most common type of headache and most common presentation in docs office
The most common type of primary headache are tension-type headaches
Migraine headaches are the most common presentation in the doctor’s office
peripheral sensitization mechanism of a migraine
Peripheral sensitization: throbbing head pain that worsens with movement due to primary/first order sensitization of nociceptors of the meninges and dural vessels → normal pulsation activates the nociceptors
So, normal pulsation of intravascular pressure activates nociceptors of the dura inappropriately during migraine, whereas without migraine, normal pulsations or movements inside the head are painless.
the cortex of the brain/brain parenchyma technically cannot feel pain. What structures are pain-sensitive?
Dura mater (mostly adjacent to vessels)
Dural arteries and large veins
Pial arteria
Falx cerebri, tentorium
Venous (dural) sinuses
Proximal portions of large intracerebral arteries
CN V, VII, IX, X
central sensitzation mechanism of migraines
Central sensitization: sensitization of 2nd order nociceptive neurons in the caudal trigeminal nucleus where there is convergent input from dural nociceptors and nociceptors from the skin of the face (especially VII facial) → pain with shaving, touching skin, wearing glasses, putting the face on pillow
Trigeminovascular theory: why does the sensitization occur?
Trigeminal afferents on dural vessels release neuropeptides antidromically (CGRP, SubstP, Bradykinin)
These peptides act on dural vessels to cause neurogenic inflammation– vasodilation, extravasation of plasma proteins such as histamine → AKA NEUROGENIC INFLAMMATION
This is believed to cause sensitization of the nociceptors
outline the trigeminovasculat theory of nociceptor sensitization in migraines
Trigeminovascular theory: why does the sensitization occur?
Trigeminal afferents on dural vessels release neuropeptides antidromically (CGRP, SubstP, Bradykinin)
These peptides act on dural vessels to cause neurogenic inflammation– vasodilation, extravasation of plasma proteins such as histamine → AKA NEUROGENIC INFLAMMATION
This is believed to cause sensitization of the nociceptors
Outline how the aura is created in a migraine headahce
the aura mechanism is due to cortical spreading depression of Leao
neuronal excitation/depolarization→ increased blood flow via vasodilation→ decreased neuronal activity → decreased blood flow → spread through cortex.
CSD activates release of neuropeptides from trigeminovascular neurons and causes plasma protein extravasation leading to neurogenic inflammation.
outline the diagnostic criteria for migraine without Aura (543210 rule)
Definition: duration for 4-72 hours, recurrent (at least 5 attacks), no secondary cause identified.
Symptoms: throbbing, worse with movement, skin sensitive to light touch, allodynia
Etiology: genetic– D2 neuron receptor changes, sodium ATPase mutations etc.
Diagnostic Criteria WITHOUT Aura (most common):
Pain criteria (2 of): throbbing, unilateral, moderate or severe, worse with routine activity/movement
Associated symptoms (1 of): photophobia and phonophobia, nausea and or vomiting
**Memorization technique: 5-4-3-2-1-0:
- At least 5 attacks
- 4 hours in duration
- 3 days in duration
- 2 pain features
- 1 associated feature
- 0 other causes identified.
5 hints as to why aura from migraine is NOT a stroke:
Gradual onset of symptoms
Complete resolution
Spread of symptoms usually makes some anatomic sense with respect to cortical representation; doesn’t necessarily respect vascular territories
Often involves the tongue.
Usually more positive symptoms then negative.
4 classes of medication for acute pharmacologic treatment for migraine management
- NSAIDS
- triptans
- combo
- Anti-emetics; metaclopramide
when should you consider using prophylactic treatment in migraine management
- >8 headache attacks per month
- Recurrent migraine attacks causing disability despite optimal treatment
- Frequency of acute mediation use is >10 days/month for triptans, >15 days for NSAID, acetaminophen
- Recurrent attacks with prolonged aura
Betablockers and Antidepressants→ SSRIs not recommended, antiepileptics, riboflavin and citrate vitamins, CGRP receptor antagonists (monoclonal antibodies), botox injections
management of medication overuse headache
- withdrawal of medications must be done, 10% make an improvement.
definition and diagnostic criteria of a cluster headache
Definition: 5 attacks of severe or very severe unilateral, orbital, supraorbital and or temporal pain lasting 15-180 minutes.
- To diagnose episodic cluster, must have more than one cluster, lasting between 7 and 365 days, with a remission > 1 month.
- Most attacks last 2 wks to 3 months.
- Chronic cluster is diagnosed when attacks last >365 days without remission.
Frequency- 1 every other day to 8 per day, not attributed to another disorder and at least one of the following:
- Ipsilateral conjunctival injection/lacrimation
- Ipsilateral nasal congestion/rhinorrhea
- Ipsilateral eyelid edema
- Ipsilateral forehead and facial sweating
- Ipsilateral miosis/ptosis or a sense of restlessness/agitation
common triggers for cluster headache
etOH, nitraaets, histamine, MSOKING
abortive, transitional, preventatibe and surgical management of cluster headaches
Abortive: oxygen, triptans, nasal spray, occipital nerve block, intranasal lidocaine, possible non-invasive vagal nerve stimulation
Transitional: steroids (poor evidence), vitamin D and Ca
Preventative: verapamil, lithium, melatonin, topiramate
Surgery: deep brain stimulation (⅔ of patients benefit)
diagnostic criteria for tension headache
Definition: at least 10 episodes occurring less than 1 day per month (infrequent) or between 1 and 14 days per month (frequent), and fulfilling:
- Duration 30 min to 7 days
- Has at least 2 of the following criteria:
- Bilateral location– usually front and occipital
- pressing/tightening quality
- Mild or moderate intensity
- Not aggravating by routine activity
- No nausea or vomiting
- No more than one of photophobia or phonophobia (or else consider migraine)
- May or may not be associated with increased pericranial tenderness with palpation of pericranial muscles.
Investigations: look for depression and MSK problems
Management; physio for postural training, acupuncture, venlafaxine, amitriptyline, treat depression.
most common cause of headache in babys
Fever- meningitis, Red Reflex- retinoblastoma
most common cause of headache in child
viral
most common cause of head ache in teen
trauma/concussion
most common cause of headaache in college
meningitis, tension headache, migraine
common cause of headache in adult population
common cold, sinusitis, otitis, sinus thrombosis, dental pain, analgesic headache, shingles, trigeminal neuralgia, aneurysm
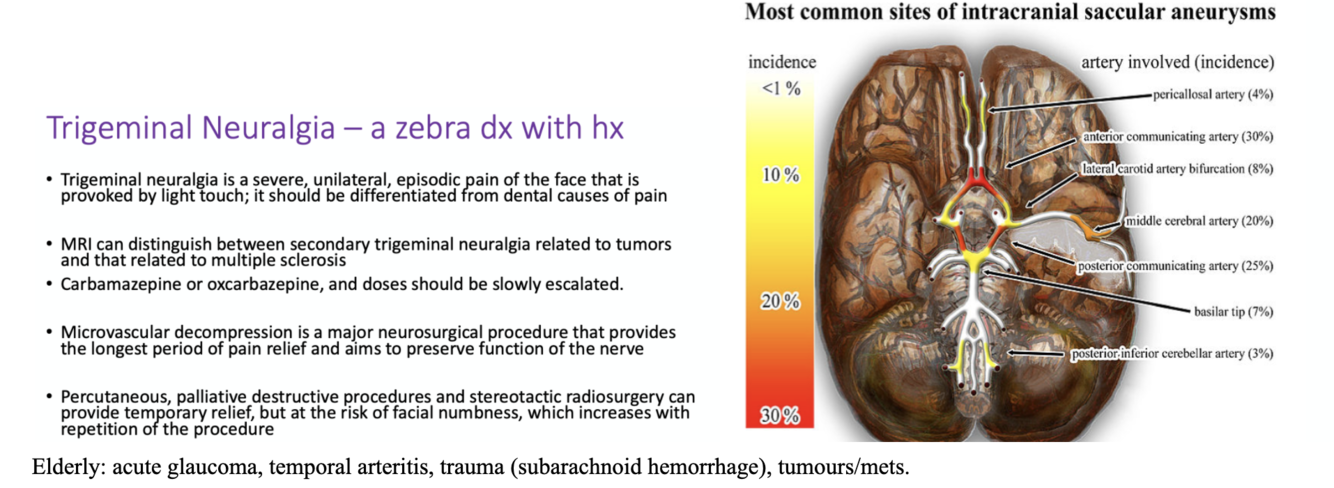
common cause of headache in elderly population
acute glaucoma, temporal arteritis, trauma (subarachnoid hemorrhage), tumours/mets.
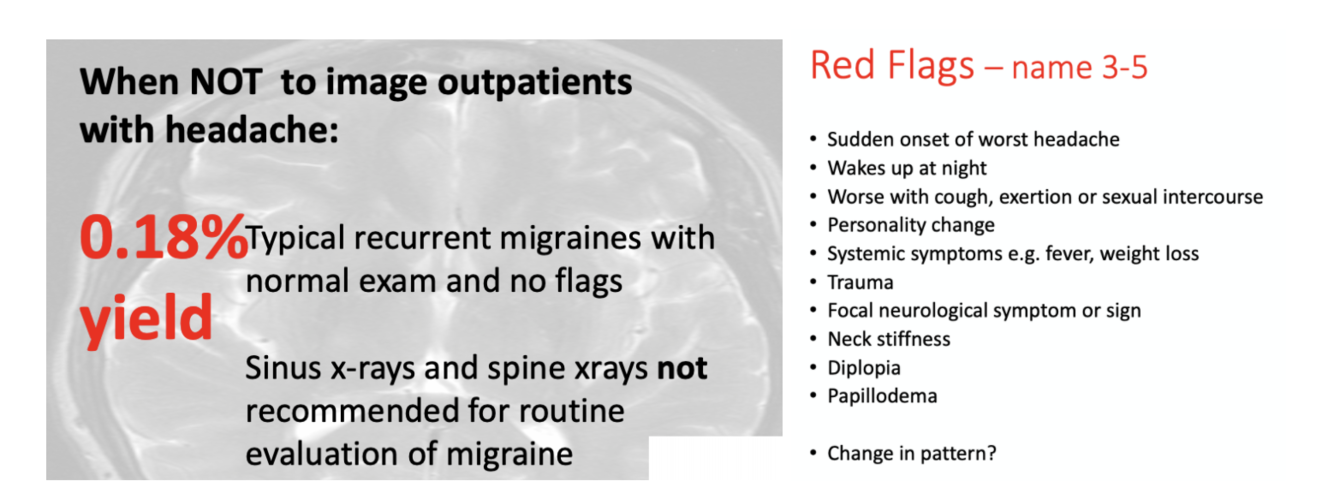
SNOOP redflags of headache that may indicate a secondary headache type over a primary
S: systemic symptoms (myalgais, amalaise, fever, weightloss), sudden onset
N: neurological signs/symptoms (diplopia, RAPD)
O: older age over 40
O: onset (thunderclap)– trauma and neck stiffness
- Thunderclap headache is a medical emergency. Could be a subarachnoid hemorrhage
Remote history of cancer
P: progressive tempo
P: pressure (symptoms of raised ICP)
- Projectile vomiting
- Morning headache
- Supine headache
- Headache with valsalva
investigations into subarachnoid hemorrahe
- emergent CTA
- lumbar puncture to look for xanthochromia from RBC breakdown
- vascular imaging with CTA or CTV
investigations into vasculitis
giant cell/temporal arteritis can cause a secondary headache in the temrporal region.
- ESR and CRP elevated. Temperal artery biopsy will show granulation and inflammation.
tx with prednisone
-
Localization of Weakness17
-
Peripheral Nervous System: Evaluation and Treatment11
-
Hyperkinetic Movement Disorders15
-
Localization in Clinical Neurology Part 116
-
Localization of Cortical Syndromes21
-
Headache25
-
Parkinsonian Disorders18
-
Bedside Approach to Speech and Language Disorders9
-
Womens Health and Neurology12
-
Sensory Systems (5 Parts)18
-
Lower Motor Neurone28
-
Cerebellum Structure and Function14
-
Bowel, Bladder, and Sexuality in Neurologic Disease3
-
Dementia24
-
Dementia: Non-Alzheimer's Disease9
-
Confusion and Delirium12
-
Epilepsy Part 119
-
Epilepsy Part 217
-
Coma Lecture23
-
Multiple Sclerosis27
-
Concussion9
-
CNS Infections31
-
Stroke Part 138
-
Traumatic Brain Injury17
-
Hydrocephalus Lecture14
-
Evaluation of Neck and Back Pain20
-
Ophthalmology: (Acute) vision loss and Ophthalmic Emergencies53
-
Ophthalmology: Diplopia and Pupil Changes15
-
Dysphonia24
-
Tinnitus and Otalgia9
-
Vertigo11
-
Brain Tumours: Neuro-Oncology14
-
Medical Management of Pain14
-
Sleep Disorders6
