Qual a condição mais associada à virilização na infância?
CARCINOMA DE ADRENAL
Que medicação psiquiátrica está associada ao HIPOTIREOIDISMO?
LÍTIO
Laboratório clássico da deficiência prolongada de vitamina D?
(cálcio - fósforo - PTH)
- CÁLCIO BAIXO (ou normal)
- FÓSFORO BAIXO
- PTH ELEVADO
LAB do hiperparatireoidismo?
PTH alto
Cálcio alto
Fosfato baixo
Possíveis manifestações do HIPERPARA
LEMBRAR = CÁLCIO ALTO / OSSO FRACO
- Fraqueza
- Lesões ósseas
- Poliúria - LESÃO TUBULAR
- Nefrolitíase
- QT CURTO (hipercalcemia)
Quando indicar paratireoidectomia no hiperpara?
SINTOMÁTICOS
ASSINTOMÁTICOS SE…
- Idade < 50 anos
- Cálcio > 1 mg/dL acima do LSN
- ClCr < 60
- Calciúria > 400mg/24h ou Nefrolitíase ou Nefrocalcinose
- Osteoporose ou fratura
As 3 principais causas de HIPERCALCEMIA
Como diferenciá-las?
HIPERPARATIREOIDISMO PRIMÁRIO
PTH alto (ou normal-alto) / LESÃO óssea
MALIGNIDADE (PTH-rp)
PTH BAIXO / LESÃO óssea
HIPERVITAMINOSE D (SARCOIDOSE)
PTH baixo / SEM lesão óssea
Principal causa de síndrome de CUSHING?
CORTICOTERAPIA
Qual a 2ª causa de Síndrome de Cushing em crianças?
Quando suspeitar?
TUMOR DE ADRENAL (geralmente CARCINOMA)
SUSPEITAR DE MALIGNIDADE
Tumor > 6cm + VIRILIZAÇÃO
Suspeita de Sd Cushing - como fazer SCREENING?
- Teste supressão 1mg dexa → cortisol matinal > 2µg/dL
- Cortisol livre urinário 24h > 50 µg/dL
- Cortisol salivar noturno > 2 µg/dL
Testes de CONFIRMAÇÃO de hipercortisolismo?
- Dexametasona 0,5mg 6/6h por 48h → dosar cortisol plasmático após primeira e última dose
(+) se queda < 5µd/dL
- Teste do CRH
Principal causa de Insuficiência Suprarrenal
SECUNDÁRIA = SUPRESÃO EIXO HHA → suspensão abrupta de corticoterapia
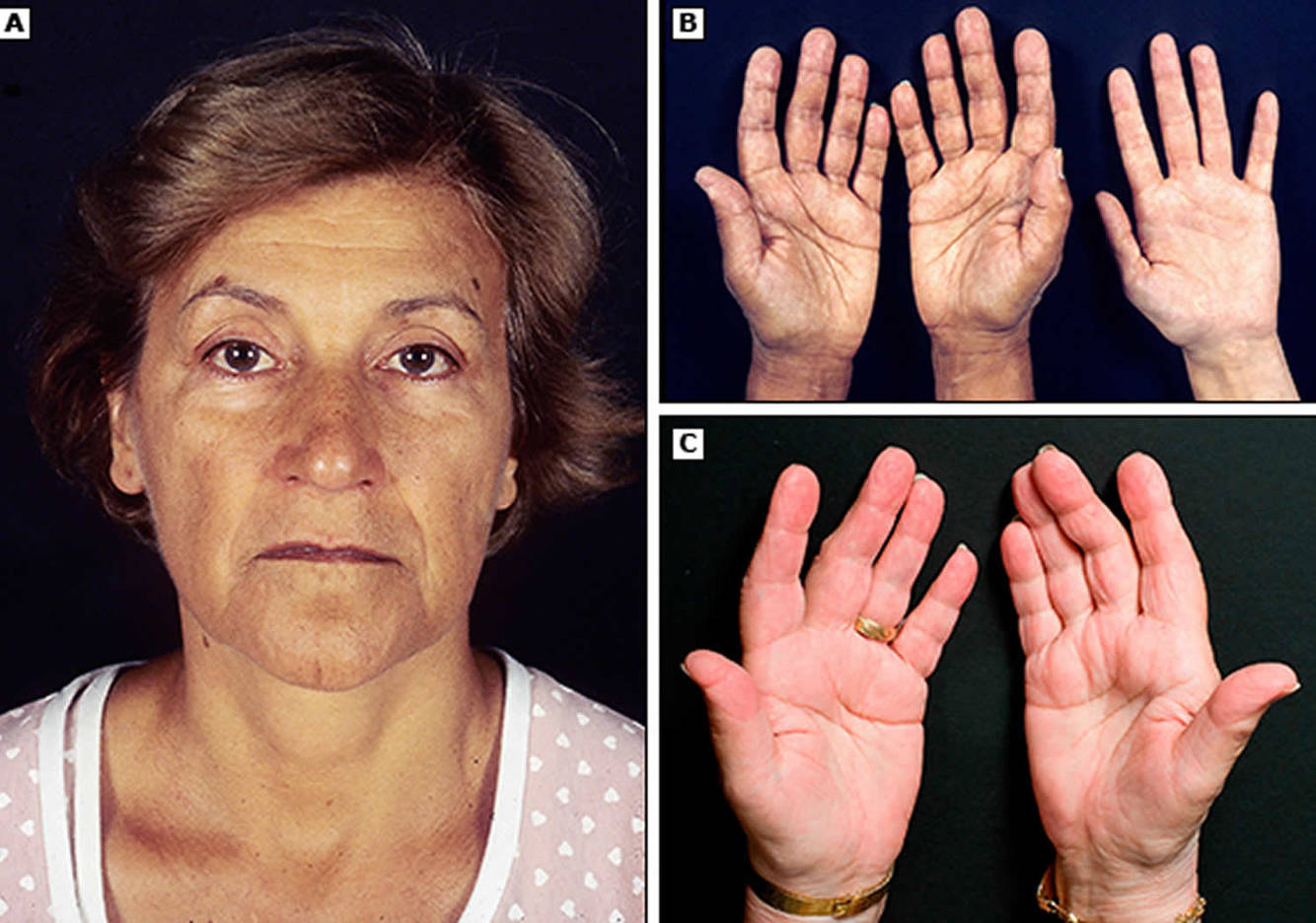
Causas para sempre lembrar diante de Insuficiência Adrenal Primária
Que achado no exame físico é característico?
- AUTOIMUNE
- Tuberculose
- Fúngica
- AIDS
- Metástases
- Síndromes poliglandulares
HIPERPIGMENTAÇÃO
Qual exame para rastreio de hipocortisolismo?
Que valor?
CORTISOL MATINAL BASAL < 3
Principal causa de HIPERPLASIA ADRENAL CONGÊNITA?
Deficiência da 21-hidroxilase
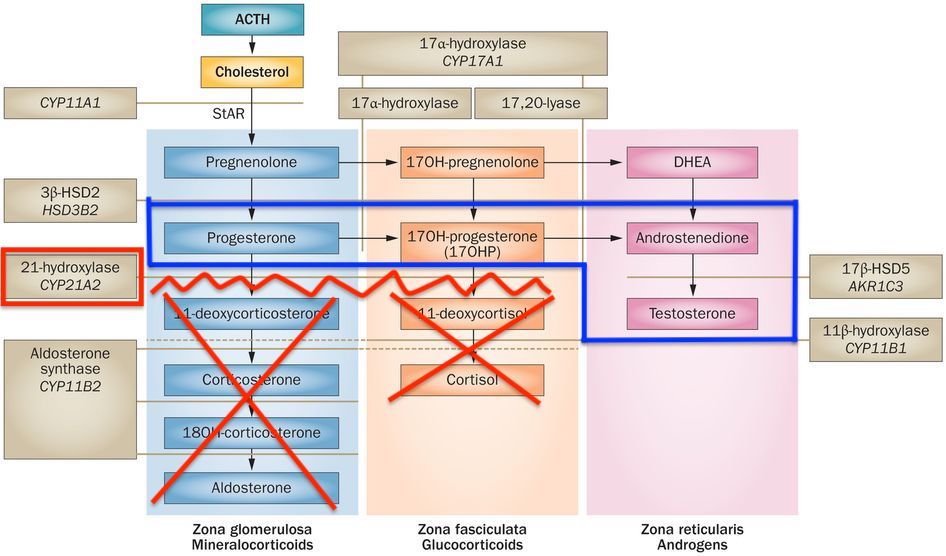
LABORATÓRIO da HIPERPLASIA ADRENAL CONGÊNITA
- Hipocortisolismo
- Hipoaldosteronismo (presente ou não)
- Hiperandrogenismo
Formas da Hiperplasia Adrenal Congênita
(1) PERDEDORA DE SAL = deficiência mais grave da 21-hidroxilase = HIPOALDOSTERONISMO associado
Perda ponderal / vômitos / desidratação
(2) NÃO PERDORA DE SAL = deficiência menos grave = possui aldosterona = manofestações do hipocortisolismo
Tratamento HAC
Reposição GLICOCORTICOIDE por toda a vida
Reposição de FLUDROCORTISONA na forma perdedora de sal
RN → pode usar HIDROCORTISONA no início (efeito mineralocorticoide associado)
Teste confirmatório na suspeita de FEOCROMOCITOMA
Dosagem de METANEFRINAS na URINA de 24h
LOCALIZAR TUMOR = TC / RNM / PET-CT
Preparo cirúrgico no feocromocitoma?
BLOQUEIO ALFA = PRAZOSINA / Fenoxibenzamina
(por 10 dias)
DEPOIS = Beta-bloqueador
NA CIRURGIA, se crise hipertensiva
(Fentolamina +- NPS + Beta-bloq IV)
