What is Parsonage Turner syndrome?
Acute brachial plexus neuritis.
aka brachial neuritis, neuralgic amyotrophy
Presentation:
- sudden onset of intense pain that subsides in 1 to 2 weeks
- typically awakens people from sleep
- followed by weakness for a period of up to 1 year in the muscle that is supplied by the involved nerve
Physical exam
severe weakness of the external rotators and abductors
can have decreased sensation (up to 75% of patients)
especially in lateral antebrachial cutaneous nerve
commonly affects more than one nerve branch
outcomes
90% of patients recover full muscle strength and function by 3 years with no residual pain or deficits
only 35% of patients recover at 1 year
Name the common sites of compression of the median nerve (5)?
What symptoms/signs will the patient have?
- DIFFERS FOM AN AIN PALSY. THIS IS AKA PRONATOR SYNDROME. Should have predominantly sensory symptoms which can be provoked, also has aching pain in forearm and sensory disturbance over palm of hand which can differentiate from carpal tunnel syndrome. ALSO HAVE PRONATOR WEAKNESS and WEAKNESS OF HAND INSTRINSICS LIKE AN AIN PALSY.
Can also have hand instrinisc weakness if there is a martin gruber anastamosis (due to the takeover of ulnar innervated hand intrinsics by the median-to-ulnar connection)
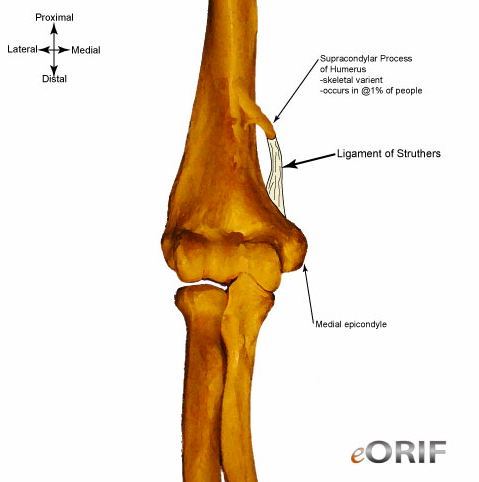
- supracondylar process of the humerus
- ligament of struthers
- Lacertus fibrosis
- between ulnar and humeral heads of pronator
- FDS aponeurotic arch (sublimis bridge)
- (then in the wrist - carpal tunnel)
Name the common sites of compression of the AIN (8)?
What is the common presentation, how does it differ from a median nerve proper lesion?
AIN compression syndrome is different from Median nerve proper lesion (aka Pronator syndrome) as there is weakness in all AIN supplied muscles (FPL,FDP 1/2 and PQ) and NO sensory symptoms.
There may be only intrinsic weakness if there is an incomplete palsy or a reverse martin gruber anastomosis (i.e Marinacci anastomosis) is present (in 15% of ppl, where Ulnar nn axon cross over to the AIN/Median to innervate certain muscle groups)
Depending on where the AIN comes off, sites of compression can be:
- edge of lacertus fibrosis
- tendinous edge of pronator teres
- FDS arch
- accessary head of FPL (Gantzers)
- accessory muscle from FDS to FDP
- Abberant mm (FCRB, palmaris profundus)
- thrombosed ulnar or radial artery
- abberant vessels
Answer from our lecture series:
- Accessory muscles: Gantzer’s accessory FPL muscle
- FDS
- Aberrant vessels
- Pronator teres
What are the common sites of compression of the Radial nerve (PIN compression syndrome)(5)?
Fibrous bands anterior to radial head
Recurrent radial vessels (Leash of Henry)
ECRB
Arcade of Frohse (proximal edge of supinator)
distal edge of supinator
What is the arcade of struthers?
What is the ligament of struthers?
Arcade of struthers:
Thickening of the deep investing fascia of the arm - Extends from the medial head of triceps to the intermusular septum Present in 70% of the population 1.5-2cm in width, 8-10cm proximal to the medial epicondyle.
where the ulnar n crosses lateral IM septum to go from anterior to posterior compartment - potential site of compression of ULNAR NERVE
Ligament of struthers:
This is a ligament from the supracondylar process (1% of pop) to the humerus and is a potential site of compression of the MEDIAN nerve
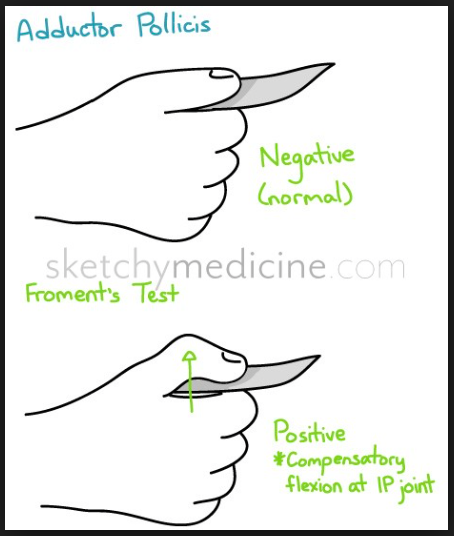
What is Froment’s sign? What does it indicate?
Seen with an ulnar nerve palsy with paralysis to the adductor pollicis.
There is compensatory flexion of the thumb IP joint when asked to grab a piece of paper.
***This is in contrast to an AIN palsy when the patient will be unable to grasp a piece of paper using a pincer grip due to loss of the long flexors***
Describe the pathogenesis of ulnar claw:
- MCP hyperextension: loss of intrinsics (responsible for MCP flexion)
- IP Flexion: Unopposed action of long extensors. Loss of lumbricals causes IP flexion
High vs low ulnar nerve lesion:
‘the closer to the Paw, the worse the Claw’.
This is because higher up you lose innervation to FDS to the ulnar two fingers which is a deforming force and functions to flex the IP joints. If you have a lower lesion then FDS is intact, causing more deformity and the “Worse the claw”
In a lower ulnar nerve lesion you get the Hand of benediction: - Hyperextension of MCPs & Flexion of IP joint - Due to loss of intrinsics and ulnar 2 lumbricals
Caused Low lesion of ulnar nerve causing above paralysis, exacerbated when asked to extend fingers.
Hand of benediction can also be seen with a median nerve lesion when asked to make a fist
What is the ulnar paradox?
High ulnar nerve lesion causes a paradoxically more benign looking hand (although the pathology is worse) - High ulnar nerve lesion takes out FDP also, causes less of an IP flexion contracture and a benign looking hand.
“The lower the claw, the worse the paw”
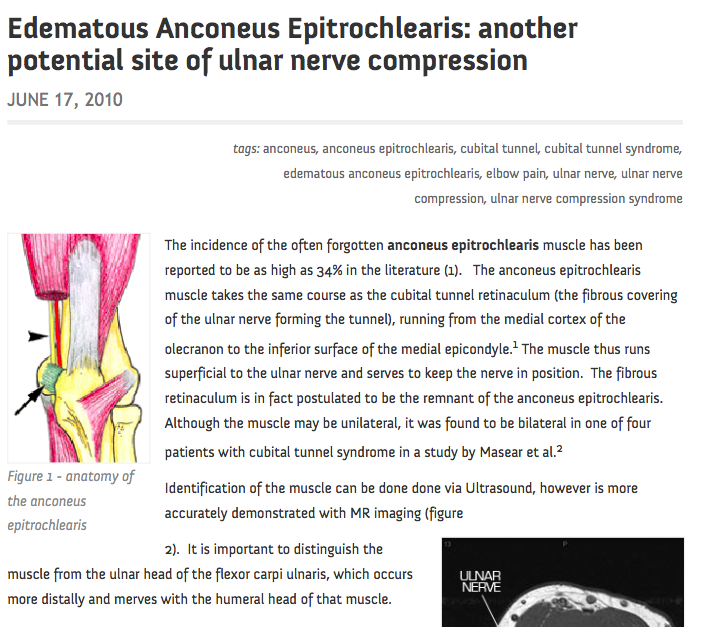
What is an anconeus epitrochlearis?
Anomalous muscle found in 10% of patients - Arises from medial border of olecranon & adjacent triceps - Inserts into medial epicondyle May be a muscular or fibrous structure
ANCONEUS proper is on the other side of the elbow. Dont get them confused
like a “muscular osborne’s ligament”
What is pronator syndrome?
Compression of median nerve at elbow
Main dDx: CTS
- Parasthesia in median nerve distribution Different from CTS b/c:
- Aching pain over proximal volar forearm
- Sensory disturbance over palmar cutaneous branch distribution (this arises 4-5cm proximal to carpal tunnel)
- Lack of night symptoms
What is AIN syndrome?
Compression of AIN
Weakness of FPL, FDP to middle and index fingers, and PQ
Cannot make OK sign
When do you see the “Hand of Benediction”
This refers to a median nerve palsy where you lose the ability to flex D1-3. This sign is brought out by asking the patient to make a fist. This looks very simliar to a claw hand but they are different as clawing is due to ulnar nerve lesion. A low ulnar nerve lesion is often also referred to as the hand of benediction. Worse with asking the patient to extend the fingers.
Where does the AIN originate?
4cm distal to medial Epicondyle, but generally quite variable where it branches off the median n proper, usually somewhere around the 2 heads of pronator
If you ask a patient to hold a piece of paper between their index and thumb and they do this, what is your diagnosis? what is this sign called?

AIN nerve palsy
Subtle weakness of the FPL and index finger FDP may be uncovered by asking the patient to pinch a sheet of paper between his thumb and index finger using only the fingertips and then trying to pull the paper away
This is NOT froment’s sign!
What are the boundaries of the the radial tunnel?
Cubital tunnel?
Carpal Tunnel?
Guyon’s canal?
Cubital tunnel:
Floor:
- Medial joint capsule
- MCL
- Olecranon
Roof:
- Osborne’s ligament
Carpal Tunnel
Floor:
- Carpal bones
Roof:
- Transverse Carpal ligament (flexor retinaculum)
Radial Border:
- Scaphoid tubercle
- Trapezium Ridge
Ulnar Border:
- Hook of Hamate
- Pisiform
Guyon’s Canal
Roof:
- volar carpal lig
Floor:
- Transverse Carpal ligament
Radial:
- hamate
Ulnar:
- pisiform
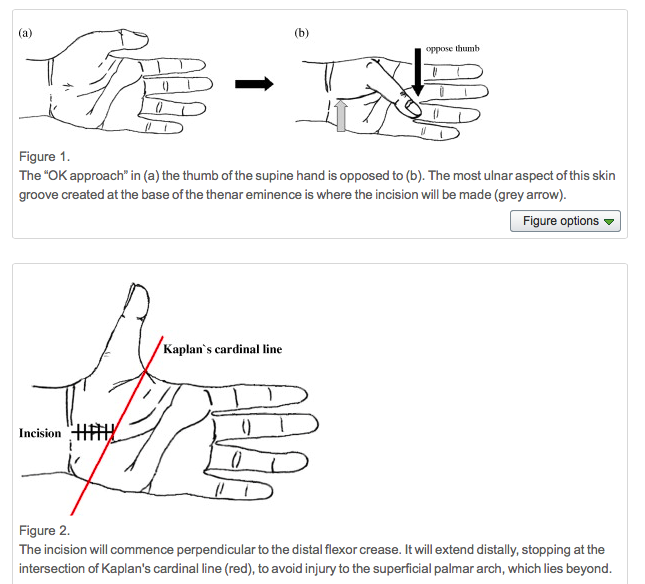
What is the flexor retinaculum in continuity with proximally?
What is a danger distally when releasing the carpal tunnel? How do you landmark this danger?
- In continuity with the antebrachial fascia.
- Danger at the distal edge is the superficial palmar arch.
- Dont go distal to Kaplans Cardinal line. (evidence that this is a better surface landmark for the superficial palmar arch than the deep palmar arch)
Hand. 2010 Jun; 5(2): 155–159.
The Clinical Application of Kaplan’s Cardinal Line as a Surface Marker for the Superficial Palmar Arch
What is the Martin Gruber Anastamosis?
What is it’s clinical significance?
Occurs in 10 to 44% of people
Branches from the median to ulnar nerve in the forearm. Can have 2 patterns:
- Median nn in the prox forearm to the ulnar nerve in the middle to distal third
- From AIN to ulnar nerve
- THE RESULT IS THAT THE MEDIAN NERVE ENDS UP INNERVATING HAND INTRINSICS
Clincial significance
- High ulnar n. laceration:
Preservation of intrinsic muscle function, along with loss of function of the FCU and FDP to the ulnar two fingers
- High median n. laceration:
Loss of some of the intrinsic muscles usually innervated by the ulnar n.
In the literature, some researchers cited the clinical importance of MGA. The intrinsic muscles of the hand were completely unaffected by median lesions. A lesion of the median nerve situated proximal to the departure of the communicating branch would affect the median thenar muscles, whereas a lesion below that would not
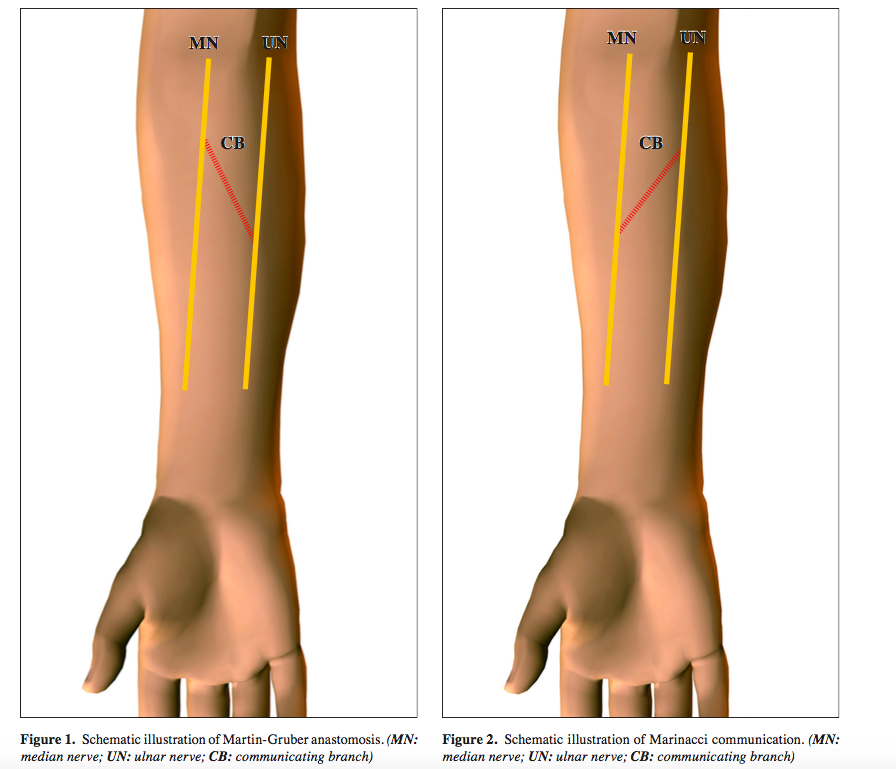
What is the Marinacci Anastamosis?
- A reverse Martin gruber from the ulnar to the median nerve.
- THE ULNAR NERVE ENDS UP INNERVATING THE THENAR MUSCLES
What is the Riche-Cannieu Anastamosis?
This is a communication between the deep branch of the ulnar nerve and the recurrent branch of the median nerve.
This can lead to a hand with complete ulnar intrinsic innervation. I.e the thenar eminence is ulnar based. This can be a problem with compression neuropathies at the wrist i.e guyon’s canal leading to weakness of the thenar eminence
Where does the AIN arise?
Where does it then run?
What does it innervate?
Usually arises 4cm distal to the medial epicondyle
Arises from the median nerve at a variable level as the nerve passess beween the heads of pronator teres. It then runs along the volar aspect of the IOM deep to FDP
Innervates FPL, lateral half of FDP and pronator quadratus (deep muscles)
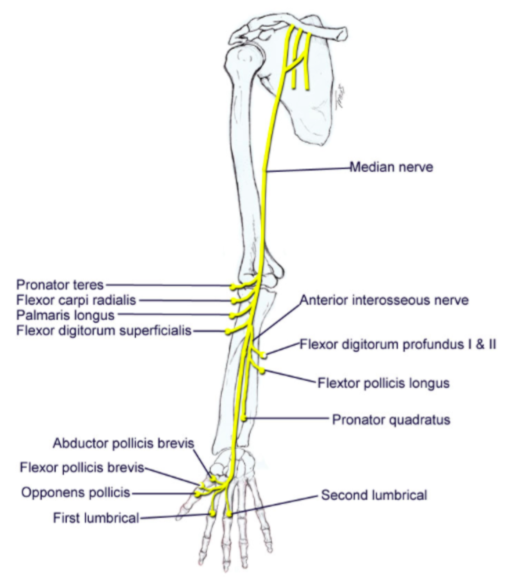
What does Median nerve innervate in the forearm and hand and what is the order of supply?
PT
FCR
PL
Then the AIN takes over and supplies FDP (1 and 2), FPL and PQ
In the hand the median nerve proper supplies:
APB, FPB, OP, Lumbricals 1 and 2
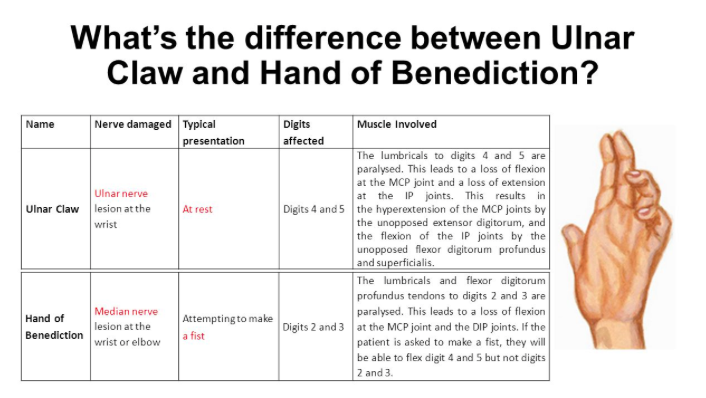
What is the difference between the Hand of Benediction and an Ulnar claw hand?
These two entities look very similar however
Benediction - median nerve. Only brought out if asked to make a fist. Unable to flex D1-3 due to loss of the long flexors. Only for high median nerve lesion before bifurcation to the AIN.
Claw hand - ulnar nerve. Spontaneous. MCP hyperextended, IP flexed all due to the overpull of the volar long flexors.
To explain why this occurs, we need to consider the muscles that are affected by an ulnar nerve lesion at the wrist:
Medial two lumbricals: Flexes at the MCP joints and extends at the IP joints of the little and ring fingers.
Interossei: Abducts and adducts the fingers.
Hypothenar muscles: Flexes, abducts, and opposes the little finger.
Adductor pollicis: Adducts the thumb.
Ulnar Claw
D4 and 5 are hyperextended at the metacarpophalangeal (MCP) joint, and flexed at both interphalangeal (IP) joints.
In the ulnar claw, the important muscles to consider are the medial lumbricals. If these muscles are paralysed, there is a loss of flexion at the MCP joints, and a loss of extension at the IP joints. This leads to an imbalance between the intrinsic and extrinsic muscles of the hand – producing the claw deformity:
The MCP joints are hyperextended due to unopposed extension from the long extensor muscles in the posterior compartment of the forearm.
The IP joints are flexed due to unopposed flexion from the long flexor muscles in the anterior compartment of the arm. The extensor muscles cannot extend at the IP joints as their energy is dissipated in hyperextending the MCP joints.
The ulnar claw only occurs in the little and ring fingers, as the lateral two lumbricals are innervated by the median nerve.
Hand of Benediction
The hand of benediction occurs as a result of median nerve damage at the elbow. In contrast to the ulnar claw, which is produced spontaneously, the hand of benediction is only apparent if the patient is asked to make a fist.
To explain how the hand of benediction is produced, we need to consider the muscles affected if the median nerve is lesioned at the elbow:
Long flexors in the anterior compartment of the arm (except the medial half of the flexor digitorum profundus and the flexor carpi ulnaris).
Lateral two lumbricals: Flexes at the MCP joints and extends at the IP joints of the index and middle fingers.
If the patient is asked to make a fist, they will be able to flex the little and ring fingers. This action is performed by the medial half of the flexor digitorum profundus and the medial two lumbricals.
The patient will not be able to flex the index and middle fingers. Thus, the patient displays a claw shape, where the little and ring fingers and flexed, the index and middle fingers extended.
What is ulnar paradox?
When there is a high ulnar nerve lesion and you get less clawing than with a more distal lesion. This is due to the loss of the FDP to D4-5.
“The closer to the paw, the more the claw”
Ulnar Paradox
The ulnar claw is a deformity produced by an ulnar nerve lesion at the wrist. We shall now look at what happens if the ulnar nerve is damaged more proximally – at the elbow.
In a high ulnar nerve injury, some muscles in the anterior forearm are paralysed (in addition to the hand muscles mentioned above):
Medial half of flexor digitorum profundus: Flexes at the distal IP joints of the ring and little fingers.
Flexor carpi ulnaris: Flexes and adducts the wrist.
The ulnar claw will develop as before, but with one key difference. The flexor digitorum profundus is paralysed, and there will not be any flexion at the distal IP joints of the ring and little fingers. Now the ulnar claw only consists of hyperextension at the MCP joints and flexion at the proximal IP joints. This produces a much less evident claw hand.
This is known as the ‘ulnar paradox‘ – you would expect a more debilitating injury to produce a more pronounced deformity, but in fact the opposite occurs.
What is radial tunnel syndrome?
lateral forearm pain, may also have weakness secondary to pain (not nerve weakness, i.e not a PIN palsy
Same sites as PIN compression syndrome (5)
- Leash of henry
- fibrous bands from anterior to the radiocapitellar joint
- medial edge ecrb
- Leading edge supinator (Arcade of frohse)
- distal edge supinator















