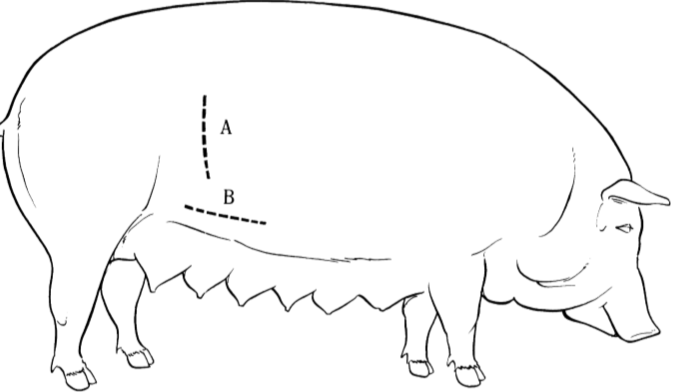
Sites for blood sampling in pigs
Depends on pig size & volume of blood req…
Sites incl :
1) Lateral auricular vv - for medication or collection of <5ml blood (collapses easily). Rubber band as tourniquet, vv at lateral/caudal margin or ear
2) External jugular - any age. 20g 1.5” in piglets, 16g 3.5” adults. Blind stick cranial to manubrium at deepest part of R jugular groove.
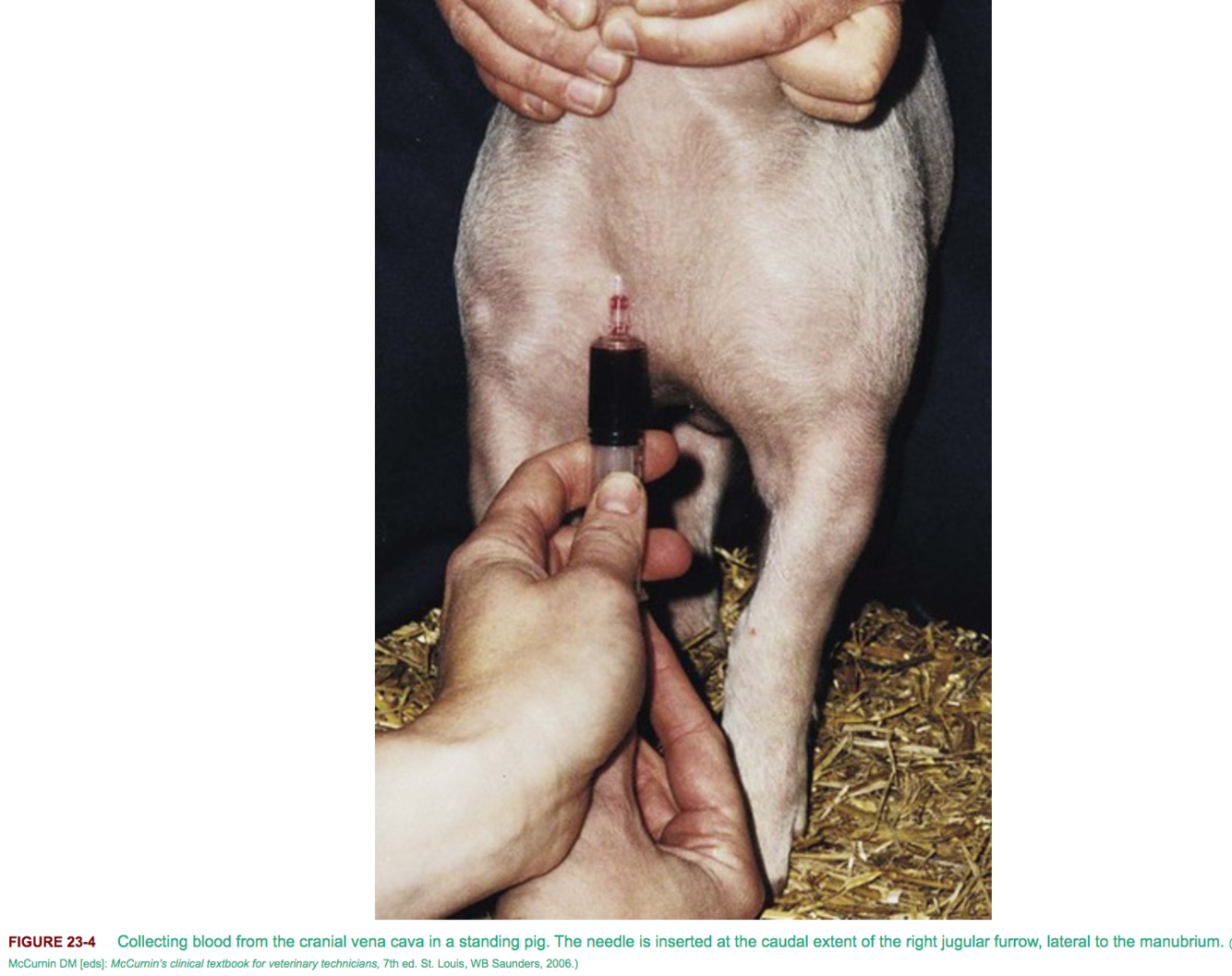
3) Cranial vena cava - located at thoracic inlet & gives rise to left & right jugulars. Technically demanding but suitable for any age & large volumes of blood collection. Always use RIGHT side (as for ext jugular) as left phrenic nn in more vulnerable position. Smaller pigs restrained in dorsal, larger standing w head elevated. 1.5” needle in small pigs, at caudal extent of R jugular furrow, just lateral to manubrium. 18g 2.5” (finishers) or 16g 4.5” (adults) in older pigs.
4) Coccygeal vv - uncommonly used, adults only with un-docked tails & <5ml blood collected. Use 20g 1.5” needle w tail held vertically & needle inserted near base perpendicular to skin
5) Mammary vein in sows
Risk factors for gastric ulcers in pigs
Slatted floors, small feed particle size
Also stress (overcrowding, extended transport, feed withholding etc)
CSs & surgical tx for gastric ulcers
CSs incl melena, pale mms +/- inappetence, vomiting, weight loss
SURGERY:
- GA dorsal and cranial ventral midline incision from close to the xyphoid caudally
- Most common site is near oesophagus/cardia in squamous region
- Place stay sutures or elevate w Babcocks & perform gastrotomy along greater curvature
- Mucosal/submucosal ulcers, can be surgically dissected & edges electrocoagulated or ligated
- Oversew with inverting pattern
- If ulcer almost full thickness- gastrectomy recommended - close in simple continuous then inverting
- Poor px w multiple bleeding ulcers
- Omeprazole PO may decr recurrence
Common causes of small intestinal obstruction in pigs
Impaction, intussusceptions (weaners/growers), foreign bodies (esp outdorr pigs eg stones), intestinal volvulus (adults) & intestinal incarceration in hernias
Neoplasia in older & Vietnameese pot-bellied pigs (usually pets so live longer) incl GI carcinoma
Enterotomy site for FB in pig SI
As for horses; longitudinal anti-mesenteric enterotomy over or immediately oral to FB
Closure = single layer appositional pattern in young pigs, or 1 or 2 layer inverting in older pigs
Recommended small intestinal anastomosis technique in pigs (pattern, suture etc)
Single layer simple interrupted pattern recommended in younger pigs and 1-2 layer continuous (broken) w inverting oversew in older /larger pigs
Ideally monofilament absorbable
What is the most common cause of GI obstruction in pigs?
What are the diagnostic features?
Atresia ani
Present w progressive abdominal distension, poor thrift etc. NB Dx often delayed somewhat in pigs vs other spp as they can vomit, do decompress the GIT & take in enough nutrients to sustain life. Ofter 3-4 weeks at dx vs other spp; several days
NB other congenital abnormaliteis eg RV fistula in gilts- does enable them to pass faeces & may delay dx even longer
How is atresia ani treated?
circular piece of skin is excised below the tail over the bulging rectum.
The rectal pouch is identified using blunt dissection, mobilised, and tacked to the SQ before incising blind ending rectum
Suture mucosa to skin
V similar to other spp
Clinical features of rectal strictures in pigs
- Weight loss, lack of faeces & progressive abdo distension . Have an anus so pass some loose faeces past stricture & present older - ave 16-18 weeks
- Most occur as a sequale to rectal prolapse following repair or following vascular thrombosis dt ulcerative proctitis caused by Salmonella typhimurium enterocolitis
Treatment of rectal fistulas
- Circular incision around anus & perirectal dissection to cranial aspect of stricture
IF short, can resect cranially & pull to rectum caudally to suture to skin incision
- If stricture extends cranially, ventral midline lap may be req to ID cranial extent & do anastomosis
- Can anastomose proximal end of descending colon to the perianal skin incision.
- A loop of spiral colon may need to be dissected (with its vascular supply) for use in the colonic pull-through because stretching the descending colon can interfere with its vascular supply. The pull-through is accomplished by temporarily occluding the segment of spiral colon to be anas- tomosed with a Penrose drain or an atraumatic intestinal forceps. The mesenteric and antimesenteric sides are tagged with stay sutures that are used to deliver the bowel through the pelvic inlet to the perianal region. The segment of bowel used in the pull-through procedure must also be sutured to the dorsal body wall to prevent volvulus of the segment.
- Alternative is left flank lap with colostomy
Risk factors for rectal prolapse
Birth weight <1kg, male, short tails (lambs), peri-parturient period in sows, coughing, tenesmus, certain antibiotics, zearalenone toxicosis, and a diet that contains 20% more lysine than required
Treatment options and complications of rectal prolapse
- 1) manual reduction & purse string suture (leaving 2 finger opening in adults) left in place for 5-10d. Recurrence likely unless underlying cause addressed
2) If above fails or mucosa too necrotic to replace = amputation
(insert rubber tube so 2-3” protrude, fixed w 2 long needles at 90° . Exposed mucosa dissected down to inner mucosa & submucosa, & blunt dissec to create a submucosal plane toward caudal aspect of prolapse. Healthy outer segment of prolapsed tissue adjacent to mucocutaneous junction is pushed cranially, & inner segment is amputated 2-3 cm distal. The inner mucosa tacked to outer mucosa with 4x interrupted cruciates (0 absorbable) at 4 equidistant sites. Fill in the gaps, remove tube and allow to retract
- Alternative - a prolapse ring or PCV tubing is placed in the rectum with the tube’s halfway point inserted as far as the anal sphincter. A ligature or rubber band is applied over the prolapse as close to the anus as possible. Tube may require frequent manual evacuation. Necrotic prolapse falls off within 5-7d
Complications: 1) rectal stricture -
2) Bladder retroversion -
3) Small intestinal eventration - correction often not economically feasible
Management options for pigs with foot infection/P3 sepsis, or DIP/PIPj
Simialr as for cows …
1) Proper debridement of the hoof abnormality & curettage of the coffin bone lesions - lateral wall access is preferable to sole access where possible
2) Digit amputation - only for commercial growing pigs and not appropriate for HIND LATERAL claws. Circumferential skin incision at 45deg from distoaxial to proximoabaxial. Much worse px than for cows. Reflect skin proximally & excise distal & a potion of middle phalanges at 45°. If PIPj involved transect to level of distal P1. Bandage 10-14d
3) Ankylosis - Only valid tx for non commercial pigs & where hind lateral claw affected in commercials. GA - 1cm incision into affected joint. All infected & sequestered bone fragments removed. Remaining articular surface removed or destroyed w 4-6mm-diameter drill bit. Curettes to debride joint & remove all infected SCB; thorough curettage of all infected bone is critical for effective ankylosis. Tissues are extensively lavaged w normal saline, & ABx administered for 10-14 days. A drain is placed into the joint for 3 weeks. Partner claw is elevated with acrylic. Strict confinement for 8-12 weeks is needed for ankylosis to occur. Ankyloses is not essential, but resolution of infection is needed to restore function
Ideal age of castration for piglets
Ideally done at 2-3 weeks. Def before 3 weeks. Better when done on d14 vs d1
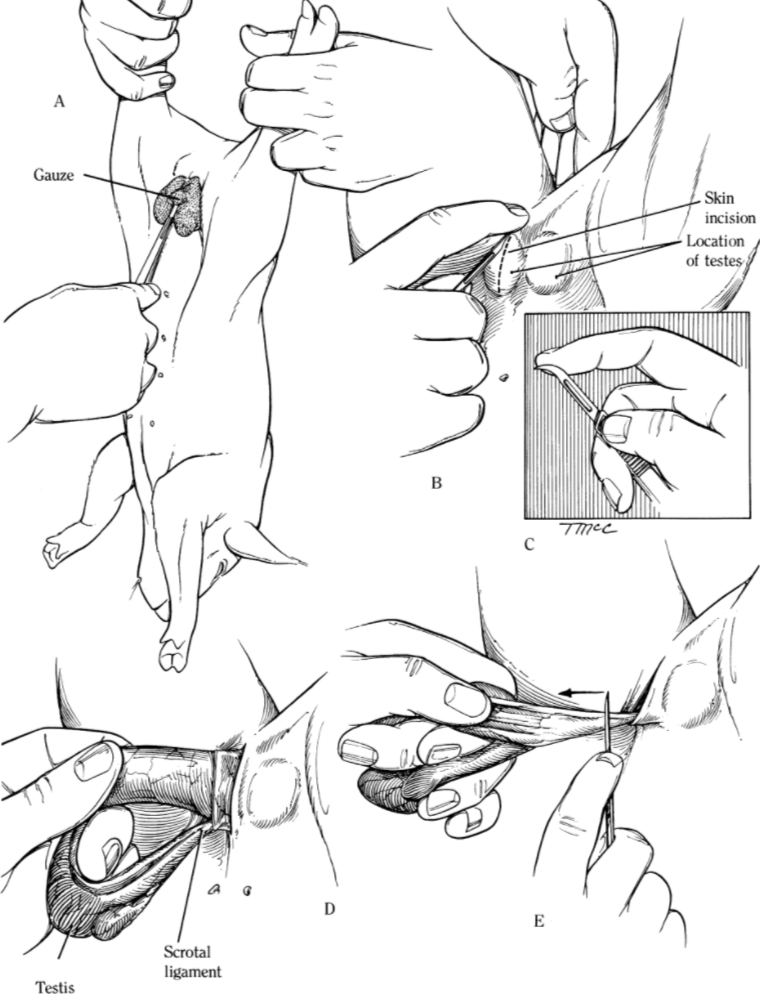
Castration technique in piglets <3weeks
- Usually concious, restrained upside down suspended from HL at hocks
- Intratesticular or intrafurnicular local (4mg/kg 2% lido)
- Testes are pushed craniad into the inguinal area - this makes incisions cranial to normal testicular position for better drainage
- Longitudinal incision through skin, SQ, & fascia made directly over each testis with 12 blade
- W blunt finger dissection, grasp the testis in 1 hand while applying sufficient traction to break the scrotal ligament; this delivers the tunic-covered testis through the wound
- If incision results in an open vaginal tunic, tunic retrieved immediately to reduce the incidence of scirrhous cord.
- Traction on the testis is maintained w left hand while a sterile scalpel blade is used to scrape and sever tunic & cord structures. Scraping should be performed as proximal as possible on the cord, so severed end retracts into inguinal region. This reduces the chances of infection & scirrhous cord. Repeat for other side
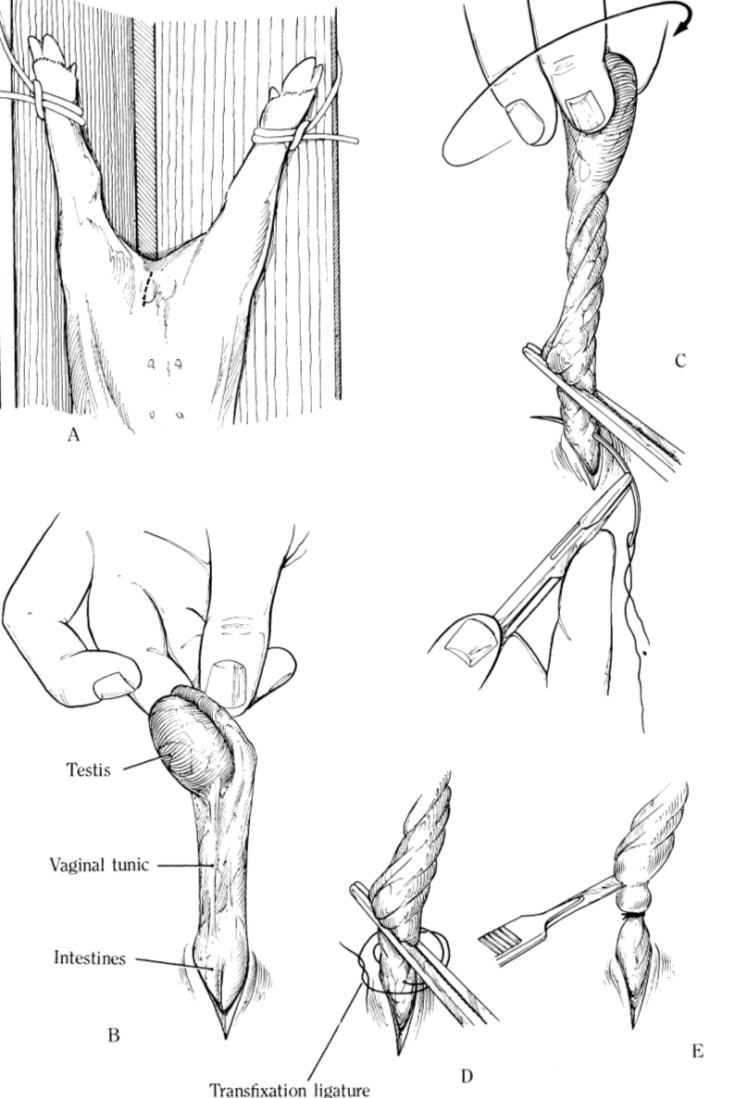
Technique for inguinal herniorrhaphy in piglets
- 7cm incision through skin, SQ, and fascia over ext inguinal ring (poss larger for larger hernias)
- The testis, spermatic cord, & surrounding fascia are isolated w blunt dissection. Steady traction is exerted on the testis, tunics, & cord, pulling them loose from their attachment in the scrotum (scrotal ligament)
- The freed vaginal tunic should NOT be incised. Grasp testis & twists vaginal sac, to return intestines to abdomen
- Kelly forceps used to grasp the sac while a transfixation ligature is applied on the proximal cord just distal to the inguinal ring w strong, absorbable suture, such as no. 0 or no. 1 syn- thetic absorbable suture
- Can anchor the hernia sac to the inguinal ring with the ends of the transfixation ligature.
- Testis and excess spermatic cord are removed
- Skin incision can be partially closed or left completely open for ventral drainage.
- Hereditary, so bilateral castration recommended.
- Hernias often bilateral so should transfix cord on opposite side to prevent PO herniation.
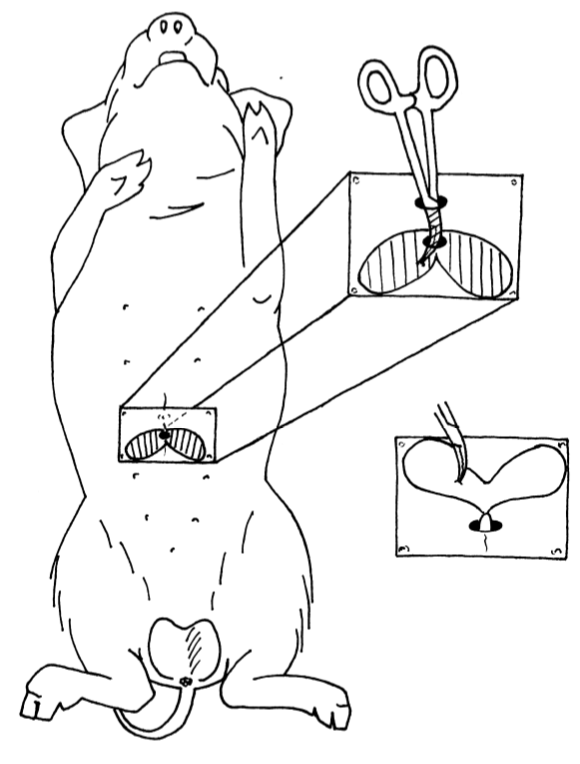
Procedure for obliteration of the preputial diverticulum
- GA dorsal.
- Diverticulum located on the dorsal aspect of the perpuce
- Sponge or oschner forceps used to outline diverticulum; usually place 2 forceps into the diverticulum, one in each lobe
- Forceps then used to grasp the deepest part of the diverticulum on each side & roll the forceps to evert the sac like diverticulum, without tearing it.
- When both sides of the bilobed structure are everted, the stalk connecting the diverticulum to the preputial cavity is ligated w a transfixation ligature of USP 1 absorbable suture being careful not to compromise the lumen of the preputial cavity
- Alt: (more involved) paramedian incision. If eversion is not successful eg tearing or scarring.
- Diverticulum packed w roll gauze soaked in ABx to help outline the structure.
- 4cm paramedian incision approx 2cm off midline over either side of packed diverticulum.
- Skin & SQ incised to expose very thin preputial diverticulum, which is then dissected free & the stalk connecting it w preputial cavity is ligated. Close dead space & SQ & skin. Care must be taken not to damage the prepuce.
Common causes of dystocia in the sow
uterine inertia; excessive adipose tissue around the birth canal; relative fetal oversize in small, immature sows; transverse presentation of a piglet; fetal monsters; and malformation of the birth canal due to previous pelvic fractures or injuries during previous parturitions (also for gnotobiotic piglets in research settings)
Technique for caesarean in the sow
- Restrain in lateral w local. Anaesthesia not desirable dt usually poor state of the sow & -ve efefcts on piglets
- For vertical incision (alt is horizontal incision 6-8cm lateral of mammary glands) - 20cm skin incision from 6–8cm ventral to lumbar TPs, midway between last rib & thigh muscles.
- Incise skin, SQ adipose tissue, mm of the flank, sub- peritoneal adipose tissue, & peritoneum.
- 15-20cm incision through uterine wall, as close to uterine body as poss,
- If the bifurcation can be located, entire litter can be brought out through 1 incision.
- If not possible, an incision is made in each uterine horn close to the bifurcation; & the piglets are removed from each horn separately.
- Great care to expose the ovarian end of each uterine horn. Its attachment is friable in the sow; and if one is not careful, the ovarian artery may be easily torn, possibly resulting in fatal haem. Explore vaginal canal for remaining piglets & to remove any loose placentae.
- Dead & emphysematous piglets usually have their corresponding placentae detached and are easily removed.
- Uterus closed with an inverting pattern. If infection present, 2-layer closure recommended.
- Uterine horns are placed in the abdominal cavity individually, making sure not twisted.
- Combined muscle & SQ layers are closed as 1, w 0 or 1 synthetic absorbable
- Continuous skin closure (supramid ford interlocking)
Location of incision for caesarean in the sow
3 basic types of incisions are used for cesarean section in sows.
- Vertical incision, in the left or right PLF/flank
- Horizontal incision in the ventral paralumbar area, 6–8 cm above the well-developed mammary tissue
- Ventral midline incision; allows access to both uterine horns; but it is awkward to position the sow for this incision, & some concerned re potential disruption by piglets
Technique for OVH in pot-bellied pigs
- GA dorsal. Ventral midline incision from just caudal to umbilicus toward pelvic brim
- SQ fat can be dissected bluntly w sx sponges to expose linea alba (less haem vs sharp)
- A horn of the uterus is located with a finger in abdominal cavity & followed to ovary.
- Ovarian pedicle is ligated w absorbable suture.
- Uterus then followed to other ovary - ligated & transected.
- Body of uterus then ligated w transfixation & circumferential sutures caudal to the cervix.
- Uterus & ovaries removed; all ligatures are examined for haem.
- Routine closure
- Alt; OV without hysterectomy. Same goals but quicker & technically easier. But obv doesn’t prevent uterine tumors - not uncommon in older pets
-
Ch 4 Fluid Therapy28
-
Dehorning11
-
Bovine GI Surgery & Dx73
-
Bovine Musculoskeletal Dz63
-
Urolthiasis in Small Ruminants16
-
Integument3
-
Physiology/Medicine General1
-
Ch 1 general considerations7
-
Pigs21
-
Anaesthesia9
-
Bovine Respiratory22
-
Neoplasia Ch823
-
dentistry ch 915
-
Ocular dz/sx ch 1012
-
Repro32
-
Sheep general7
-
Teats/Mastitis11
