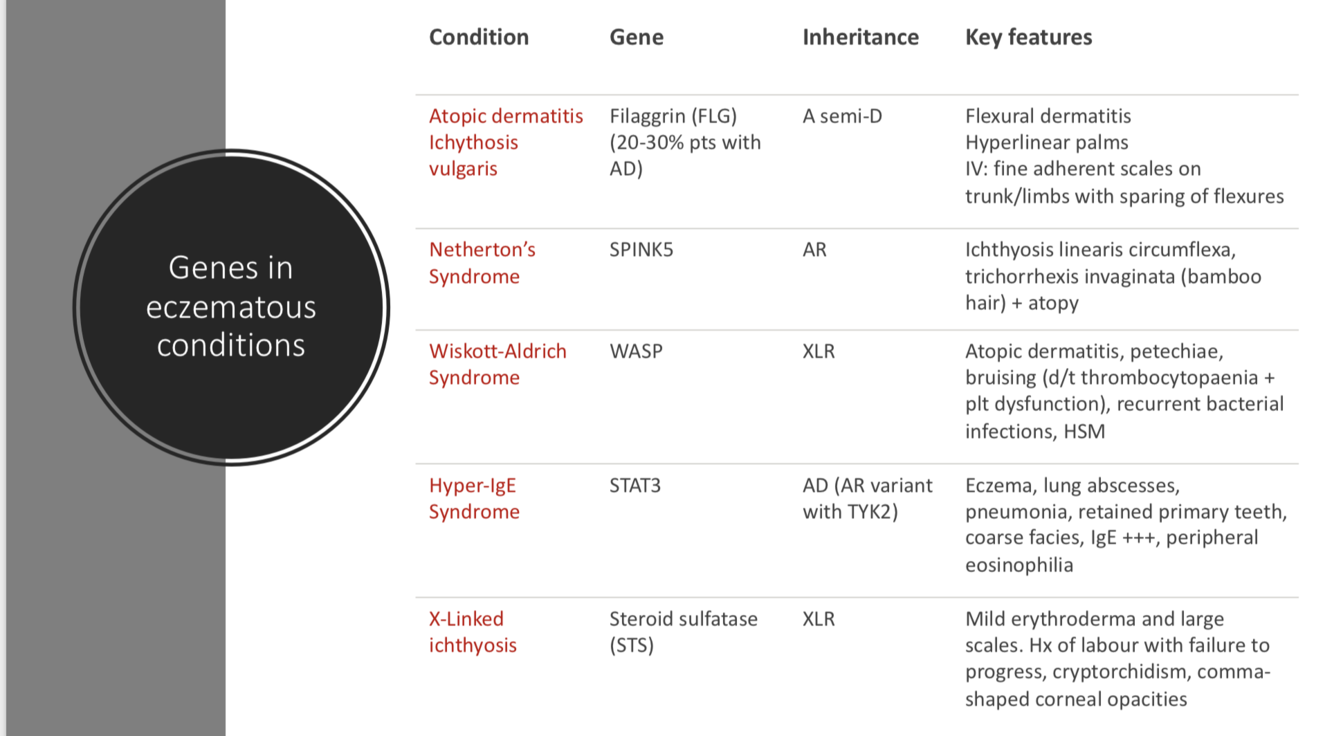
Genes in eczematous conditions
- Atopic dermatitis
- Netherons
- Wiskot aldrich
- Hyper IgE
- XL icthyosis
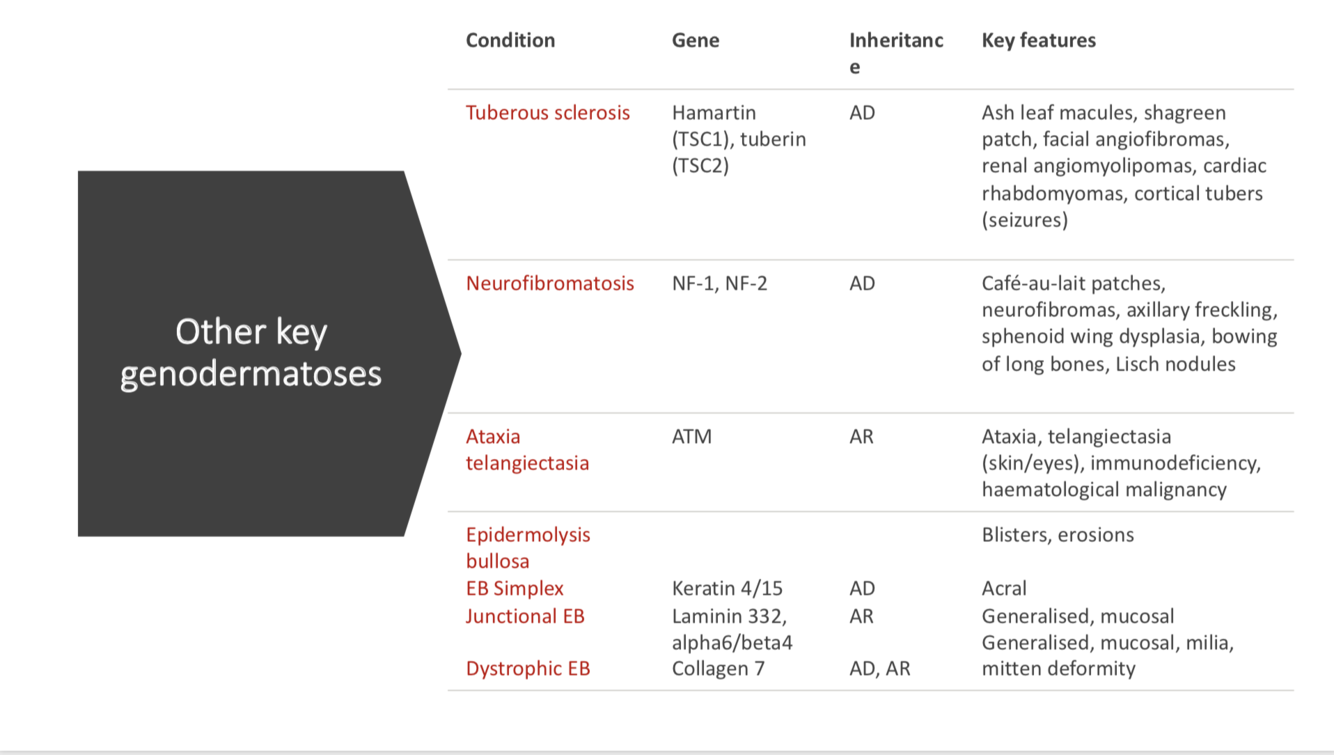
Dermatoses
- TS
- NF
- Ataxia telangiectasia
- EB
-
Resp99
-
Neonate166
-
Immunology37
-
Cardiac20
-
Gen Paed38
-
Renal91
-
Short cases108
-
Endocrine98
-
Haem96
-
Oncology97
-
Infectious Disease122
-
Statistics36
-
Cardiology187
-
Emergency Medicine129
-
Rheumatology/dermatology64
-
Genetics229
-
Metabolic124
-
Gastroenterology235
-
Cardiology COPY157
-
Neurology267
-
Derm16
-
Nephrology219
-
Psych AND Adolescent25
-
Pharmacology56
-
Pharmacology COPY145
