What is Psoriasis?
An inflammatory skin disorder, where you get an incraese in skin turnover due to an increase in keratinocyte turnover.
Typically there are red scaly plaques on extensor surfaces and the scalp and it is a chronic relapsing condition.
Describe the epidemiology of psoriasis, prevalence, gender, age of onset?
2% of the population
Affects men and women equally
1st age peak is 5-9 y/o in females and 15-19 y/o in males
2nd age peak of onset in 50’s
What is the aetiology of Psoriasis?
Unknown but has genetic and environmental factors
10 times increased risk if you have the HLA-CW6 gene ( codes for antigen?)
Which factors can aggravate psoriasis?
- Streptococcal throat infection.
- Drugs (beta blockers, lithium, anti-malarials and steroid rebound-withdrawal)
- Stress/emotional upset
- Smoking and alcohol
- Trauma/friction
- Sunlight (usually improves but make worse in 5%)
What are the different types of Psoriasis and which is most common?
- Chronic plaque (80%)
- Nail
- Guttate (10%)
- Flexural (inverse)
- Pustular (generalised/von Zumbusch or palmoplantar)
- Erythrodermic
Describe the characteristic features of chronic plaque psoriasis?
- Well demarkated salmon pink plaques often with silver scaling
- Plaques may coalesce.
- Most commonly on extensors, behind the ears and on the scalp.
- Usually symmetrical
- Often itchy and painful - may crack + bleed

Describe which nail changes you can see in this image?

Subungal hyperkeratosis -
is scaling under the nail due to excessive proliferation of keratinocytes in the nail bed and hyponychium.
Describe which nail changes you can see in this image?

Onycholysis
Distal portion of the nail is coming away from the nail bed.
Describe which nail changes you can see in this image?

Pitted nails
-common in psoriasis affecting up to 50% of people
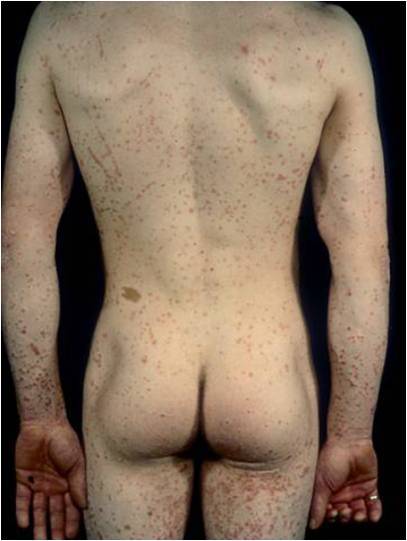
What is the Koebner Phenomenon?
Tendency for a skin condition to occur in sites in scars or along sites of trauma. AKA along excoriation lines.
Psoriasis exhibits this effect.
What form of psoriasis is shown and describe its key features?

Erythrodermic psoriasis
Erythroderma is when 90% of persons body is covered by a rash.
It is an uncommon form of psoriasis and may be caused by the rebound effect if a patient’s psoriasis has been treated with steroids.
Patient may be systemically ill and may have problems with heat, fluid and protein loss from the inflamed skin.
What form of psoriasis is shown and describe its key features?

Chronic plaque psoriasis
Plaques may coalesce as seen in the image here.
Usually the plaques will form some silvery scaling also.
It is most commonly found on the extensors, scalp and behind the ears.
What form of psoriasis is shown and describe its key features?
Guttate psoriasis
Raindrop red lesions.
It is more common in children and adolescents.
Often following a streptococcal infection
It is self resolving (months)
May precede chronic plaque psoriasis
What form of psoriasis is shown and describe its key features?
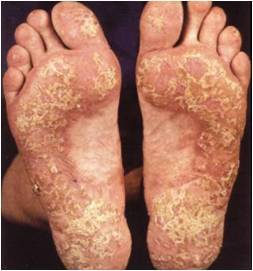
Palmoplantar psoriasis
Just affects the palms and soles.
Same characteristic features of chronic plaque.
What form of psoriasis is shown and describe its key features?

Flexural psoriasis
Only effects flexures.
Breasts folds, vulva, groin folds and axillae
Often no scaling but instead a shiny well demarkated erythematous plaque.
What form of psoriasis is shown and describe its key features?

Pustular psoriasis
2 forms: Palmoplantar (more common)
Genrealised (also known as von Zumbusch)
Palmoplantar is more common in females and adults. It is associated with smoking and is usally symmetrical but not always.
Generalised is rare, may occur with normal psoriasis and may be caused by a rebound effcet following cessation of oral steroids.
It is characterised by sheets of pustules on a background of erythema.
What is a common complication of psoriasis?
Psoriatic arthiritis affects 10%
Can present in various ways, resembling RA, ankylosing spondolitis, or just affectinng single joints
Onset 40-60 yr olds
What is the 5 step approach in managing psoriasis?
- Education
- Topical Treatment
- Phototherapy
- Systemic Treatment
- Biologicals
Discuss the topical treatments of psoriasis?
1st Line:
- Emollients
- Vitamin D3 analogues (calcipotriol) - slows production of new skin
- Topical corticosteroids - blocks harmful effects of immune system on skin
Thick plaques:
- Retinoids e.g. tazarotene
- Dithranol
Guttate Psoriasis:
- Coal Tar therapy
Which sites should you be careful of when applying topical treatments?
Scalp, face flexures.
For the scalp you can get special shampoos.
For the face or flexures you can use mild/moderate corticosteroids.
For the flexures you can also use calititrol.
Discuss the types of photodynamic therapy and the risks/side effects?
Narrow band UVB or UVA + psoralens tablets (PUVA- photochemotherapy)
Usually 3 sessions a week for 8 weeks.
Side effects:
- Erythema + pruitis (similar to sun burn)
- Nausea with the psoralen tablets
- Increased risk of developing skin cancer, greater risk in PUVA
What are the systemic agents which can be used to treat psoriasis and what are there advanatges and disadvantages?
Methotrexate:
- Advantages: Treats arthiritis aswell as skin
- Disadantages: Teratogenic, nausea and GI upset, Agranulocytosis, liver fibrosis, pulmonary fibrosis.
Monitor LFTs and FBC
Ciclosporin
- Advantages: Short term control - limit to 1-2 years (too high risk side effects)
- Disadvantages: Can cause hypertension and nephrotoxicity and gum hypertrophy.
Acitretin
- Advantages: Effective treatment
- Disadvanatge: Not for women of child bearing age as long half life and teratogenic, cannot conceive for 2 years. Cause dry skin and lips (good way to check compliance)
- Also can cause hyperlipidaemia and hepatotoxicity
What are the biological agents which can be used for psoriasis?
Only for very severe psoriasis in which all other treatments have failed (very expensive)
Etanercept (sub cut inj) and Infliximab (IV infusion) both of these are: TNF alpha antagonists
Efaluzimab (sun cut inj) monoclonal antibosy which blocks t cell activation
