Major demyelinating diseases
- Multiple sclerosis
- Neuromyelitis optica (NMO)
- Acute disseminated encephalomyelitis (ADEM)
- Optic neuritis
- Transverse myelitis
Epidemiology of multiple sclerosis
- Occurs more commonly in young women
- more prevalent further from the equator
Natural history of multiple sclerosis
- demyelinating disease of the CNS
- In its most common clinical course, patients have multiple flares of symptoms at multiple time points, and recover from these attacks to varying degrees (relapsing-remitting MS)
- Later in the disease, patients with a relapsing-remitting course may enter a period of progressive decline, a scenario referred to as secondary progressive MS
- Primary progressive MS is the least common clinical phenotype of MS, and is typically a spinal cord predominant illness with steady clinical decline
- Marburg variant, tumefactive demyelination, or Balo’s concentric sclerosis presents rather with large tumor-like lesions
Initial presentation of typical MS
- Focal neurologic deficits that emerge and evolve over hours to days and usually resolve completely or near completely in subsequent days to weeks
- Can include a region of paresthesias and/or weakness, diplopia, vertigo, optic neuritis, transverse myelitis, ataxia, and/or trigeminal neuralgia
MS patients between flares
Between flares of MS, the accumulation of subclinical lesions may cause cognitive symptoms, neuropsychiatric symptoms, and/or fatigue, but progression of focal neurologic deficits between attacks is uncommon in relapsing-remitting MS.
On neurologic examination, patients often demonstrate ___ signs
On neurologic examination, patients often demonstrate upper motor neuron signs, which makes sense given that MS primarily affects the CNS.
These signs may appear even outside of regions of new or prior clinical symptoms due to subclinical lesions that have caused CNS damage without having caused clinical flares.
Classic symptoms and signs of MS include
- Uthoff’s phenomenon
- L’hermitte’s sign
- Internuclear ophthalmoplegia
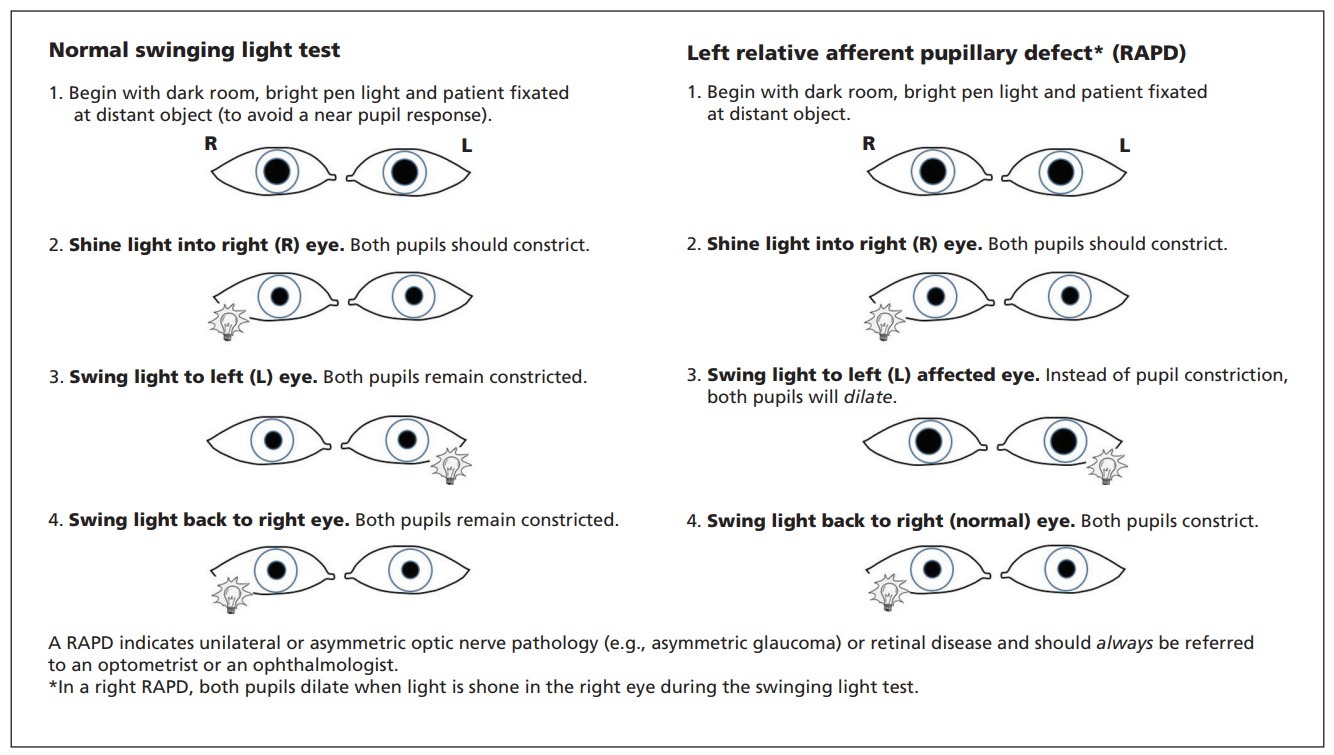
- Afferent pupillary defect
Uthoff’s phenomenon
Recurrence or emergence of neurologic symptoms with heat (due to environmental temperature in the summer, hot bath, or exercise).
L’hermitte’s sign
Electrical sensation down the spine with forward flexion of the neck.
This can occur in any type of cervical myelopathy and is not specific to MS
Internuclear ophthalmoplegia
Due to disruption of the medial longitudinal fasciculus (MLF)
Afferent pupillary defect
Due to prior optic neuritis.
An afferent pupillary defect may be present even in patients who have not had a clear clinical episode of optic neuritis
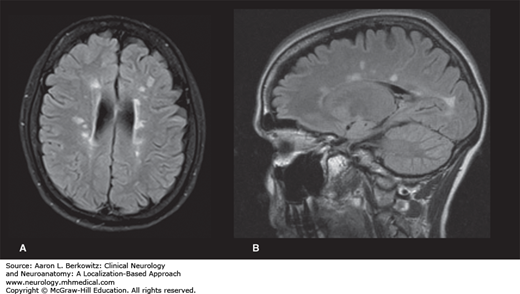
Neuroimaging of MS
- Key diagnostic test for MS
- Classic radiologic features of MS are small, ovoid T2/FLAIR hyperintensities that are perpendicularly oriented to the lateral ventricles and corpus callosum.
- Acute lesions may demonstrate enhancement with gadolinium, often in an open ring (as compared to the complete ring of contrast enhancement seen with tumor and abscess)
- The damage caused by lesions over time can lead to T1 hypointensities at sites of prior demyelination (T1 black holes).
Clinically isolated syndrome
- When a patient presents with a first demyelinating event typical of MS (e.g., optic neuritis, transverse myelitis, or another focal symptom with suggestive imaging correlate)
- If a patient has normal brain imaging in the setting of a first attack of optic neuritis or transverse myelitis, the risk of future development of MS is two to three times lower but is still in the range of 10%–30%
- Based on evidence that vitamin D deficiency may be associated with an increased risk of the development of MS, many practitioners initiate vitamin D supplementation in patients with CIS.
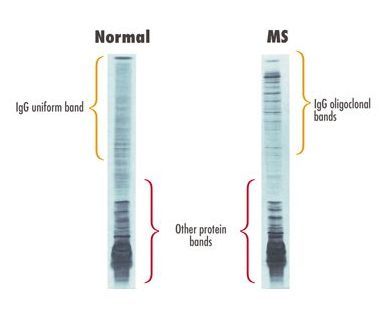
Oligoclonal Bands
- The presence of oligoclonal bands in the CSF that are not present in the serum indicates intrathecal IgG synthesis
- Nonspecific and can be seen in CNS infections and other CNS inflammatory conditions
Visual Evoked Potentials
- Examine a particular EEG of visual stimulation (P100) to evaluate conduction along the visual pathway.
- If the latency of P100 between the two eyes is significantly different, this suggests slowed conduction in one optic nerve, a sign of optic nerve dysfunction
- In cases of possible MS, abnormal VEPs can suggest prior optic neuritis.
- The optic nerve can also be examined by optical CT to look for prior damage to the nerve.
Radiologically Isolated Syndrome
- MRI performed for a different reason incidentally finds radiographic features of MS
- Such patients should be evaluated for other evidence of possible MS and other causes of CNS white matter disease (cerebrovascular disease, systemic inflammatory disease)
- This evaluation is commonly unremarkable
- Such patients are typically followed clinically and with serial imaging.
- About one third of patients with RIS will eventually develop MS and have presumably been discovered in the preclinical stage
- Empiric vitamin D supplementation recommended to reduce risk
Fulminant Demyelinating Disease
- Marburg variant MS, tumefactive demyelination, and Balo’s concentric sclerosis are names given to differing radiologic and pathologic appearances of these entities
- Biopsy is necessary for diagnosis as radiologic apperance may appear similar to other pathologies
- If steroids are ineffective in treating fulminant demyelination, patients may be treated with IVIg or plasma exchange. If these are ineffective, cyclophosphamide and/or rituximab may be considered.
Treating MS
- Acute attack rescue medications:
- 3–5 day course of IV methyprednisolone
- Preventative medications:
- Diethyl fumarate, fingolimod, and teriflunomide are all convenient oral preventative agents, often first-line for prevention
- Natalizumab (second line, mAb, anti-α4 integrin subunit)
- Injectable treatments IFN β and glatiramer acetate are favored for chronic disease
*
Fingolimod
S1P receptor agonist
Downregulates S1P receptor within the lymphatic system, preventing T cells from following the chemotactic gradient and egressing. In effect, fingolimod decreases the cycle frequency of T cells and increases the lymphatic T cell storage at any given moment.
Bradycardia and macular edema are sometimes seen. Baseline electrocardiogram (ECG) and cardiac monitoring are required with the first dose. Baseline ophthalmologic examination and subsequent periodic ophthalmologic monitoring are also necessary.
Teriflunomide
Inhibitor of pyrimidine biosynthesis.
Decreases lymphocyte proliferation.
Hepatotoxicity and teratogenicity are notable side effects. Liver function monitoring is required, and women planning to conceive require elimination of teriflunomide with cholestyramine
Natalizumab
Anti-α4 integrin subunit. Prevents T cell recruitment to regional lymph nodes.
Progressive multifocal leukoencephalopathy is a common consequence of use. PML is an opportunistic CNS viral infection caused by the John Cunningham Virus. The risk of developing PML with natalizumab treatment is related to three factors:
- Whether the patient has antibodies to the JC virus
- Whether the patient has received prior immunosuppressive therapy
- Length of treatment with natalizumab beyond 2 years
anti-JC antibody screening required. In patients who are not found to have JC virus antibodies, the risk of developing PML is exceedingly low. Given these risks, JC virus antibody–negative patients on natalizumab therapy must be screened for JC virus antibody every 6 months to evaluate for seroconversion
Symptomatic Management in Multiple Sclerosis
- Fatigue: amantadine, modafinil
- Gait: dalfampridine (contraindicated if seizures or renal failure)
- Spasticity: baclofen, tizanidine, botulinum toxin
- Bladder dysfunction: anticholinergics (e.g., oxybutynin), alpha-blockers (e.g., terazosin)
- Depression: psychiatric/psychological care, selective serotonin reuptake inhibitors (SSRIs)
John Cunningham virus
One of the two major polyomaviruses.
Causes progressive multifocal leukoencephalopathy. In this disease, patients develop CNS white matter damage. May cause memory loss, poor speech, and impaired coordination.
Risk factors for developing MS
- Hypovitaminemia D
- Previous EBV infection
- Obesity
- Genetics (20-40% concordance rate)
-
Basic Neuroanatomy I: The Brain54
-
Headache62
-
Meningitis64
-
Basic Neuroanatomy II: The Spine87
-
Integration I26
-
Intro to Psychiatry25
-
Mood Disorders63
-
Mood Disorders II27
-
The Visual System32
-
Multiple Sclerosis30
-
Cerebral Cortex I and Vascular Territories49
-
Stroke and Intracerebral Hemorrhage46
-
Schizophrenia and Psychosis47
-
Basal Ganglia and Difficulty Walking66
-
Development and Autism58
-
Seizure and Epilepsy54
-
Integration II72
-
Anxiety Disorders and PTSD58
-
Cerebellum and Ataxia48
-
Brainstem and Cranial Nerves64
-
Personality Change70
-
Substance Use Disorders56
-
Eye Movements and Pupillary Reactions57
-
Brainstem Review24
-
Peripheral Nervous System20
-
Weakness30
-
Personality Disorders54
-
Pain6
-
Additional Demyelinating Diseases and Autoimmune Neuropathies14
-
Integration III1
