define
= cardiac valves develop vegetations composed of bacteria + platelet-fibrin thrombus
suspect if: fever + new murmur
RFs
The strongest risk factor for developing infective endocarditis is a previous episode of endocarditis.
The following types of patients are affected:
- previously normal valves (50%, typically acute presentation)
- rheumatic valve disease (30%)
- prosthetic valves
- congenital heart defects
- intravenous drug users (IVDUs, e.g. typically causing tricuspid lesion)
causes [culture positive]
- historically Streptococcus viridans was the most common cause of infective endocarditis.
- This is no longer the case, except in developing countries.
- Staphylococcus aureus is now the most common cause of infective endocarditis.
- Staphylococcus aureus is also particularly common in acute presentation and IVDUs
============================================
- coagulase-negative Staphylococci such as Staphylococcus epidermidis commonly colonize indwelling lines and are the most cause of endocarditis in patients following prosthetic valve surgery, usually the result of perioperative contamination.
- After 2 months the spectrum of organisms which cause endocarditis return to normal (i.e. Staphylococcus aureus is the most common cause)
Streptococcus viridans still accounts for around 20% of cases. Technically Streptococcus viridans is a pseudotaxonomic term, referring to viridans streptococci, rather than a particular organism. The two most notable viridans streptococci are Streptococcus mitis and Streptococcus sanguinis. They are both commonly found in the mouth and in particular dental plaque so endocarditis caused by these organisms is linked with poor dental hygiene or following a dental procedure
=======================================
Streptococcus bovis is associated with colorectal cancer
========================================
non-infective: systemic lupus erythematosus (Libman-Sacks),
==============================
malignancy: marantic endocarditis
causes [culture negative]
- prior antibiotic therapy
- Coxiella burnetii
- Bartonella
- Brucella
- HACEK: Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella)
s/s
The classical diagnostic triad is:
- persistent fever
- emboli
- new or changing murmurs.
Other possible features include:
infective
- fever - may be low-grade, especially in the elderly, often with rigors;
- weight loss and anorexia;
- malaise;
- night sweats;
- clubbing after 1-2 months - now rarely seen;
- splenomegaly;
- anaemia, usually normocytic, rarely, haemolytic;
- arthritis
cardiac -
- murmurs;
- heart failure
embolic events -
- cerebral emboli producing stroke;
- mycotic aneurysm, potentially causing subarachnoid haemorrhage or affecting the popliteal artery;
- recurrent pulmonary emboli in right sided endocarditis
renal -
- haematuria from embolism with infarction;
- mild proteinuria from fever;
- nephritis usually focal proliferative but may be diffuse
vasculitic -
- splinter haemorrhages;
- Janeway lesions; Janeway lesions are painless palmar macules seen in patients with infective endocarditis. They are very rare.
- Roth’s spots; =superficial retinal haemorrhages with red edges but pale or white centres.
- Osler’s nodes =red, raised tender nodules usually 5 mm in diameter on the pulps of toes or fingers. They may also occur on the thenar or hypothenar eminences.They are thought to be due to the deposition of immune complexes.
- vasculitis
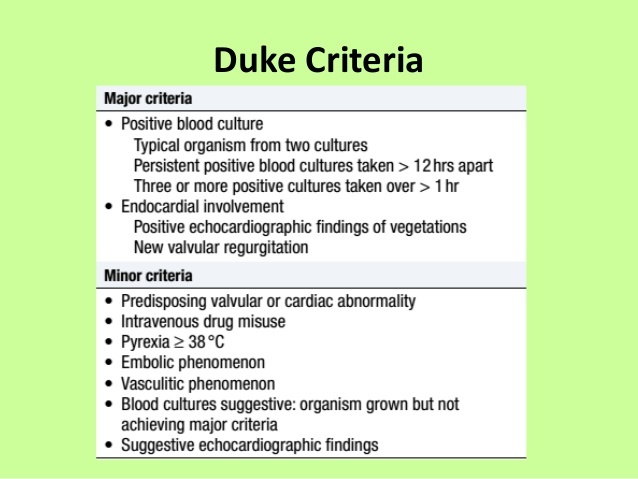
diagnosis
duke’s criteria
dx if:
- pathological criteria positive, or
- 2 major criteria, or
- 1 major and 3 minor criteria, or
- 5 minor criteria
Pathological criteria
Positive histology or microbiology of pathological material obtained at autopsy or cardiac surgery (valve tissue, vegetations, embolic fragments or intracardiac abscess content)
ix
- blood cultures
- echocardiography, cardiac doppler, transoesophageal doppler
- urine - microscopic haematuria and proteinuria are common
- blood:
🍓 normochromic, normocytic anaemia is usual; rarely, a haemolytic anaemia with positive Coomb’s test
🍓 leukocytosis is common and occasionally, thrombocytopenia
🍓 liver function tests may show increased serum alkaline phosphatase
🍓 CRP and ESR are usually raised
- chest radiology may reveal heart failure or emboli in right sided endocarditis
- ECG may reveal myocardial infarction due to emboli
- serum immunoglobulins are increased but total complement and C3 complement are decreased.
mx of acutely ill pt
- Seek expert advice.
- Antibiotics are given according to the organism most likely involved. Current UK guidelines recommend i.v. benzylpenicillin plus i.v. gentamicin as initial empirical treatment unless staphylococcal endocarditis is suspected when vacomycin is substituted for penicillin (1). If a patient is penicillin allergic then empirical treatment should be with vancomycin plus gentamicin
- Sit the patient up and administer oxygen and diamorphine - initially at a low dose. This acts as a vasodilator and reduces panic.
- Consider a diuretic - for example frusemide 40mg iv, which also acts as a vasodilator.
- Give intravenous digoxin if the patient is in AF.
- Consider replacement of the infected valve before irreversible heart damage occurs.
when would you do surgery for infective endocarditis?
Situations where urgent surgical assessment should be undertaken include :
- persistent pyrexia
- persistently positive blood cultures
- new murmurs
- recurrent emboli despite maximal antimicrobial therapy
- development of congestive cardiac failure - development of cardiac failure has a mortality of over 50% in patients with infective endocarditis managed with medical treatment alone
- large vegetations
- persistent vegetation after a major systemic embolus
- evidence of an intracardiac abscess
- worsening renal failure may necessitate consideration of surgical intervention rather than continuation of medical therapy
Absolute indications for surgery include acute valvular regurgitation with pulmonary oedema, dehiscence of a prosthetic valve, and abscess formation
Timing is critical. Ideally, infection should be eliminated beforehand but this has to be balanced against the risk of leaving the heart in a compromised haemodynamic state.
There is a 10 to 25% mortality for patients undergoing surgery during the acute phase.
prophylaxis of IE??
NICE recommends the following procedures do not require prophylaxis:
- dental procedures
- upper and lower gastrointestinal tract procedures
- genitourinary tract; this includes urological, gynaecological and obstetric procedures and childbirth
- upper and lower respiratory tract; this includes ear, nose and throat procedures and bronchoscopy
The guidelines do however suggest:
- any episodes of infection in people at risk of infective endocarditis should be investigated and treated promptly to reduce the risk of endocarditis developing
- if a person at risk of infective endocarditis is receiving antimicrobial therapy because they are undergoing a gastrointestinal or genitourinary procedure at a site where there is a suspected infection they should be given an antibiotic that covers organisms that cause infective endocarditis
-
ACS23
-
MI complications9
-
Anaphylaxis3
-
Atrial fibrillation3
-
HTN7
-
SVT3
-
HOCM5
-
hypothermia1
-
1ry pulmonary htn4
-
heart failure20
-
scoring systems25
-
infective endocarditis10
-
hyperlipidemia17
-
ix and mx of suspected angina pectoris11
-
DVLA: CV disorders9
-
angina11
-
rhuematic fever9
-
mitral stenosis6
-
mitral regurg7
-
mitral valve prolapse5
-
aortic stenosis9
-
aortic regurg9
-
tricuspid regurg5
-
tricuspid stenosis4
-
pulm stenosis5
-
pulmonary regurg4
-
cardiac surgery10
-
heart disease in diff systemic conditions [mostly rare]27
-
acute myocarditis5
-
cardiac myxoma4
-
dilated cardiomyopathy7
-
hypertrophic cardiomyopathy7
-
restrictive cardiomyopathy5
-
general overview of cardiomyopathyyyyy5
-
ADULT CONGENITAL HEART DISEASE16
-
marfans syndrome2
-
E-D syndrome1
