Identify those cells
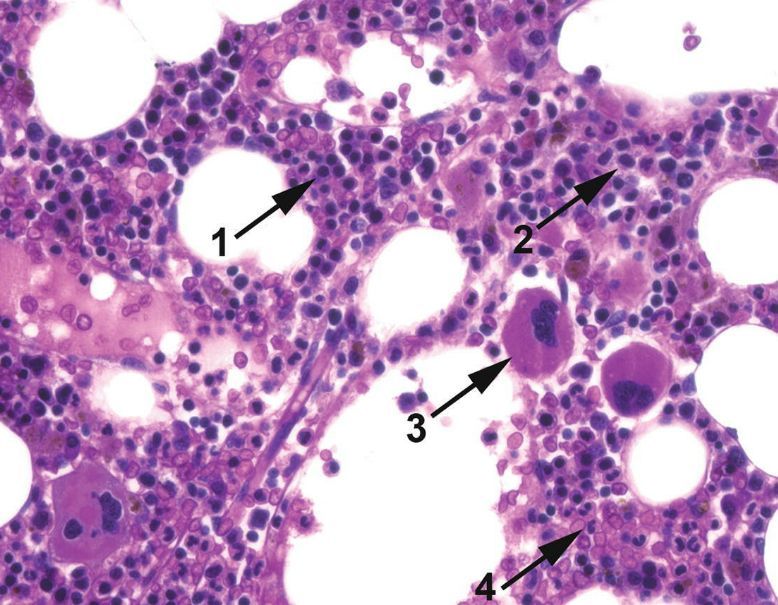
- Erythroid precursors - distinct rim of clear cytoplasm. Centrally located, round nuclei that gradually become smaller and denser as they mature. “Looks kind of like a lymphocyte” until it accumulates heme.
- Myeloid precursors - Everything else. Also accumulate granules.
- Megakaryocytes - Easy to identify.
- Maturing neutrophils - Bands, easy to identify.
Lymphoid cells in the marrow
Generally should not be seen – especially immature lymphoid cells.
Hematogones (non-neoplastic B cell precursors) are the exception and can be more frequent in children.
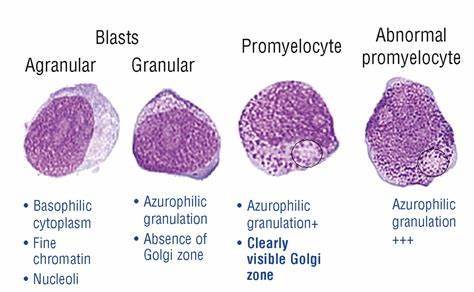
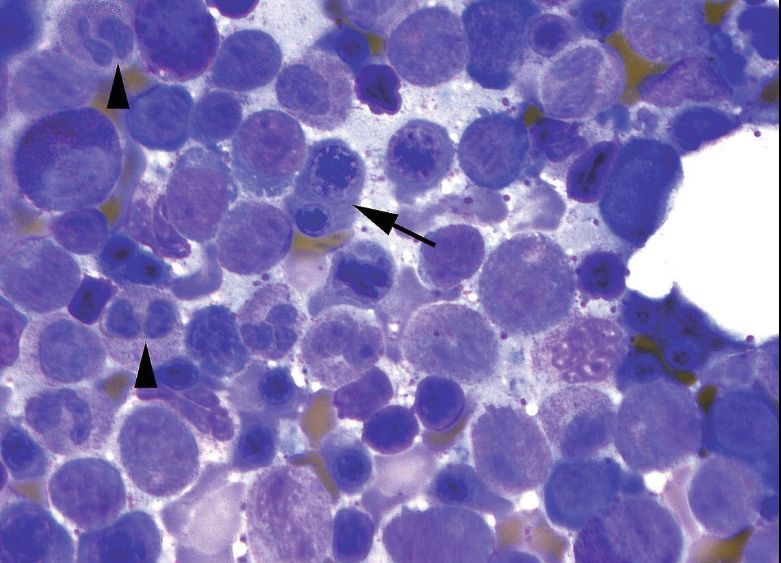
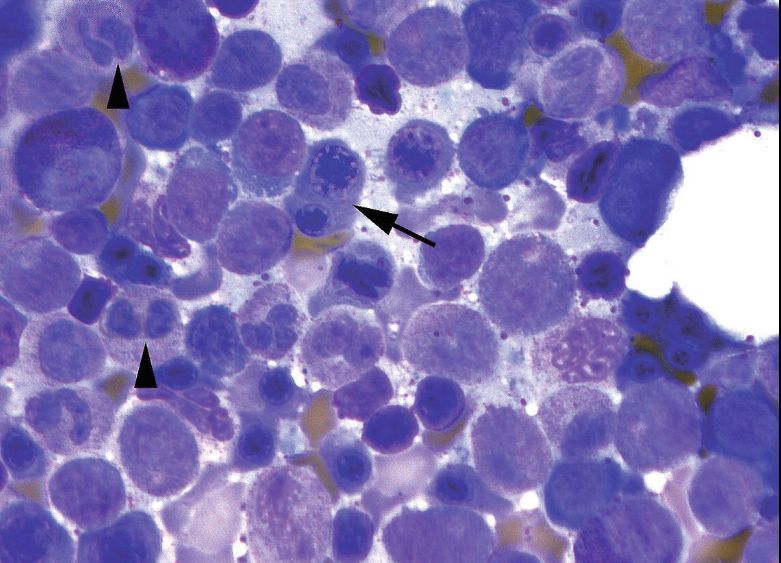
Identify the cell marked by the arrowhead
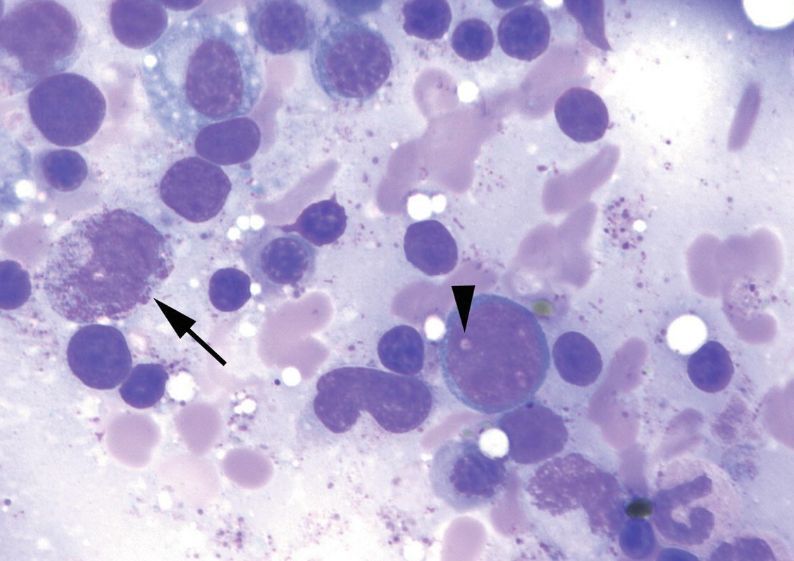
This is a blast. Note that we are on Giemsa-Wright cytology, not H and E histology.
The blast nucleus is large and round with very finely textured chromatin and a nonstaining nucleolus that shows up as a “hole” in the chromatin.
The more differentiated precursors (promyelocytes, melocytes) have similar nuclei but acquire cytoplasmic features (granules, a hof).
A normal promyelocyte should have a cearly visible. . .
. . . Golgi apparatus
The absence of this clear Golgi apparatus and increased toxic granulation suggests a dysplastic promyelocyte, such as in APML.
Nucleoli vs Vacuoles
In normal, healthy blasts, nucleoli can look lighter, almost like punched-out holes.
However, true vacuoles within the nucleus are a sign of dysplasia.
Differentiating the two is important.
Erythroblasts
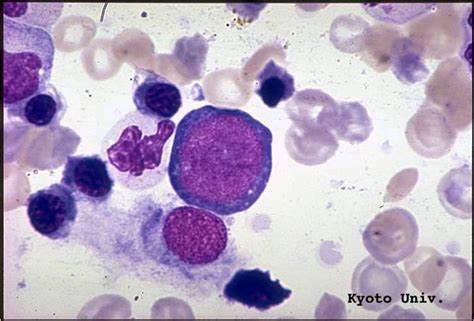
Often described as having “royal blue” cytoplasm and very round nuclei.
Estimating the cellularity of marrow
Roughly 100% - Age (for those ages ~20-70)
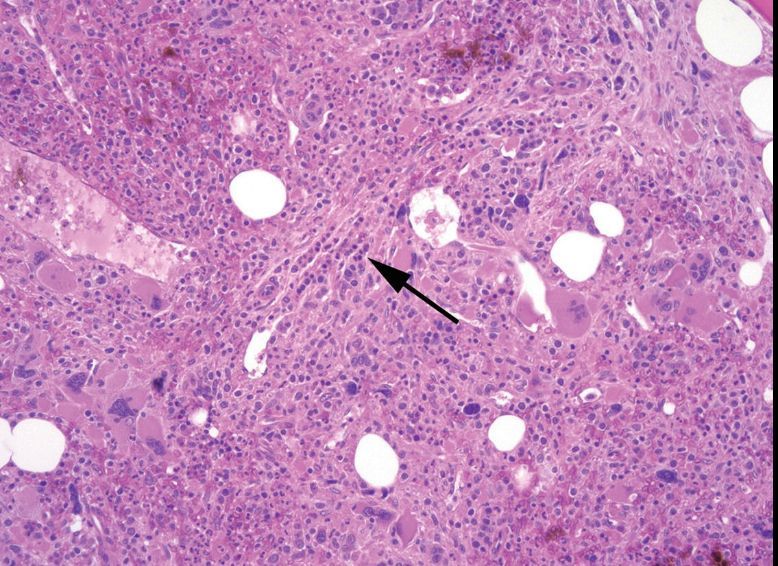
Marrow fibrosis
The marrow appears hypercellular at low power, but on high power has clear bands of fibrosis giving it a “streaming” texture.
Hematopoietic cells are divided into nests and chains.
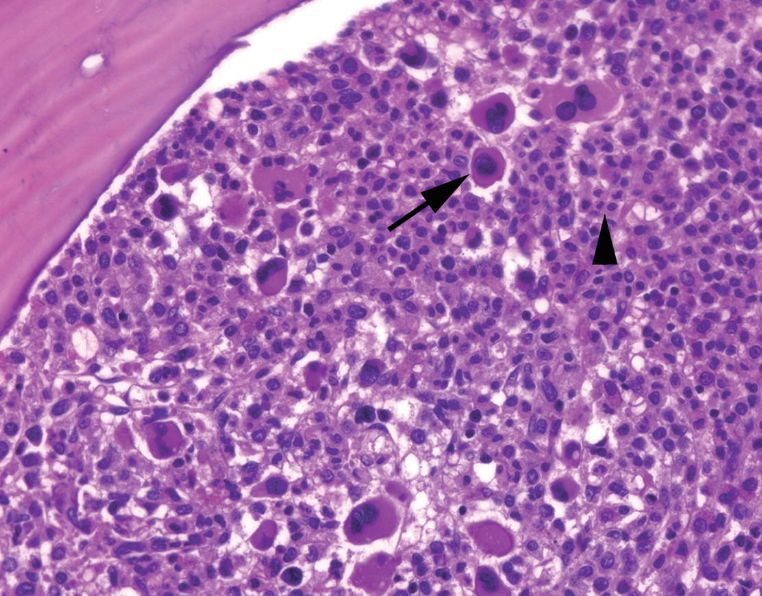
Chronic myeloid leukemia
The marrow is hypercellular and full of small, hypolobated megakaryoytes and mature neutrophils
Remember: Numerous neutrophils may indicate CML, but sheets of multiple lineages of myeloid cells may indicate infection.
Any more than __% of blasts in the bone marrow is abnormal.
More than __% of blasts is necessary for a diagnosis of most leukemias.
Any more than 5% of blasts in the bone marrow is abnormal.
More than 20% of blasts is necessary for a diagnosis of most leukemias.
Dyserythropoiesis features
- Binucleated red cells
- Red cell precursors with irregular nuclear membranes
- “Megaloblastoid change”
- A softer sign
- “Sliced salami” nuclei within mature (pale gray) cytoplasm
Dysgranulopoiesis features
- Abnormalities in nuclear lobation (“Pelgeroid”, aka bilobated like spectacles)
- Abnormal granluation (absence of granules or occasionally coarse basophilic granules)
- Hypersegmented neutrophils suggest megaloblastic anemia
Plasma cell dyscrasia spectrum
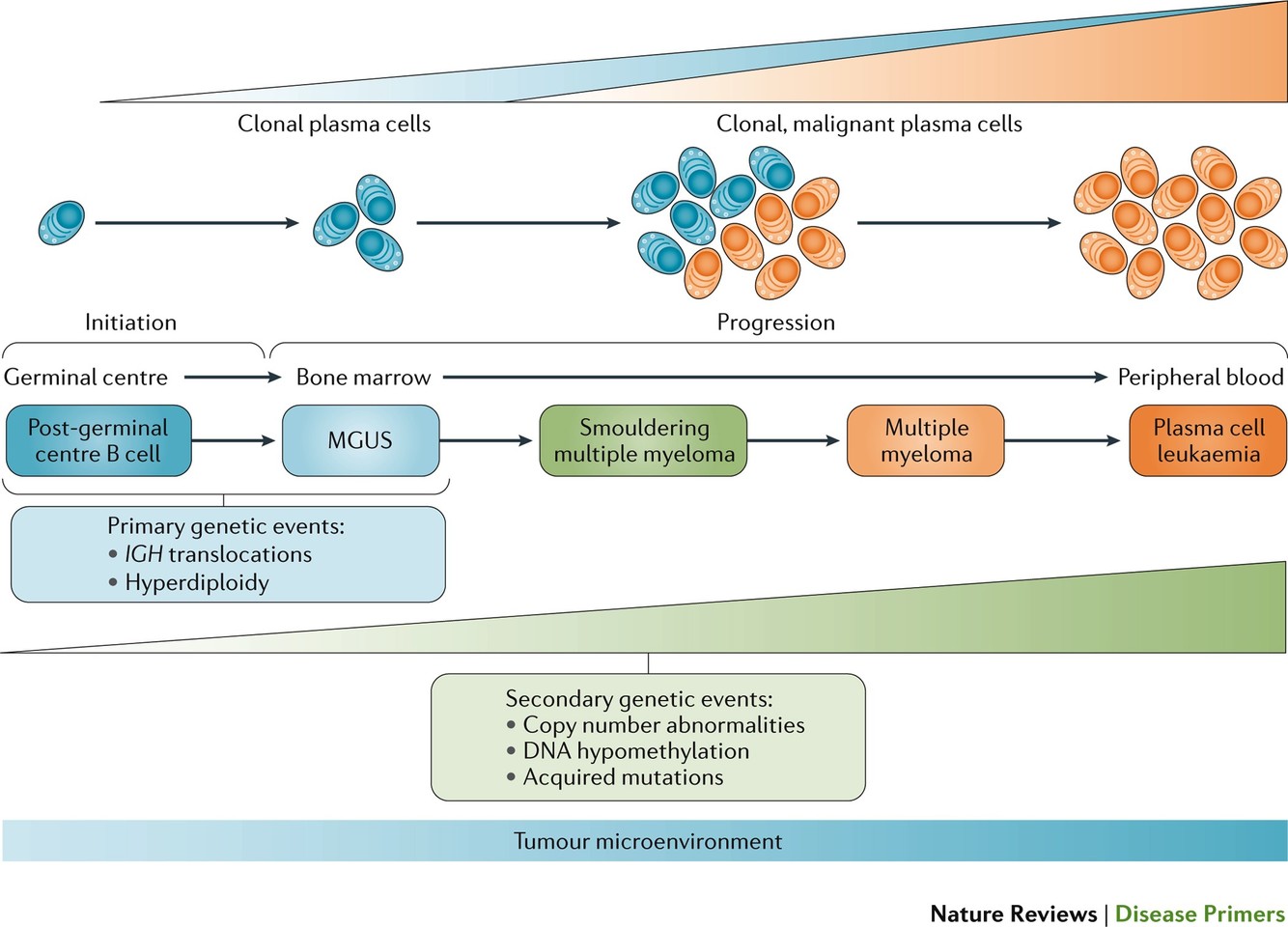
Plasma cells making up >__% of bone marrow cells indicates a possible plasma cell dyscrasia.
Plasma cells making up >10% of bone marrow cells indicates a possible plasma cell dyscrasia.
Prussian blue staining of bone marrow
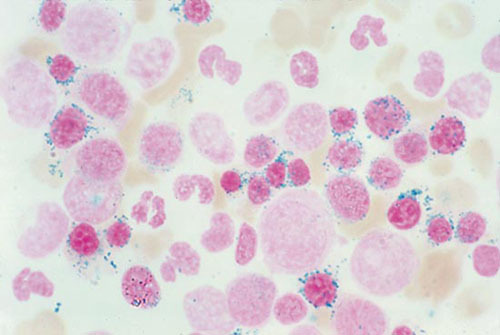
This staining shows sideroblasts. Some sideroblasts are present at baseline, but the proportion may change with pathology:
- Decreased in iron deficiency anemia
- Increased in sideroblastic anemia (especially ringed sideroblasts, shown here)
- Heritable: One of many AD or X-linked mutations in heme metabolism
- Acquired: Lead toxicity, somatic SF3B1 mutation (MDS, splicing error), B6 deficiency, Cu deficiency, Zn toxicity, some medications.
5 steps to categorizing bone marrow disorders
- What’s the cellularity? (normal/hyper/hypo)
- Is there a dominant cell line?
- Are there too many blasts?
- Are there too many plasma cells?
- Are there any lymphocytes?
Ddx for hypercellular marrow
- Physiologic response to anemia (hemolysis, infection, no dysplasia)
- Ineffective hematopoiesis (megaloblastic, HIV)
- Myelodysplasia (dysplasia in some cell line, <20% blasts)
- Myeloproliferative disorder
- Acute leukemia (>20% blasts with or without dysplasia)
- Other neoplasm (lymphoma, myeloma, metastatic cancer)
- Might present as myelophthisis
Ddx for hypocellular marrow
- Aplastic anemia
- Chemotherapy or toxin-induced
- Infection
- Hypocellular forms of myelodysplatic syndrome or AML (blasts are still increased!)
Diagnostic features of myelodysplastic syndrome
- Dysplasia of at least one cell line
- <20% blasts within the bone marrow
Blasts, MDS, and leukemia
Blast % is important in diagnosis of both diseases.
Generally, leukemias have >20% blasts as a requirement for diagnosis, and MDS must have <20% blasts to be MDS.
However, an MDS may progress to an AML, in which case blasts will go from <20% to >20%. Be aware that this transition is possible.
Nondiagnostic supportive findings of MDS
- Tend to have an erythyroid predominance in the marrow, since the body is appropriately trying to adapt to its anemia
- Decreased M/E ratio
- Ringed sideroblasts, excess blasts, or defining mutations may be involved
“MDS with ringed sideroblasts”
>15% ringed sideroblasts or iron stain
Subcategorizing a diagnosis of MDS
- “MDS with single lineage dysplasia”
- Erythroid dysplasia with anemia and <5% blasts.
- May or may not have “with ringed sideroblasts”
- “MDS with multilineage dysplasia”
- Two or more (usually three) lineages
- Dysplasia must be seen in >10% of given cell line to be significant
- <5% blasts
- May or may not have “with ringed sideroblasts”
- “MDS with excess blasts”
- MDS-EB1 is 5-9% blasts
- MDS-EB2 is 10-19% blasts OR presence of Auer rods OR >5% circulating blasts (high risk of transformation to AML)
MDS/MPN
The overlap category between MDS and MPN
Chronic myelomonocytic leukemia (CMML) is the classic example
It has dysplasia, anemia, thrombocytopenia, monocytosis, <20% blasts and NO Philidelphia chromosome.






-
Fibrotic Lung Diseases5
-
Molavi Chapter 3 - Inflammation20
-
Molavi Chapter 4 - Complex Epithelia24
-
Molavi Chapter 5 - Ditzels (Common specimens)18
-
Molavi Chapter 22 - Lungs and Pleura37
-
Molavi Chapter 24 - Thyroid and Parathyroid48
-
Hematopathology Notes9
-
Laryngeal Tumors7
-
Dermatopathology Conference16
-
Molavi Chapter 15 - Ovary34
-
Molavi Chapter 16 - Cervix and Vagina22
-
Molavi Chapter 17 - Uterus34
-
Molavi Chapter 18 - Placenta3
-
PathElective Breast Pathology37
-
General Pathology4
-
Molavi Chapter 7 - Stomach and Duodenum38
-
Molavi Chapter 8 - Colon and Appendix38
-
Molavi Chapter 28 - Skin54
-
Molavi Chapter 27 - Brain and Meninges16
-
Molavi Chapter 20 - Bone Marrow31
-
Molavi Chapter 9 - Liver40
-
Molavi Chapter 10 - Pancreas16
-
Molavi Chapter 6 - Esophagus16
-
Molavi Chapter 11 - Prostate42
-
Molavi Chapter 12 - Bladder23
-
Molavi Chapter 13 - Kidney26
-
Molavi Chapter 14 - Testis5
-
Blood Bank93
-
Molavi's Chapter 21 - Lymph Node and Spleen36
-
Platelets3
-
Blood and BM Path Chapters 2 and 3 - Normal Bone Marrow15
-
"Other" Hematologic Disorders2
-
Blood and BM Path Chapter 4 - Regulation of Hematopoiesis22
-
Blood and BM Path Chapter 5 - Pathology of the Marrow39
-
NeoGenomics Medical Flow Cytometry50
-
Blood and BM Path Chapter 18 - Acute Myeloid Leukemia52
-
Blood and BM Path Chapter 19 - Acute Lymphoblastic Leukemia/Lymphoma27
-
Blood and BM Path Chapters 20-21 - MDS and MDS/MPN31
-
Blood and BM Path Chapter 24 - CML12
-
Blood and BM Path Chapter 28 - Chronic Lymphoid Leukemias18
-
Blood and BM Path Chapter 30 - Abnormalities of Ig Producing Cells39
-
Hemoglobinopathies8
-
Disorders of Coagulation19
-
Molecular Hemepath44
-
Immunology Lab25
-
Viral Lymphoproliferative Disorders and PTLD6
-
Renal2
-
Benign Heme, Somatic hematologic mutations, Heme Ditzels3
-
Thymus7
-
Blood and BM Path Chapter 29 - Lymphoma37
-
Cutaneous Hemepath3
-
Cancer syndromes1
-
Spleen Biopsy Interpretation2
-
CHIP11
-
Neuropathology Rotation45
-
Brain Tumors I40
-
Advanced Hemepath11
-
PathElective Head and Neck91
-
T cell Lymphomas5
-
Macrophage Disorders2
-
Hematopathology Reading (Articles)3
