What are the diagnostic indications for ECT?
- Major Depressive Episode
- Bipolar Disorder, Depressed and Manic states
- Severe unipolar depression resistant to medications
- Schizophrenia - Catatonic subtype (paranoid or other states not as effective)
- Schizoaffective Disorder
- Delirium
- Also status epilepticus that is not responsive to anticonvulsives
• Actively suicidal depressed patients who may
not live until anti-depressants work (first line, as well as catatonia, neuroleptic malignancy, previous ECT and pregnancy with severe illness)
• Depressed patients (particularly the elderly)
whose medical condition makes administration
of antidepressants risky.
• Seriously depressed patients who have had an
adequate trial of antidepressants
Which diagnoses are ECT not effective for?
Dementia and Amnestic Disorders
Substance-related Disorders
Anxiety and Somatiform Disorders
Factitious Disorders
Dissociative Disorders
Sexual Dysfunctions
Sleep Disorders
Impulse Disorders
Adjustment Disorders
Personality Disorders
What are contraindications for ECT?
No absolute contraindications for use.
• Very High Risk
– intracranial pressure (brain tumor, infection)
– Recent MI
• (Vagal arrhythmias producing postictal PVCs and extravagal arrhythmias producing PVCs anytime during the procedure)
• Moderate Risk
– Severe osteoarthritis, osteoporosis
– Retinal detachment
– CV disease (HTN, Angina)
– Recent CVA
– Pheochromocytoma
What tests should be done before ECT?
• EKG
• Chest x-ray if clinically indicated <75
• CBC, lytes, BUN, creatinine, Ca, Phos, TFTs (TSH, etc),
LFTs, UA
• Ophthalmoscopy (Fundus)
• EEG and CT generally not indicated
What is the protocol for ECT?
- Electrodes placed unilaterally or bilaterally on scalp.
- Thirty to sixty seconds of a generalized tonicclonic seizure.
- Two to three times weekly for 6-12 treatments (4 treatments after improvement).
• General Anesthesia given (methohexital/propofol), neuromuscular blockade (succinylcholine), airway with bite block, anticholinergic only if anesthesiologists deems necessary.
- Brief-pulse square-wave AC
- Voltage approx. 200V (based upon 220 Ω impedance)
- Current 0.9A
- Frequency 30 - 70Hz
- Pulsewidth 0.5 - 2 msec
- Duration 0.1 - 8 sec
- Charge 25 - 504mC (5 - 99J)
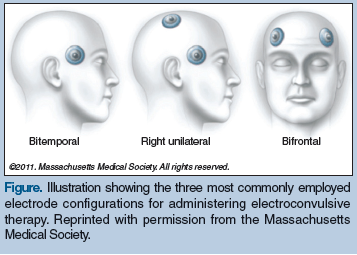
Electrode placement:
• Bilateral (BL) - most common, most effective,
most cognitive dysfunction (concentration and memory)
• Right unilateral (RUL- nondominant hemisphere) - less cognitive effect,
may be less clinically effective
• Bifrontal (BF) – may be as effective as BL
with less cognitive effect
What are the side effects of ECT?
• Amnesia (retrograde and anterograde)
– Variable after 3-4 treatments
– Lasting 2-3 months (after 6 months generally improve cognitively), elderly may have up to 6 years of amnesia
- Headache, muscle aches, nausea
- Dizziness, confusion (<1-2 hours)
More side effects from anesthesia:
– Atropine worsens narrow angle glaucoma
– Succinylcholine prolonged by pseudocholinesterase deficiency states
– Class 1A and 1B anti-arrhythmics can
interact/potentiate succinylcholine
– Methohexital can precipitate an attack of acute
intermittent porphyria (heme genetic disorder)
Which medications do and do not need to be reduced or discontinued before ECT?
Discontinue:
Anticonvulsants (except epileptics)
Stimulants
Lithium
Trazodone (increases seizure threshold)
Reserpine, chlorpromazine
Continue:
Antidepressants (SSRIs, etc.)
Neuroleptics (synergistic)
What are the alternatives to ECT?
- Pharmacologic Tx - TCA, MAOI, SSRI, SNRI, Atypical Neuroleptic, Lamictal
- Psychotherapy - CBT
- VNS (Vagus nerve stimulation, FDA approved)
- rTMS (Repetitive Transcranial Magnetic Stimulation, experimental, as effective for nonpsychotic depression as ECT)
- Neurosurgery – DBS (deep brain stimulation, experimental for failed ECT, psychosurgery, drill hole in skulle and apply directly onto brain with device on chest, used for elderly and Parkinsons, longterm)
-
Depression - Nametz19
-
Anxiety Disorders - Todder8
-
Schizophrenia - Lauden6
-
Personality Disorders - Sher13
-
Psychiatric Evaluation of the Child - Meiri4
-
Anti-Anxiety Drugs - Lauden5
-
Sexual Disorders - Ben Zion3
-
Bipolar Disorder and Treatment - Belmaker4
-
Psychodynamic therapy/CBT - Osher1
-
Electroconvulsive Therapy - Kaptsan8
-
Autism and other Pervasive Developmental Disorders - Meiri7
-
Childhood Anxiety Disorders - Lachish5
-
Post-Traumatic Stress Disorders - Matar6
-
Somatoform Disorders - Lauden5
-
Intro to Psych - Lauden6
-
Antipsychotic Medications - Lauden5
-
ADHD - Meiri6
-
Geriatric Psych - Lauden2
-
Forensic Psychiatry - Meir3
-
Eating Disorders - Schlafman3
-
Psychoanalysis - Osher3
