What cell types are present in the epidermis?
◦Keratinocytes
◦Melanocytes
◦Langerhans cells
What is the function of keratinocytes?
- Barrier Function—Stratum Corneum
- Produce cytokines and inflammatory molecules
- Produce antimicrobial proteins & lipids
- Drug metabolism
What is the function of Melanocytes?
- Pigment-producing cells of skin
- Protect against Ultraviolet radiation
What is the function of Langerhans cells?
- Macrophage-like cells in epidermis
- Important for antigen recognition
What is the function of fibroblasts? Where are they located?
- Found in dermis
- Responsible for collagen, ground substance production
What is the first step in accessing a rash?
stand back, look at the entire process, pattern, and distribution
What is a macule?
- A circumscribed, flat (NON-PALPABLE) discoloration
- Can be any color
- Few centimeters in diameter
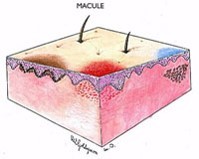
What is a patch?
- A circumscribed, flat (NON-PALPABLE) discoloration
- Can be any color
- More than a few centimeters in diameter

What is a papule?
- elevated solid lesion
- up to 1 cm in diameter
- color varies

What is a Plaque?
- circumscribed, elevated solid lesion
- greater than 1 cm in diameter
- Often formed by the confluence of papules

What is a nodule?
- circumscribed, elevated, solid lesion
- more than 1 cm in diameter

What is the difference between a papule, a nodule, and a tumor?
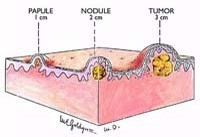
What is a tumor?
- A circumscribed, elevated, solid lesion
- Larger than a nodule
What is a wheal?
- Firm, edematous plaque
- results from infiltration of the dermis with fluid

What is a Pustule?
- circumscribed collection of leukocytes and free fluid that varies in size

What is a vesicle?
- A circumscribed collection of free fluid
- up to 0.5 cm in diameter

What is a bulla?
- circumscribed collection of fluid greater than 0.5 cm

What is the difference between a primary and a secondary lesion?
- PRIMARY LESION:
- Basic lesion that defines the disease process
- SECONDARY LESIONS:
- Lesions that evolve during the skin disease process, or created by scratching or infection
What are scales?
Excess dead epidermal cells that are produced by abnormal keratinization and shedding

What are crusts?
A collection of dried serum and cellular debris; a scab

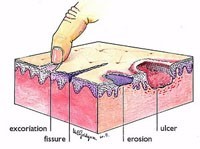
What is an erosion?
- Focal loss of epidermis
- do not penetrate below Dermal-Epidermal junction
- do not scar
What is an excoriation?
- An erosion caused by scratching
- Excoriations are often linear

What is an ulceration?
- A focal loss of epidermis and dermis
- heal with scarring

What is the difference between an erosion and an ulcer?
- Erosion: doesn’t cross DEJ
- Ulcer: loss of epidermis and dermis