what are the causes of a restrictive picture on FEV1/FVC?
fibrosis, obesity, sarcoidosis, pneumoconiosis, interstitial pneumonia, connective tissue disesase, massive pleural effusion, chest wall defects (kyphoscoliosis)
what is the KCO?
the gas diffusion coefficient: represents the carbon monoxide diffusing capacity corrected for alveolar volume
how is TLCO measured?
a single inspitation of CO held for 10s, then CO measured in the blood.
TLV is measured with a helium dilution test
what are the causes of a high and low KCO?
high - alveolar haemorrhage
low - emphysema and interstitial lung disease
what does this flow-volume loop represent?
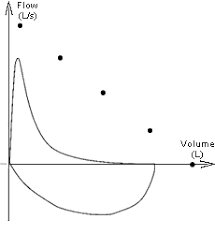
there is a characteristic defect in the expiratory phase of the flow volume loop.
This is commonly seen in intra-thoracic chest disease.
examples include asthma and emphysema
what does this abnormal flow-volume loop represent?
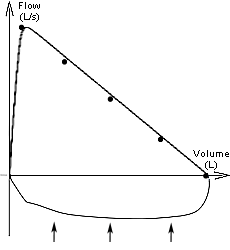
there is a characteristic pathological pattern during the inspiratory phase of this flow volume loop.
This typically represents an extra-throacic pathology.
An example would be tracheal obstruction, whereby during inspiration negative pressure the airway obstruction is sucked into the lumen reducing the flow of inspired air
what is the role of USS in respiratory medicine?
USS is commonly used to guide pleural drain insertion and pleural aspiration, especially in the case of loculated effusion/empyema
what is broncheoalveolar lavage? indications? complications?
BAL - performed during USS guided bronchoscopy. warmed 0.9% saline instilled into the distal airway and aspirated. fuild sent for lab testing.
- *indications** -
diagnostic: ?malignancy, ?pneumonia, ?bronchiectasis, ?TB, interstitial lung disease (sarcoid, pneumoconiosis, EAA)
therapeutic: alveolar proteinosis
complications
transient shadow on CXR, transient hypoxia (give O2), transient fever
infection (rare)
what are the methods for lung biopsy? when are they useful?
- percutaneous needle biopsy* with USS guidance - peripheral tumours located on chest CT
- transbronchial, performed during bronchoscopy* - interstitial lung disease (sarcoid, IPF)
what is the indication of mediastinoscopy?
for visualisation, examination and biopsy of medisatinal lymph nodes/lesions
who should be offered pneumococcal vaccine?
how frequently is the vaccine given?
- adults >65 y/o
- chronic heart, liver or renal failure patients
- DM not controlled by diet alone
- immunosupression: splenectomy, AIDS, chemo or pred >20 mg/OD
every 5 years
what are the complications of pneumonia?
lung: respiratory failure (type I), parapneumonic effusion, empyema (pus in pleural space), lung abscess
systemic: hypotension, atrial fibrilation (elderly), sepsis, death, pericarditis/myocarditis, jaundice (co-amox and flucloxacillin)
define bronchiectasis
chronic inflammation and insult to the airways leads to thinning and dilatation
what are the causes of bronchiectasis?
congenital: CF, ciliary disorders (kartagner’s), PCD
post-infectious: measles, pertussis, recurrent bronchiolitis
how do you manage bronchiectasis?
conservative: airway clearance, chest physio and pulmonary rehab
medical:
abx - treat the isolated organism. >3 exac per year, long-term nebs antibiotics
surgical:
lobectomy: maybe considered for localised disease or to control haemoptysis
consider: bronchodilators (co-existant obstructive pathology) or steroids & itraconazole (ABPA)
what is the inheritance of CF?
most common autosomal recessive condition
affect 1:2000 live births, 1:25 carry a copy of the gene
diagnosis of CF?
sweat sodium and chloride >60 mmol/L
(chloride > sodium usually)
principles of managing CF?
lung
- chest physio - frequently family/carers know best. usually in the morning, often >1 x per day
- treat infections, prophylactic Abx, test for pseudomonas colonisation
- mucolytics (DNase alpha or hypertonic saline)
- bronchodilators
- yearly CXR
- extra: mutation-specific therapy ivacaftor and lumacaftor target the CFTR protein
GI
- pancreatic enzyme replacement (CREON)
- fat-soluble vitamin supplements (ADEK)
- ursodeoxycolic acid for impaired liver function
- cirrhosis = liver transplant
other
- CF-related diabetes
- osteoporosis
- genetic councilling/fertility
median age of survival in CF?
41 years in the UK, though baby born today would expect to live longer
what lymph nodes are affected in bronchial carcinoma?
mediastinal (cannot palpate), supraclavicular and axillary
differential diagnosis of nodule on CXR?
- malignancy (1ary or 2ary)
- abscess
- granuloma (TB or sarcoid, look for lymphadenopathy)
- carcinoid tumour, other benign neoplams (hamartoma)
what must be done in the work-up for curative lung tumour resection before surgery?
PET-CT for staging
- N0 no nodes
- N1 peribronchial or ipsilateral hilum
- N2 ipsilateral medistinum or subcarinal
- N3 contralateral mediastinum or hilum, scalene or subcarinal
what is the prognosis for patients with bronchial carcinoma?
NSCLC - 50% 2 year survival without spread, 10% with spread
SCLC - 3 months if untreated, 1-1.5 yrs if treated
what are the 5 ways aspergillus can affect the lung?
- asthma (present in 1-5% of asthmatics)
- allergic bronchopulmonary aspergillosis
- aspergilloma
- invasive aspergillosis
- extrinsic allergic alveolitis

