What are the mechanisms of abnormal GI motility
Shock
Surgery
Inflammatory Cytokines
Medications: Opiods
Electrolyte Imbalance –> Hypokalemia, hyponatremia, hypomagnesemia
Dehydration / Hypovolemia
Hypervolemia –> bowel edema
What is Hypermotility?
– Hypermotility
• Increased delivery to small intestine –> increased
absorption
• Decreased time for absorption in small bowel
What is Hypomotility?
• Decreased delivery to small intestine –> decreased
absorption
What are the most common indication for prokinetics?
Indications:
– Increased gastric residual volume
– Gastroparesis
What is the MOA of Metoclopramide?
Mechanism of action
- Antagonist of dopamine (D1,D2 receptors)
- Enhances anticholinergic activity (sensitizes GI system to acetylcholine) and GI peristalsis through negative feedback
- Indirect and direct effects on cholinergic receptors – Mixed 5-HT3 antagonist and 5-HT4 agonist
- PROKINETIC EFFECT IS LIMITED TO THE STOMACH
would Metoclopramide work on lower GI issues?
no.
How is metoclopramide cleared?
adjust dose based on renal and hepatic dysfunction
** heavily renally cleared
Motoclopromide notable side effects
when do you avoid use?
Erythromycin MOA
What are the adverse effect of Erythromycin?
- Qtc prolongation –> big deal, drug and dose related
- Arrythmias
- Skin reactions! –> Stevens Johnson
- Toxic epidermal
- C. diff
- INHIBITS CYP ENZYME SYSTEM
What would combination therapy cause?
diarhhea
Why would you avoid Azithromycin?
consider avoiding to induction of bacterial resistance
MOA of Naloxone
- nonselective Mu opioid receptor antagonist in brain and peripheral tissues
-
• Use as adjunct therapy if no bowel movement after ~3 days with
conventional laxatives
MOA: Methylnaltrexone
How do you adjust it?
- Peripherally acting opioid antagonist with
limiting crossing blood brain barrier
WEIGHT BASED TYPE OF A DRUG AND IT IS RENALLY CLEARED
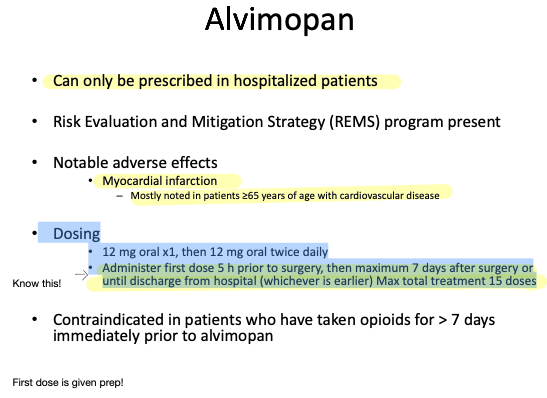
MOA: Alvimopan
first drug that reduces post-op ileus
- Peripheral opioid antagonist with limiting the crossing of blood brain barrier
- FDA labeled indication: postoperative ileus
- Accelerate time to upper and lower GI recovery after surgery including small bowel resection with primary anastamosis
- Only agent shown to decrease incidence of ileus and hospital length of stay
- Colorectal surgery and cystectomy patients not on chronic opioids
Alvimopan safety issue
MI
- first dose preOp then can maximum 7 days after surgery
Dosing
- 12 mg oral x1, then 12 mg oral twice daily
- Administer first dose 5 h prior to surgery, then maximum 7 days after surgery or until discharge from hospital (whichever is earlier) Max total treatment 15 doses
MOA: Neostigmine
Reversible acetylcholinesterase inhibitor that stimulates M2
type receptors on GI smooth muscle cell
What complications can you have from Neostigmine?
Wat are the contraindication?
- Complications: bowel ischemia, perforation (usually of cecum) – Response rates 60-90%
- Contraindications
- – Toxic megacolon
– Mechanical obstruction
- – Toxic megacolon
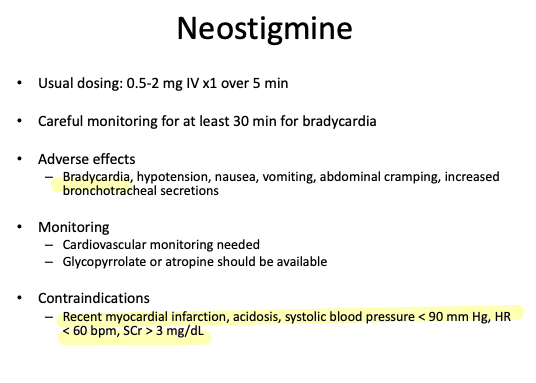
What are the adverse effects of Neostigmine?
What do you monitor?
What are the contraindication?
- Bradycardia, hypotension, nausea, vomiting, abdominal cramping, increased bronchotracheal secretions
- Monitoring
- Cardiovascular monitoring needed
- Glycopyrrolate or atropine should be available
-
Opioids, Benzos, Induction times14
-
Inhalation Agents180
-
Inhalation II20
-
IA Review Questions64
-
Chemo drugs35
-
HIV DRUGS13
-
Antimicrobial59
-
anti Fungal11
-
IA Comparison18
-
Anticoagulants72
-
Vasodilators75
-
Psychiatric Drug48
-
Anti Seizures31
-
ANS DRUGS1
-
Antacids and Acid Supressive Medication30
-
Antiematics24
-
PK lecture39
-
Benzos23
-
Opiods33
-
Induction Drugs2
-
Herbal Supplements23
-
Prokinetics21
-
DIURETICS40
-
HORMONES32
-
COPD Asthma19
