Incidence in ovulation induction
- Commonest complication of IVF
- Mild OHSS may affect as many as 1/3 IVF cycles
- moderate/severe OHSS estimated to affect 3.1 - 8% cycles
- Most commonly follows controlled ovarian stimulation for IVF
- Rarely follows clomiphene ovulation induction alone (<1%)
- Very rarely can occur spontaneously during pregnancy
Stages of IVF process
Controlled ovarian stimulation: -Short cycle OR Long cycle
Ovulation trigger
Oocyte retrieval
Embryonic development
Embryo transfer
Luteal phase support
Medications used in IVF
- GnRH agonists (e.g. buserelin, naferelin) – a synthetic GnRH agonist that competitively blocks the action of GnRH, preventing the release of leuteinising hormone (LH) and follicle stimulatin hormone (FSH) from the anterior pituitary gland. However, initially there is a release of FSH and LH, the so-called ‘flare effect’.
- GnRH antagonists (e.g. cetrotide) – GnRH antagonists competitively and reversibly bind to GnRH receptors in the pituitary gland, blocking the release of LH and FSH from the pituitary, thus preventing ovulation. They are rapid acting and do not have a flare effect.
- Gonadotrophins – these are available in the form of urinary-derived human menopausal gonadotrophin (hMG) or FSH (e.g. Menopur® and Fostimon®) - contain small amount LH with FSH. Recombinant preparations (rFSH) are now available (e.g. Puregon® and Gonal F®) which are ‘pure’ FSH with no LH. There is no evidence of benefit of one preparation over the other.
Principles of long and short protocols
- “Long protocols” involve starting medications in the menstrual cycle before the IVF cycle; this is often done with a GnRH agonist.
- “Short protocols” are regimens in which medications are started at the start of the menstrual cycle in which IVF is performed.
- Stimulation is achieved with human menopausal gonadotropins (hMG) or FSH and spontaneous ovulation is blocked with either a GnRH agonist (by using the initial stimulation of leuprolide) or with a GnRH antagonist.
- GnRH antagonists are preferred over GnRH agonists for the short protocol.
Long protocols
- Starts in the cycle before the cycle in which egg collection occurs
- Utilises GnRH agonist for 2–3 weeks to desensitise the pituitary. There will be an initial ‘flare’ effect.
- Down regulation is confirmed in the presence of a thin endometrium and a lower plasma estradiol level.
- Ovarian stimulation is commenced using either hMG or rFSH with USS follicular monitoring until the desired follicular response is obtained. The GnRH agonist is continued concurrently with stimulation.
- hCG or recombinant LH is administered to induce final maturation of the oocytes.
- Oocyte collection is arranged for 34–37 hours after final hCG administration.
Short protocols
- “Short protocols” are regimens in which medications are started at the start of the menstrual cycle in which IVF is performed.
- No downregulation stage to desensitise the pituitary.
- hMG or rFSH is administered in the early menstrual phase of the patient’s cycle, usually starting on day 2 or 3.
- GnRH antagonists are administered from day 5 or 6 of stimulation and used concurrently with the gonadotrophins. The GnRH antagonist prevents premature leutenisation prior to follicle maturity being reached.
- This combination of treatments continues until the follicles have reached an appropriate stage of growth on follicular monitoring.
- hCG or recombinant LH is administered to induce final maturation of the oocytes.
- Oocyte collection is arranged for 34–37 hours after final hCG administration.
Pathophysiology of OHSS
Majority cases follow hCG/recombinant LH ‘trigger’ administration after controlled ovarian stimulation
Hyperstimulated ovaries release proinflammatroy cytokines (incl VEGF)
Process: Proinflammatory cytokines cause:
- Increased vascular permeability which leads to Loss of fluid to third space (ascites/pleural effusion/pericardial effusion), Hypovolemia, Reduced serum osmolality and Na
- Vascular endothelial dysfunction which leads to: Prothrombotic state, Increased risk of VTE
- Enlarged ovaries which leads to: Abdominal pain and distension, Risk ovarian cyst rupture or torsion
Signs/symptoms of OHSS
Abdominal discomfort and distension
Leg/vulval swelling
SOB/chest pain
Nausea/vomiting
Reduced urine output
Signs/symptoms DVT/PE
Signs/symptoms ovarian torsion or ovarian cyst rupture
Investigations
- Bloods: FBC, LFTs, CRP, U+E, Coag, plasma osmolality, hCG
Justification: High Hct, high WCC, low plasma osmolality, low Na/High K+ and high Cr, can have low albumin and raised ALT/AST, clotting- high fibrinogen and low antithrombin -
Imaging: Pelvic USS, CXR
Justification: pleural effusions, ovarian size/ascites, doppler if suspected ovarian torsion
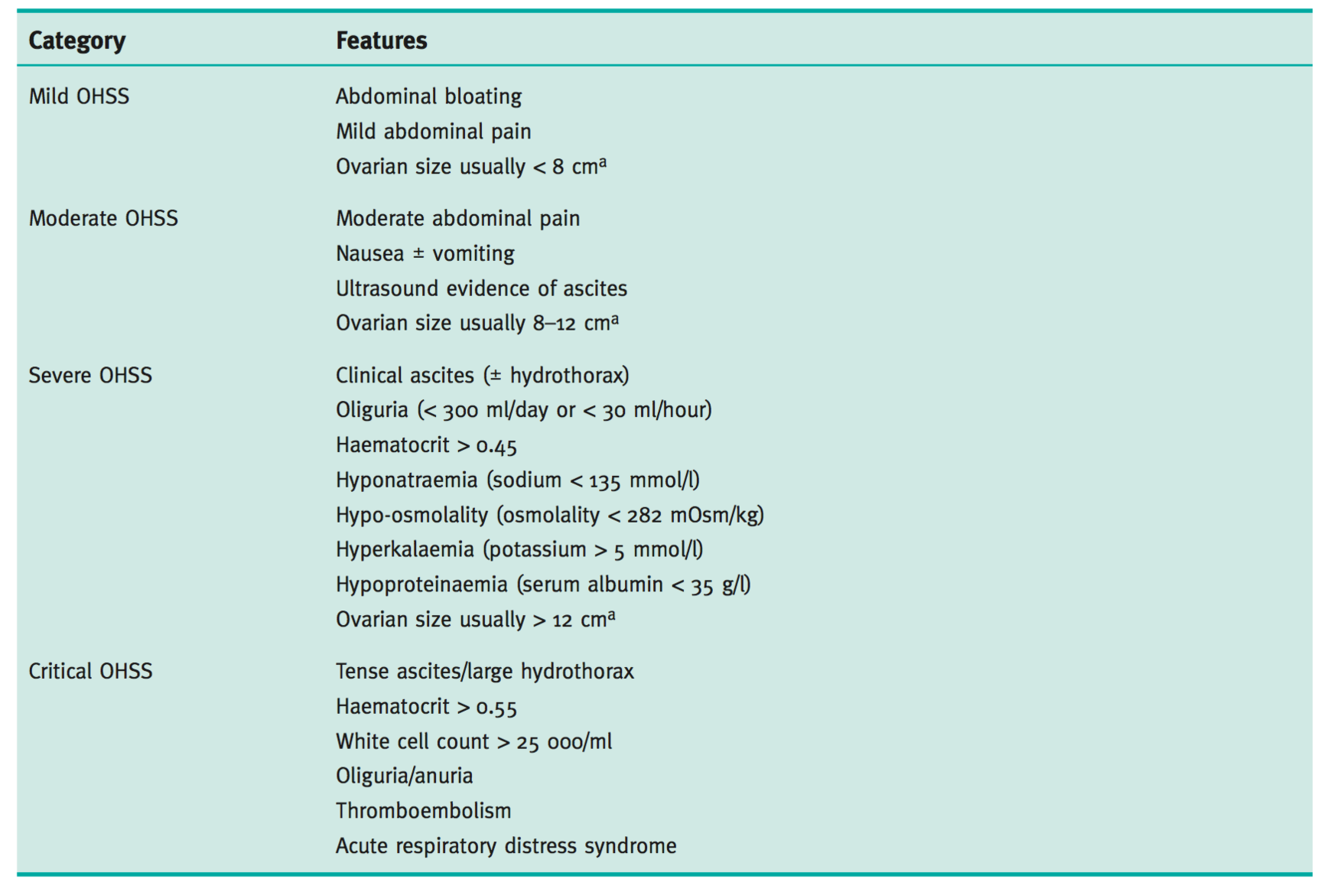
Stage of OHSS
Risk factors
- Previous OHSS
- PCOS
- High antral follicle count (AFC)
- High AMH
- GnRH agonists (long cycle IVF) used for pituitary down-regulation, as compared to GnRH antagonists
- Cycles resulting in conception (even higher likelihood if multiple pregnancy)
Management
- Supportive management
- VTE prophylaxis (LMWH for all requiring admission, severe or critical OHSS)
- Fluid balance monitoring
- Drink to thirst vs IV crystalloid fluid replacement in severe dehydration
- Human albumin solution 25% (volume expander in severe/critical OHSS)
- Drainage of ascites / pleural effusions for symptomatic relief (or if oligo-/anuria to improve renal perfusion)
- Management of complications of OHSS (e.g. PE, effusions, ovarian torsion)
- Mild/moderate OHSS can be managed as outpatient - review every 3 days
- Worsening OHSS, or severe/critical OHSS should be admitted for close monitoring
- ICU/HDU care and inotropic support may be needed (e.g. if ARDS, persistent hypovolemia, oligo-/anuria)
Criteria for admission for women with OHSS
Hospital admission should be considered for women who:
● are unable to achieve satisfactory pain control
● are unable to maintain adequate fluid intake due to nausea
● show signs of worsening OHSS despite outpatient intervention
● are unable to attend for regular outpatient follow-up
● have critical OHSS.
NB. Paracentesis can be done as outpatient and is not necessarily and indication for admission.
Pregnancy related risks for women with OHSS
pregnancies complicated by OHSS may be at increased risk of pre-eclampsia and preterm delivery
Difference between early and late OHSS
‘Early’ OHSS usually presents within 7 days of the hCG injection and is usually associated with an excessive ovarian response.
‘Late’OHSS typically presents 10 or more days after the hCG injection and is usually the result of endogenous hCG derived from an early pregnancy.
The preceding ovarian response in these women may be unremarkable. Late OHSS tends to be more prolonged and severe than the early form
Relevant features in patients history when presenting with ?OHSS
Time of onset of symptoms relative to trigger
Medication used for trigger (hCG or GnRH agonist)
Number of follicles on final monitoring scan
Number of eggs collected
Were embryos replaced and how many?
Polycystic ovary syndrome diagnosis?
Symptoms associated with OHSS
Abdominal bloating
Abdominal discomfort/pain, need for analgesia
Nausea and vomiting
Breathlessness, inability to lie flat or talk in full sentences
Reduced urine output
Leg swelling
Vulval swelling
Associated comorbidities such as thrombosis
Examination findings in women with OHSS
General: assess for dehydration, oedema (pedal, vulval and sacral); record heart rate, respiratory rate, blood pressure, body weight
Abdominal: assess for ascites, palpable mass, peritonism; measure girth
Respiratory: assess for pleural effusion, pneumonia, pulmonary oedema
Outpatient management of OHSS
- Assessment every 2-3 days
- Education regarding OHSS and complications
- Advice re. symptoms of worsening OHSS and to present for assessment if they develop
- Provide contact they can use if worsening Sx and fo advice
- Advise drink to thirst
- Ideally arrange fluid balance monitoring
- Repeat baseline tests if worsening Sx
- Signs of worsening OHSS
- increasing abdominal girth/distension
- worsening oedema
- worsening SOB/orthopnea
- signs VTE
- UO <1L in 24 hours, fluid deficit >1L in 24 hours
What are the life threatening complications of OHSS
- VTE
- Respiratory distress
- acute renal failure
- haemorrhage secondary to ovarian rupture
What monitoring is required for patients admitted with OHSS?
- Daily review and monitoring
- Weight, abdominal girth
- Fluid balance review
- FBC, U&E, LFT, serum osmolality, Hct
What are the signs of worsening OHSS?
- Increasing abdominal pain or distension
- Worsening SOB / resp distress
- Worsting oedema
- Increasing Hct
- Reduced UO - <1L in 24 hours or fluid retention > 1L in 24 hours
What is the pathophysiology of OHSS?
- Luteinisation of follicles by LH (administered exogenous gonadotrophins) and then hCG. - OHSS does not occur unless ovulatory dose of hCG is administered. - Hyperstimulated ovaries secrete VEGF leading in systemic increased capillary permeability and third spacing and intravascular volume depletion.
Define early and late OHSS:
- Early OHSS: occurs within 7 days of hCG injection and associated with excessive ovarian response. - Late OHSS: occurs within 10 days of hCG injection; usually result of endogenous hCG from early pregnancy. This form is more severe and prolonged.
