What is a development abnormality of the thyroid?
What about from inflammation?
- Developmental abnormalities - Thyroglossal duct cyst
- Inflammation - Autoimmune thyroiditis (Hashimoto) - Subacute thyroiditis (de Quervain) - Chronic fibrosing thyroiditis (Riedel)
Hyperplasia in the thyroid is d/t
- Iodine deficiency (diffuse or nodular goiter)
- Autoimmune (Graves’ disease
What neoplasias do we see in the thryoid gland?
Neoplasia - Benign tumors (follicular adenoma)
- Malignant tumors (carcinoma, sarcoma, lymphoma, etc)
Hashimoto Thyroiditis is an autoimmune disorder, what antibodies do we see in this disease?
Anti-TPO, anti-Tg
Gross appereance of hashimotos
diffuse enlargement and very nodular looking
Lymphocytic inflammation
– Germinal centers
– Hurthle cell change
All microscopic findings in:
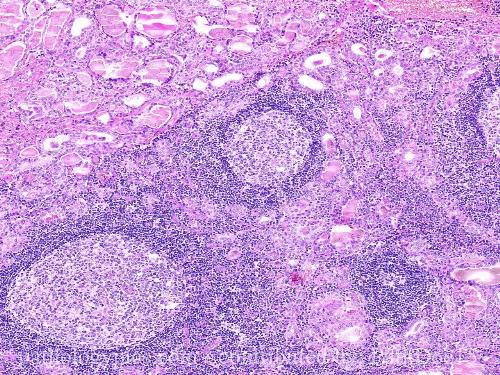
Hashimoto thyroiditis
What type of cell is in the pictuer that is seen in Hashimotos?
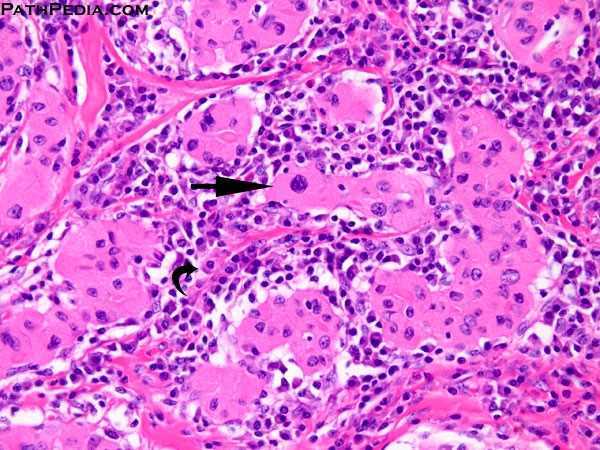
Hurthle cells; have more cytoplasm; its more pink and is dt inflammation
Suppurative (neutrophils)
Granulomatous (giant cells)
seen in what thyroid disease?
Subacute Thyroiditis (de Quervain)
Causes of Subacute Thyroiditis (de Quervain)
Viral or postviral response • Painful, self-limited disease
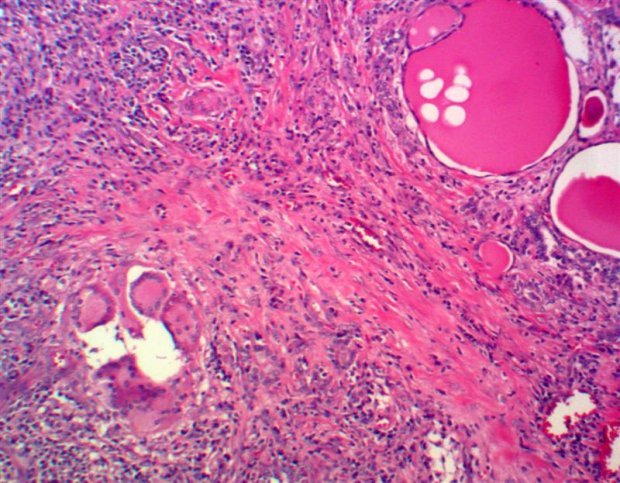
Describe Riedel or Fibrous Thyroiditis
- Hard and fixed thyroid
- Painless
– Dense fibrosis • Collagen fibers
– Fibrosis can extend outside of thyroid
seen in what type of thyroiditis?
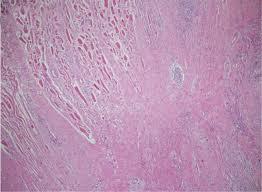
Fibrious or Riedel Thyroiditis
Autoimmune disease causing thyroid hyperplasia, most common cause of endogenous hyperthryroidism
Graves
Describe the apperance of Graves thryoid on microscopy
See irregular follicles and scalloped colloid

Histology of a Goiter
- Follicles lined by crowded_____ cells
- ____ sized follicles
- _____ colloid
columnar
Variably
Abundant
What happens overtime in pt with recurrent episodes of goiter?
Recurrent episodes lead to a multinodular gland (i.e., “multinodular goiter”) • With time will develop degenerative changes (cysts, fibrosis, calcification, hemorrhage)
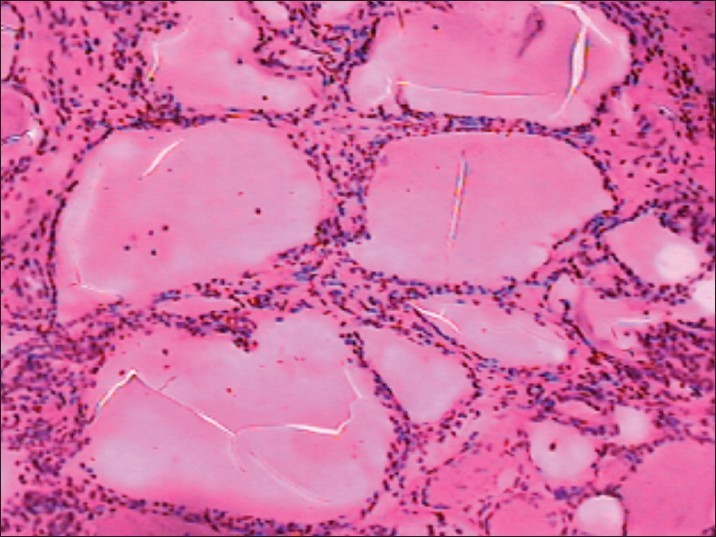
Describe the histology seen from goiter below
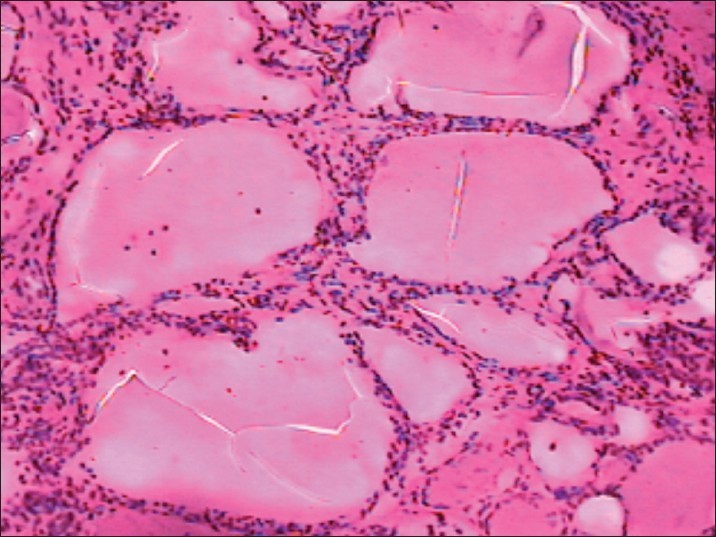
variable sized colloid filled follicles and see nodule throuhgout
How common are solitary thyroid nodules?
are they often benign or maligant?
Incidence in US is between 1 and 10%
- Four times more common in women
- Majority are non-neoplastic (focal hyperplasia, simple cysts) or benign (adenomas)
- Carcinoma is relatively uncommon (<1% of all solitary thyroid nodules)
When would a FNA be useful?
- Useful initial approach of solitary nodule
- Quick, inexpensive, minimal complications •
Can be diagnostic in papillary carcinoma, medullary carcinoma, lymphoma and metastatic tumors
What is a limitiation of FNA?
Cannot differentiate follicular adenoma from follicular carcinoma or from hyperplastic nodules
Benign neoplasm with various morphologic appearances (follicular, microfollicular, trabecular, Hurthle cell, etc.); however, this is not clinically significant
• Most are nonfunctional
Follicular Adenoma
Are we concerend about follicular adenomas progressing to cancer? What if they are funcitonal?
nope
functional = toxic adenomas and cause thyrotoxicosis
- Solitary
- Completely surrounded by a fibrous capsule – No capsular or vascular invasion
- Different growth pattern from adjacent normal gland
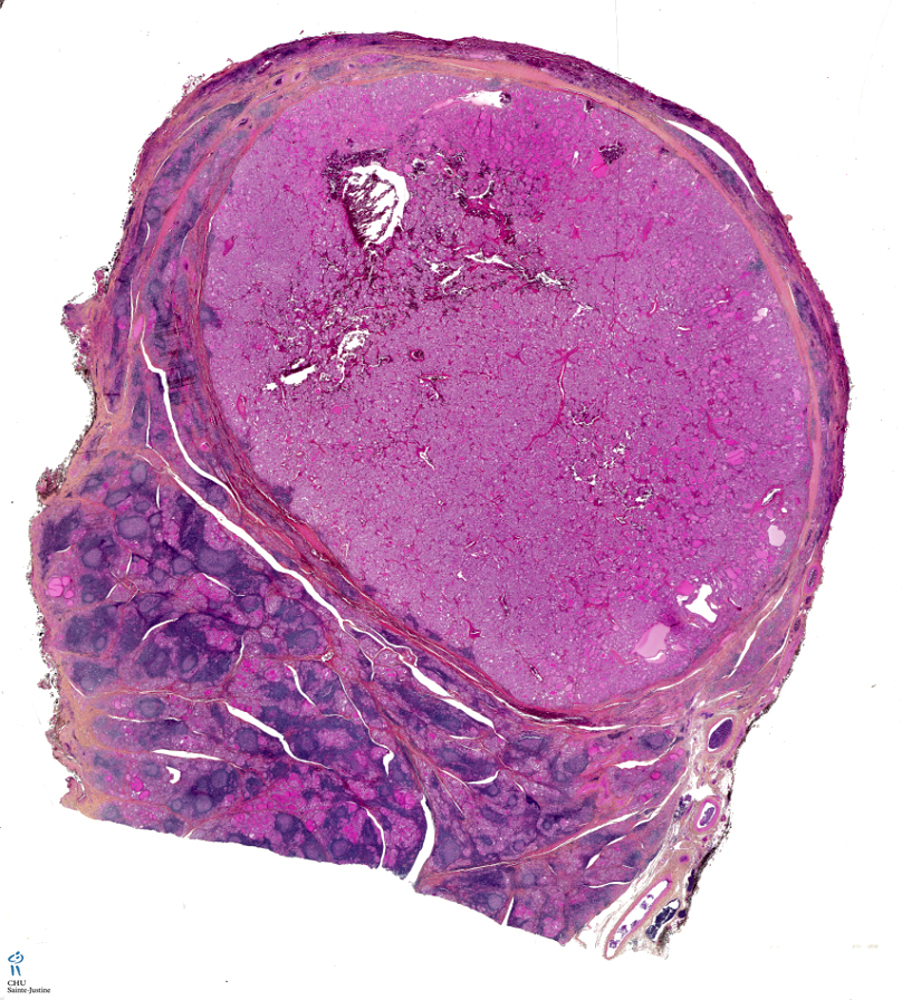
key findings of Follicular Adenoma







-
Gland histology62
-
Endocrine Devo62
-
Adrenal Insufficiency and Cushings56
-
Hypercortisolism26
-
Bone and PThyroid Path (15/16)79
-
Hypothyroidism/Hyperthyroidism49
-
Peds Thyroid issues28
-
Thyroid Pathology58
-
Diabetes physiology review36
-
Posterior PItuitary54
-
Anterior Pit (5/6)84
-
Pheochromocytoma21
-
Hyperaldosteronim36
-
Parathryoid (HYPERcalcemia)27
-
Parathyroid (HYPOcalcemia)30
-
Bone Disease (13/14)62
-
Diabetes Pharm0
-
Metabolic Sydrome29
-
MEN syndrome31
-
Hypoglycemia/insulinoma26
