Patient with collapse, P wave rate of 75, Broad qrs rate of 40
Options:
complete AV block
first degree HB
second degree HB
Complete AV block (Complete heart block)
Features:
- syncope
- heart failure
- regular bradycardia (30-50 bpm)
- wide pulse pressure
- JVP: cannon waves in neck
- variable intensity of S1
Types of heart block
- First degree heart block
- PR interval > 0.2 seconds
- Second degree heart block
- type 1 (Mobitz I, Wenckebach): progressive prolongation of the PR interval until a dropped beat occurs
- type 2 (Mobitz II): PR interval is constant but the P wave is often not followed by a QRS complex
- Third degree (complete) heart block
- there is no association between the P waves and QRS complexes
Type 1 diabetic goes to an all night party, doesn’t eat and sleeps all day. 8pm presents to A&E with vomiting. pH 7.24
Options:
DKA
hypoglycaemia
DKA (Diabetic ketoacidosis)
may be a complication existing type 1 diabetes mellitus or be the first presentation, accounting for around 6% of cases. Whilst DKA remains a serious condition mortality rates have decreased from 8% to under 1% in the past 20 years.
The most common precipitating factors of DKA are infection, missed insulin doses and myocardial infarction
Features
- abdominal pain
- polyuria, polydipsia, dehydration
- Kussmaul respiration (deep hyperventilation)
- Acetone-smelling breath (‘pear drops’ smell)
Diagnostic criteria (joint british diabetes soc 2013)
- Glucose >11 mmol or known DM
- pH<7.3
- bicarcb <15
- Ketones >3 mmol/l or urine ketones ++ on dibpstick
Management
- fluid replacement: most patients with DKA are deplete around 5-8 litres. Isotonic saline is used initially. Please see an example fluid regime below.
- insulin: an intravenous infusion should be started at 0.1 unit/kg/hour. Once blood glucose is < 15 mmol/l an infusion of 5% dextrose should be started
- correction of hypokalaemia
Complications of DKA (and it’s treatment)
- gastric stasis
- Thromboembolism
- arrhythmia secondary to hyperkalaemia/isatrogenic hypokalaemia
- iatrogenic due to incorrect fluid therapy:
- cerebreal oedema, hypokalaemia, hypoglycaemia
- ARDS
- AKI

Student comes back to England from Nigeria with jaundice, anaemia and fever.
Options:
Falciparum
Hep A
Influenza A
Typhoid
Paratyphoid fever
Falicparum
Feature of severe malaria
- schizonts on a blood film
- parasitaemia > 2%
- hypoglycaemia
- acidosis
- temperature > 39 °C
- severe anaemia
- complications:
- cerebral malaria: seizures, coma
- acute renal failure: blackwater fever, secondary to intravascular haemolysis, mechanism unknown
- acute respiratory distress syndrome (ARDS)
- hypoglycaemia
- disseminated intravascular coagulation (DIC)
Uncomplicated falciparum malaria
- strains resistant to chloroquine are prevalent in certain areas of Asia and Africa
- the 2010 WHO guidelines recommend artemisinin-based combination therapies (ACTs) as first-line therapy
- examples include artemether plus lumefantrine, artesunate plus amodiaquine, artesunate plus mefloquine, artesunate plus sulfadoxine-pyrimethamine, dihydroartemisinin plus piperaquine
Severe falciparum malaria
- a parasite counts of more than 2% will usually need parenteral treatment irrespective of clinical state
- intravenous artesunate is now recommended by WHO in preference to intravenous quinine
- if parasite count > 10% then exchange transfusion should be considered
- shock may indicate coexistent bacterial septicaemia - malaria rarely causes haemodynamic collapse
40 year old farmer has wheeze for a few weeks. Normal CXR. Diagnosis.
Options:
Asthma
Farmers lung
Aspergillosis
Allergic bronchopulmonary Aspergillosis
results from an allergy to Aspergillus spores. In the exam questions often give a history of bronchiectasis and eosinophilia.
Features
- bronchoconstriction: wheeze, cough, dyspnoea
- bronchiectasis (proximal)
Investigations
- eosinophilia
- flitting CXR changes
- positive radioallergosorbent (RAST) test to Aspergillus
- positive IgG precipitins (not as positive as in aspergilloma)
- raised IgE
Management
- steroids
- itraconazole is sometimes introduced as a second line agent
Extrinsic allergic alverolitis e.g. farmers lung (spored of saccharopolyspora rectivirgula) is a hypersensitivity induce lung damage via a type III hypersensitivity immune complex mediated process. It presents acutely, c.4-8 hrs post exposure with SOB, dry cough, fever and may present chronically. Investigations: CXR (upper/mid zone fibrosis) bronchoalveolar lavage (lymphocytosis), blood (NO eosinophilia)
Anal abscess (described as perianal erythema and swelling) with fever and a lump. What do you do?
Options:
Give abx and review early
Incision and drainage
Oral flucloxacillin
Incision and drainage
Peri-anal abscess = perianal swelling & surrounding erythema
Treatment = I & D, leave the cavity open to heal by secondary intention
Management of benign proctology (see table and…):
- Haemorroidal disease
- The treatment of haemorroids is usually conservative. Acutely thrombosed haemorroids may be extremely painful. Treatment of this acute condition is usually conservative and consists of stool softeners, ice compressions and topical GTN or diltiazem to reduce sphincter spasm. Most cases managed with this approach will settle over the next 5-7 days. After this period there may be residual skin tags that merit surgical excision or indeed residual haemorroidal disease that may necessitate haemorroidectomy.
- Patients with more chronic symptoms are managed according to the stage of their disease, small mild internal haemorroids causing little symptoms are best managed conservatively. More marked symptoms of bleeding and occasional prolapse, where the haemorroidal complex is largely internal may benefit from stapled haemorroidopexy. This procedure excises rectal tissue above the dentate line and disrupts the haemorroidal blood supply. At the same time the excisional component of the procedure means that the haemorroids are less prone to prolapse. Adverse effects of this procedure include urgency, which can affect up to 40% of patients (but settles over 6-12 months) and recurrence. The procedure does not address skin tags and therefore this procedure is unsuitable if this is the dominant symptom.
- Large haemorroids with a substantial external component may be best managed with a Milligan Morgan style conventional haemorroidectomy. In this procedure three haemorroidal cushions are excised, together with their vascular pedicle. Excision of excessive volumes of tissue may result in anal stenosis. The procedure is quite painful and most surgeons prescribe metronidazole post operatively as it decreases post operative pain.
- Fissure in ano
- Probably the most efficient and definitive treatment for fissure in ano is lateral internal sphincterotomy. The treatment is permanent and nearly all patients will recover. Up to 30% will develop incontinence to flatus. There are justifiable concerns about using this procedure in females as pregnancy and pelvic floor damage together with a sphincterotomy may result in faecal incontinence. The usual first line therapy is relaxation of the internal sphincter with either GTN or diltiazem (the latter being better tolerated) applied topically for 6 weeks. Treatment failures with topical therapy will usually go on to have treatment with botulinum toxin. This leads to more permanent changes in the sphincter and this may facilitate healing.
- Typical fissures usually present in the posterior midline, multiple or unusually located fissures should prompt a search for an underlying cause such as inflammatory bowel disease or internal prolapse.
- Refractory cases where the above treatments have failed may be considered for advancement flaps.
- Fistula in ano
- The most effective treatment for fistula is laying it open (fistulotomy). When the fistula is below the sphincter and uncomplicated, this is a reasonable option. Sphincter involvement and complex underlying disease should be assessed both surgically and ideally with imaging (either MRI or endoanal USS). Surgery is then usually staged, in the first instance a draining seton suture may be inserted. This avoids the development of recurrent sepsis and may allow resolution. In patients with Crohns disease the seton should be left in situ long term and the patient managed medically, as in these cases attempts at complex surgical repair nearly always fail. Fistulas not associated with IBD may be managed by advancement flaps, instillation of plugs and glue is generally unsuccessful. A newer technique of ligation of intersphincteric tract (LIFT procedure) is reported to have good results in selected centres.

Pain on passive dorsiflexion Compartment syndrome young guy fractured tibia playing football.
Options:
4 compartment fasciotomy within 6h
Review in 12hrs
Send home
4 compartment fasciotomy within 6h
Compartment syndrome
This is a particular complication that may occur following fractures (or following ischaemia re-perfusion injury in vascular patients). It is characterised by raised pressure within a closed anatomical space.
The raised pressure within the compartment will eventually compromise tissue perfusion resulting in necrosis. The two main fractures carrying this complication include supracondylar fractures and tibial shaft injuries.
Symptoms and signs
- Pain, especially on movement (even passive)
- Parasthesiae
- Pallor may be present
- Arterial pulsation may still be felt as the necrosis occurs as a result of microvascular compromise
- Paralysis of the muscle group may occur
Diagnosis: Is made by measurement of intracompartmental pressure measurements. Pressures in excess of 20mmHg are abnormal and >40mmHg is diagnostic.
Treatment
- This is essentially prompt and extensive fasciotomies
- In the lower limb the deep muscles may be inadequately decompressed by the inexperienced operator when smaller incisions are performed
- Myoglobinuria may occur following fasciotomy and result in renal failure and for this reason these patients require aggressive IV fluids
- Where muscle groups are frankly necrotic at fasciotomy they should be debrided and amputation may have to be considered
- Death of muscle groups may occur within 4-6 hours
30something man with joint pain - sacroiliitis and distal interphalangeal joint pain?
Options:
Ankylosing spondylitis
Psoriatic arthritis
Rheumatoid arthritis.
Psoriatic arthropathy correlates poorly with cutaneous psoriasis and often precedes the development of skin lesions. Around 10-20% percent of patients with skin lesions develop an arthropathy with males and females being equally affected
Types*
- rheumatoid-like polyarthritis: (30-40%, most common type)
- asymmetrical oligoarthritis: typically affects hands and feet (20-30%)
- sacroilitis
- DIP joint disease (10%)
- arthritis mutilans (severe deformity fingers/hand, ‘telescoping fingers’)
Management:
treat as rheumatoid arthritis
but better prognosis
Transfusion reaction - fever, other obs normal, transfusion stopped. What next?
Options:
Check bag against patient details
Start transfusion again
Give chlorpheniramine
Check bag against patient details
Febrile non-haemolytic transfusion reaction
- Signs and symptoms: Fever, chills, headache, malaise, flushing
- Mechanism: host abs vs donor MHC antigens or due to cytokines from leukocytes in donor blood
- Treatment: discontinue transfusion, fever resolves in 15-30 mins without specific treatment. Paracetamol may be used
- Other: most common transusion reaction, can be prevented with leukocyte filters or irradiation
Haemolytic transfusion reaction
- Signs and symptoms: Fever, chills, pain at the infusion site, dark urine, nausea, shock
- Mechanism: ABO incompatibility with host abs vs antigens on donor RBCs
- Treatment: discontinue transfusion, administer fluids
- Other: most SEVERE reaction
Allergic transfusion reaction
- Signs and symptoms: Uritcaria, pruritus
- Mechanism: allergic reaction to plasma proteins in transfused blood
- Treatment: DOES NOT require discontinuing transfusion, symptomatic treatment with antihistamines
- Other: can be prevented with anti-histamine pre-treatment
Anaphylactic transfusion reaction
- Signs and symptoms: Uritcaria, angioedema, wheezing, laryngeal oedema, abdo pain, hypotension, shock
- Mechanism: Host abs vs IgA antibodies in the donor plasma
- Treatment: discontinue transfusion, administer adrenaline
- Other: Seen in pts with IgA deficiency, can be prevented by administering washed IgA decifient products
Transfusion relatied acute lung injury (TRALI)
- Signs and symptoms: dyspnoea, hypoxaemia, bilateral chest infiltrates
- Mechanism: donor Abs to MHC class I/II/Human neutrophil antigens. Activated neutrophils cause endothelial damage
- Treatment: discontinue transfusion, provide airway support
- Other: most common cause of transfusion related DEATH
Transfusion associated circulatory overload
- Signs and symptoms: dyspnoea, pulmonary oedema, HTN, peripheral oedema
- Mechanism: rapid volume expansion.
- Treatment: supportive, diuretics can be used
- Other: seen in elderly pts with HF/anaemia, can be prevented with slower transfusions and diuretics

Patient on warfarin having nasal polypectomy - what do you do to the warfarin.
Options:
Admit patient two days pre-op and start heparin
Change to aspirin after op to reduce risk of bleed
Measure aptt
Stop warfarin on the day of surgery
Admit patient two days pre-op and start heparin
the newer oral anticoagulants (dabigatran, rivaroxaban, apixaban) have shorter half-lives and faster onset of action compared to warfarin and bridging is generally not required
aPTT, intrinsic pathway (12), used to monitor hepatin
PT, extrinsic pathway (7), used to monitor warfarin
Warfarin: inhibits the reductase enzyme responsible for the active form of vitamin K therefore inhibits the synthesis of factors: 2, 7, 9, 10, C, S, Z
Nasal polypectomy is a procedue with a High Risk Bleeding (greater than 1.5% or in vulnerable areas).
Holding warfarin before surgery:
- For patients whose INR is between 2.0 and 3.0, discontinue warfarin 5 days prior to surgery (last dose given 6 days before surgery) and allow the INR to spontaneously fall. Warfarin should be withheld for a longer period of time if the INR is normally maintained above 3.0.
- The INR should be measured the day prior to surgery. Vitamin K may be administered if the INR is deemed excessive.
Bridging with IV unfractionated heparin before surgery:
- After discontinuation of warfarin, patients should be admitted to hospital and started on IV unfractionated heparin in therapeutic doses. Since therapeutic oral anticoagulation will remain therapeutic for at least a day after the last warfarin dose, patients can be admitted on the second day after their last dose of warfarin.
- IV heparin should be discontinued 4 to 6 hours prior to surgery.
Restarting warfarin after surgery
- Post-operatively, warfarin should be resumed when the patient is able to take medications by mouth and after the epidural catheter has been removed (if neuraxial analgesia has been used).
- Bridging with IV unfractionated heparin after surgery: Full dose (therapeutic dose) IV unfractionated heparin should be started no sooner than 24 hours after major surgery when there is adequate post-op hemostasis. If there is evidence of surgical bleeding or if the patient is at high risk of bleeding, it should be delayed further. It should also be delayed while the epidural catheter is insitu (if neuraxial analgesia has been used). In situations where therapeutic dose IV unfractionated heparin is deferred beyond 24 hours, the administration of prophylactic dose LMWH can be considered sooner (as early as the evening of the day of surgery). IV heparin may be started sooner if the surgery or procedure is of a minor nature and the risk of bleeding is low. Heparin should be continued until the INR is therapeutic.
Breast Ca - which is the biggest risk factor in this patient?
Options
Obesity
Smoking
Multiple pregnancies
Breastfeeding
Late menarche
Obesity
- Incidence: most common cancer in women, lifetime risk 1 in 8
- Age: 75-80yrs, (younger in Afro-Caribbean’s). Sex: 99% in women.
- Risk factors:
- Susceptibility genes (12%) – BRCA1/BRCA2, also increased risk of ovarian, prostate and pancreatic malignancy. BRCA mutations cause a lifetime risk of invasive breast carcinoma of up to 85%.
- Hormone exposure
- Early menarche
- Late menopause
- Late 1st live birth (pregnancy → terminal differentiation of milk-producing luminal cells, removing these from pool of potential cancer precursors)
- OCP/HRT
- Advancing age
- Family history
- Race (Caucasian>Afro-Caribbean>Asian>Hispanic)
- Obesity, tobacco, alcohol
- Presentation: hard fixed lump, Paget’s disease, peau d’orange, nipple retraction.
- Screening: 47 to 73yr old women invited every 3 years for mammography (looks for abnormal areas of calcification or a mass within the breast)
Legionella - which Abx?
Options:
Ciprofloxacin
Clarithromycin
Cefotaxime
Cefalexin
Clarithromycin
Legionella
Legionnaire’s disease is caused by the intracellular bacterium Legionella pneumophilia. It is typically colonizes water tanks and hence questions may hint at air-conditioning systems or foreign holidays. Person-to-person transmission is not seen
Features
- flu-like symptoms including fever (present in > 95% of patients)
- dry cough
- relative bradycardia
- confusion
- lymphopaenia
- hyponatraemia
- deranged liver function tests
- pleural effusion: seen in around 30% of patients
Diagnosis: urinary antigen
Management: treat with erythromycin

Which drug is commonly co-prescribed with morphine?
Options:
Aspirin
Hyoscine
Co-danthramer
Loperamide
Co-danthramer
Co-danthramer: Constipation is a common cause of distress and is almost invariable after administration of an opioid analgesic. It should be prevented if possible by the regular administration of laxatives; a faecal softener with a peristaltic stimulant (e.g. co-danthramer) or lactulose solution with a senna preparation should be used. Methylnaltrexone bromide is licensed for the treatment of opioid-induced constipation.
Hyoscine: Bowel colic and excessive respiratory secretions may be reduced by a subcutaneous injection of hyoscine hydrobromide, hyoscine butylbromide, or glycopyrronium bromide. These antimuscarinics are generally given every 4 hours when required, but hourly use is occasionally necessary, particularly in excessive respiratory secretions. If symptoms persist, they can be given regularly via a continuous infusion device. Care is required to avoid the discomfort of dry mouth.
Loperamide: The pain of bowel colic may be reduced by loperamide hydrochloride. Hyoscine hydrobromide may also be helpful, given sublingually as Kwells ® tablets. Subcutaneous injections of hyoscine butylbromide, hyoscine hydrobromide, and glycopyrronium bromide can also be used to treat bowel colic.
Gastric distension pain due to pressure on the stomach may be helped by a preparation incorporating an antacid with an antiflatulent and a prokinetic such as domperidone before meals.
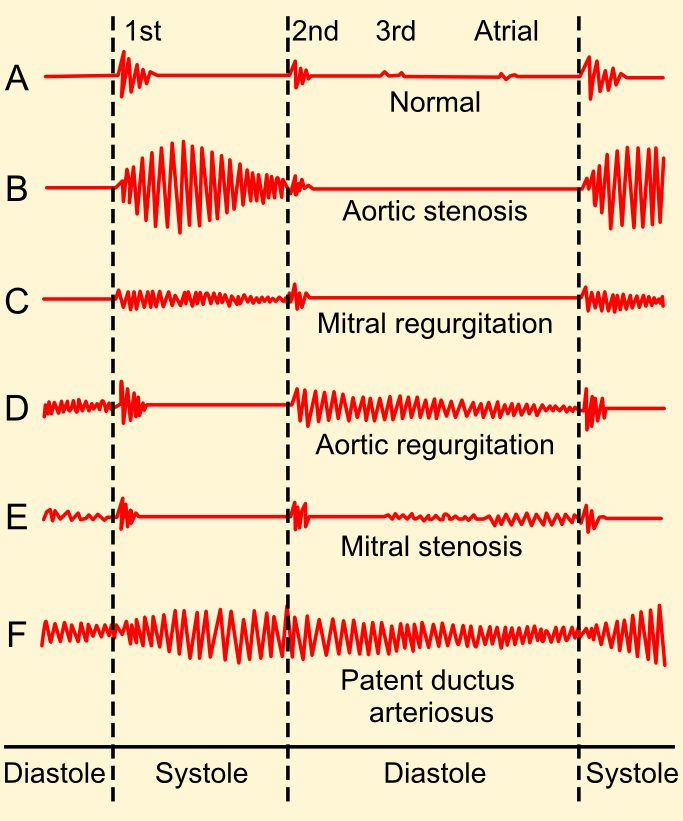
Mid-diastolic murmur
Mitral stenosis
Ejection systolic
- aortic stenosis
- pulmonary stenosis, HOCM
- ASD, Fallot’s
Holosystolic (pansystolic)
- mitral/tricuspid regurgitation (high-pitched and ‘blowing’ in character)
- VSD (‘harsh’ in character)
Late systolic
- mitral valve prolapse
- coarctation of aorta
Early diastolic
- aortic regurgitation (high-pitched and ‘blowing’ in character)
- Graham-Steel murmur (pulmonary regurgitation, again high-pitched and ‘blowing’ in character)
Mid-late diastolic
- mitral stenosis (‘rumbling’ in character)
- Austin-Flint murmur (severe aortic regurgitation, again is ‘rumbling’ in character)
Continuous machine-like mumur
- patent ductus arteriosus
Pericarditis murmur qs - Patient has widespread ST elevation, which sound heard on ausc?
Scratch (pericardial friction rub)
Pericarditis is one of the differentials of any patient presenting with chest pain.
Features
- chest pain: may be pleuritic. Is often relieved by sitting forwards
- other symptoms include non-productive cough, dyspnoea and flu-like symptoms
- pericardial rub
- tachypnoea
- tachycardia
Causes
- viral infections (Coxsackie)
- tuberculosis
- uraemia (causes ‘fibrinous’ pericarditis)
- trauma
- post-myocardial infarction, Dressler’s syndrome
- connective tissue disease
- hypothyroidism
ECG changes
- widespread ‘saddle-shaped’ ST elevation
- PR depression: most specific ECG marker for pericarditis
Management: if acuse, analgesia ibuprofen PI and Rx cause, consider steroids and immunosuppresion
Which antibodies are most specific/raised in SLE
Options:
dsDNA
anti-cardiolipin
anti-Smith
Anti-U1 RNP
Anti-Smith
Immunology
- 99% are ANA positive (sensitive)
- 20% are rheumatoid factor positive
- anti-dsDNA: highly specific (> 99%), but less sensitive (70%)
- anti-Smith: most specific (> 99%), sensitivity (30%)
- also: anti-U1 RNP, SS-A (anti-Ro) and SS-B (anti-La)
Monitoring
- ESR: during active disease the CRP is characteristically normal - a raised CRP may indicate underlying infection
- complement levels (C3, C4) are low during active disease (formation of complexes leads to consumption of complement)
- anti-dsDNA titres can be used for disease monitoring (but note not present in all patients)
EDM Aortic regurg murmur with sudden onset chest pain going to back.
Diagnosis?
Aortic dissection
Aortic dissection is a rare but serious cause of chest pain.
Associations
- hypertension
- trauma
- bicuspid aortic valve
- collagens: Marfan’s syndrome, Ehlers-Danlos syndrome
- Turner’s and Noonan’s syndrome
- pregnancy
- syphilis
Features:
- chest pain: typically severe, radiates through to the back and ‘tearing’ in nature
- aortic regurgitation
- hypertension
- other features may result from the involvement of specific arteries. For example:
- coronary arteries → angina
- spinal arteries → paraplegia
- distal aorta → limb ischaemia
Classification
- Stanford classification
- type A - ascending aorta, 2/3 of cases
- type B - descending aorta, distal to left subclavian origin, 1/3 of cases
- DeBakey classification
- type I - originates in ascending aorta, propagates to at least the aortic arch and possibly beyond it distally
- type II - originates in and is confined to the ascending aorta
- type III - originates in descending aorta, rarely extends proximally but will extend distally
Management
- Type A: surgical management, but blood pressure should be controlled to a target systolic of 100-120 mmHg whilst awaiting intervention
- Type B*: conservative management = bed rest + reduce blood pressure IV labetalol to prevent progression
Complications
- Complications of backward tear
- aortic incompetence/regurgitation
- MI: inferior pattern often seen due to right coronary involvement
- Complications of forward tear
- unequal arm pulses and BP
- stroke
- renal failure
Patient with symptoms of aortic dissection - AR etc, what test for confirming diagnosis?
Otions:
Contrast CT chest
CXR
USS
Contrast CT chest
Because of the varying symptoms and signs of aortic dissection depending on the initial intimal tear and the extent of the dissection, the proper diagnosis is sometimes difficult to make.
While taking a good history from the individual may be strongly suggestive of an aortic dissection, the diagnosis cannot always be made by history and physical signs alone. Often, the diagnosis is made by visualization of the intimal flap on a diagnostic imaging test. Common tests used to diagnose an aortic dissection include a CT scan of the chest with iodinated contrast material and a transesophageal echocardiogram.
Investigations:
- Bloods: FBC, cross-match 10 units of blood, U&E (renal function), clotting.
- CXR: Widened mediastinum, localized bulge in the aortic arch.
- ECG: Often normal. Signs of left ventricular hypertrophy or inferior MI if dissection compromises the ostia of the right coronary artery.
- CT-thorax: False lumen of dissection can be visualized.
- Echocardiography: Transoesophageal is highly specific.
- Cardiac catheterization and aortography.
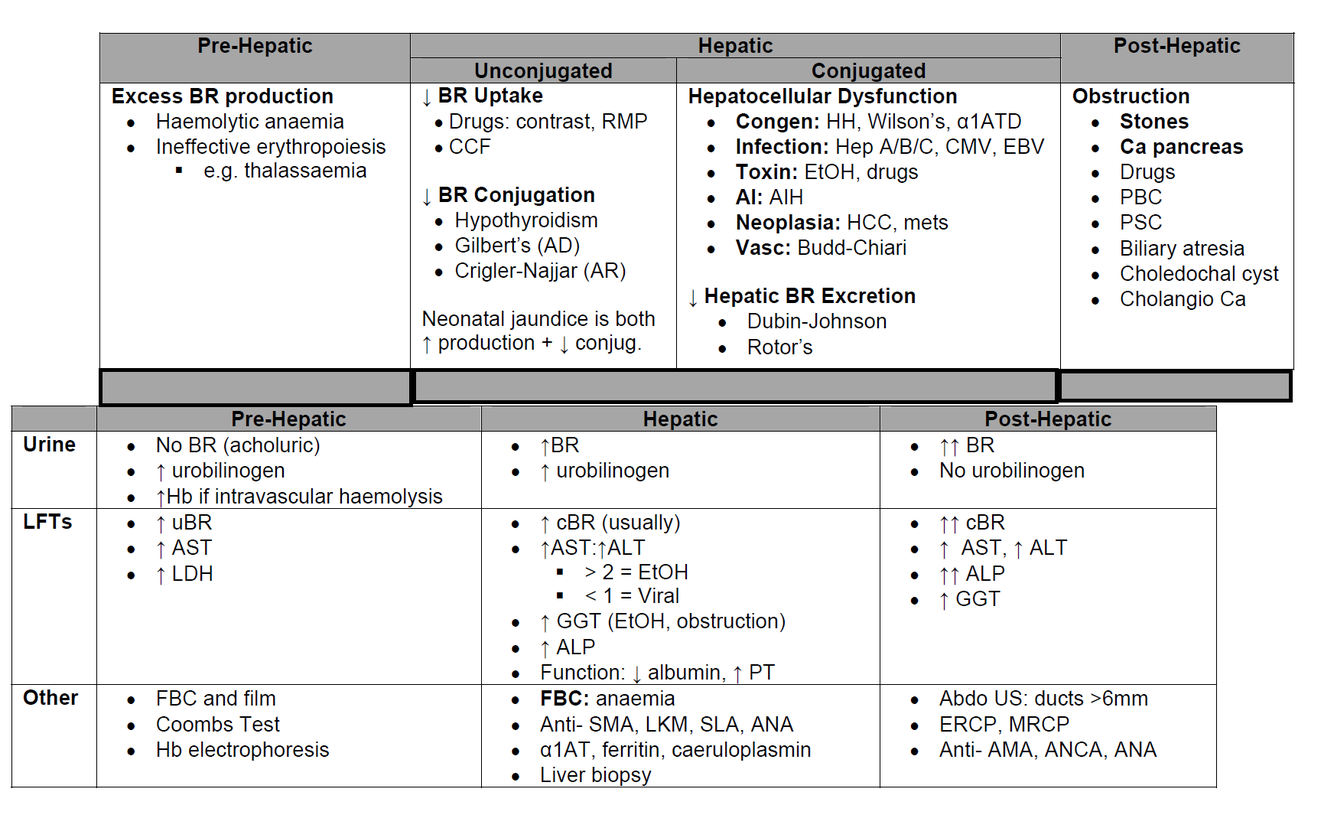
Lady with yellow eyes and high reticulocytes.
Options:
Alcoholic hepatitis
Haemolysis
Viral Hepatitis
Haemolysis
70yo lady falls in road onto outstretched hand and gets fracture. What test should GP follow up with?
Options
Vit d levels
DEXA
Bone profile
DEXA
Indications for a DEXA scan:
- a patient with a history of a low trauma fracture e.g. spine, hip, distal forearm
- an incidental X-ray finding of osteopenia or vertebral collapse or in the investigation of thoracic kyphosis or loss of height
- if there is maternal history of hip fracture
- if the patient has a low body mass index (BMI < 19 kg/m^2)
- if the patient has received corticosteroid treatment (prednisolone 7.5 mg or more) for greater than three months
- oestrogen deficiency:
- in a patient with premature menopause (< 45 years of age)
- primary hypogonadism
- secondary amenorrhoea (which lasts more than six months) e.g. secondary to GnRH anologues
- where there are conditions that predispose to secondary osteoporosis including:
- malabsorption syndromes e.g. coeliac disease, inflammatory bowel disease
- long-term treatment with anticonvulsants
- organ transplantation
- eating disorders
- chronic renal failure
- thyrotoxicosis
- primary hyperparathyroidism
- Cushing’s syndrome
- male hypogonadism
- prolonged immobilisation
Patient on warfarin for AF has INR of 3.3, falls and found on CT to have intracerebral haematoma - warfarin stopped and been given Vit K, what next?
Options
Prothrombin complex
Vit K again in 12 hours
Mannitol
Prothrombin Complex
For Major bleeding, including intracranial haemorrhage: Stop warfarin. Give prothrombin complex concentrate. If unavailable, give FFP. Also give vitamin K IV.
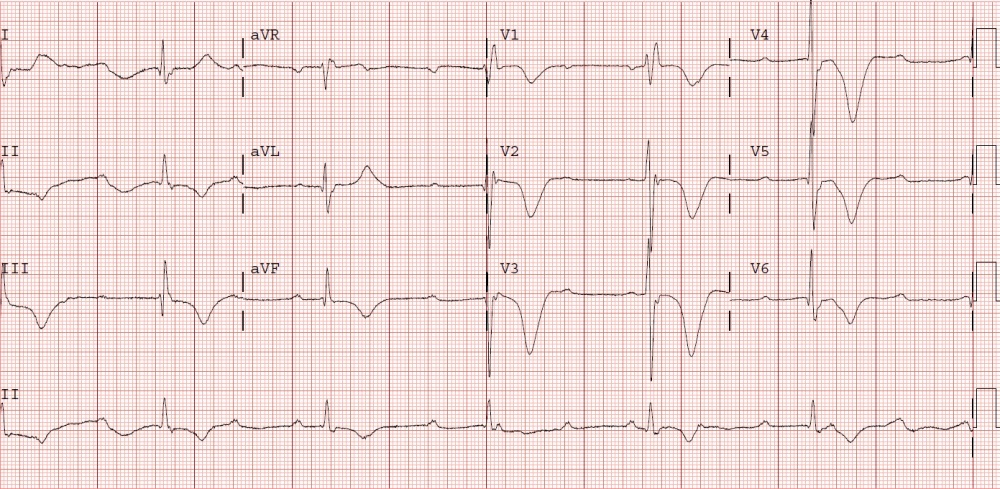
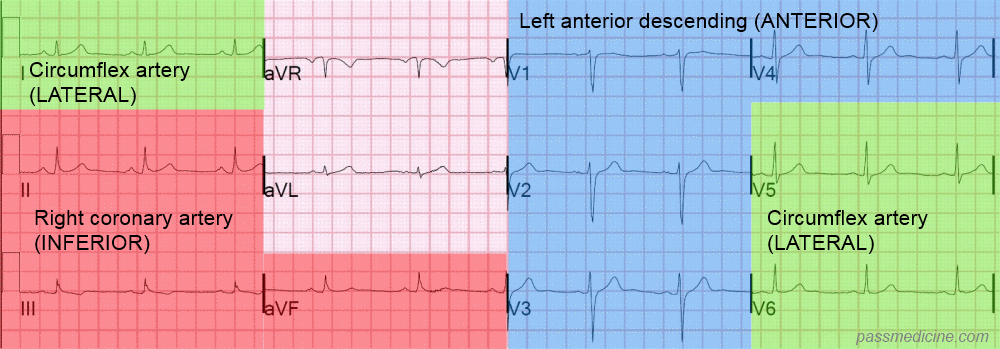
Patient has central chest pain, which ECG criteria would be indication for thrombolysis?
Options:
New RBBB
ST elevation in leads II, III and aVF
T wave inversion in aVR
ST depression in lead v1-4
ST elevation in leads II, III and aVF
- New RBBB: could be PE with RV dysfunction
- ST elevation in leads II, III and aVF: inferior STEMI
- T wave inversion in aVR: normal in aVR and V1
- ST depression in lead v1-4: ischaemia/NSTEMI (if raise troponin)
With regards to thrombolysis:
Primary percutaneous coronary intervention (PCI) has emerged as the gold-standard treatment for STEMI but is not available in all centres. Thrombolysis should be performed in patients without access to primary PCI
- Tissue plasminogen activator (tPA) has been shown to offer clear mortality benefits over streptokinase
- Tenecteplase is easier to administer and has been shown to have non-inferior efficacy to alteplase with a similar adverse effect profile
- An ECG should be performed 90 minutes following thrombolysis to assess whether there has been a greater than 50% resolution in the ST elevation
- if there has not been adequate resolution then rescue PCI is superior to repeat thrombolysis
- for patients successfully treated with thrombolysis PCI has been shown to be beneficial. The optimal timing of this is still under investigation
RBBB:
- Right ventricular hypertrophy / cor pulmonale
- Pulmonary embolus
- Ischaemic heart disease
- Rheumatic heart disease
- Myocarditis or cardiomyopathy
- Degenerative disease of the conduction system
- Congenital heart disease (e.g. atrial septal defect)
Male married 30 years, sex with only his wife, pain in testicle and epididymis. Organism?
Options
Chlamydia trachomatis
E.Coli
Neisseria gonorrhoea
E.coli
- Elderly, and unable to distinguish between two sti*
- bacterial infections are the most common aetiology for epididymitis*
- in men <= 35 years of age, ascending infection from the urethra by sexually transmittable pathogens, namely Chlamydia trachomatis and Neisseria gonorrhoeae, are aetiologically responsible
- in older men with a history of bladder outlet disturbances
- Enterobacteriaceae, particularly Escherichia coli, represent the dominant pathogens
- tuberculous epididymitis caused by mycobacteria must be considered as a differential diagnosis
Epididymo-orchitis describes an infection of the epididymis +/- testes resulting in pain and swelling. It is most commonly caused by local spread of infections from the genital tract (such as Chlamydia trachomatis and Neisseria gonorrhoeae) or the bladder.
The most important differential diagnosis is testicular torsion. This needs to be excluded urgently to prevent ischaemia of the testicle.
Features
- unilateral testicular pain and swelling
- urethral discharge may be present, but urethritis is often asymptomatic
- factors suggesting testicular torsion include patients < 20 years, severe pain and an acute onset
Management
- the British Association for Sexual Health and HIV (BASHH) produced guidelines in 2010
- if the organism is unknown BASHH recommend: ceftriaxone 500mg intramuscularly single dose, plus doxycycline 100mg by mouth twice daily for 10-14 days
- further investigations following treatment are recommended to exclude any underlying structural abnormalities
Chlamydia
is the most prevalent sexually transmitted infection in the UK and is caused by Chlamydia trachomatis, an obligate intracellular pathogen. Approximately 1 in 10 young women in the UK have Chlamydia. The incubation period is around 7-21 days, although it should be remembered a large percentage of cases are asymptomatic
Features
- asymptomatic in around 70% of women and 50% of men
- women: cervicitis (discharge, bleeding), dysuria
- men: urethral discharge, dysuria
Potential complications
- epididymitis
- pelvic inflammatory disease
- endometritis
- increased incidence of ectopic pregnancies
- infertility
- reactive arthritis
- perihepatitis (Fitz-Hugh-Curtis syndrome)
Investigation
- traditional cell culture is no longer widely used
- nuclear acid amplification tests (NAATs) are now rapidly emerging as the investigation of choice
- urine (first void urine sample), vulvovaginal swab or cervical swab may be tested using the NAAT technique
Screening
- in England the National Chlamydia Screening Programme is open to all men and women aged 15-24 years
- the 2009 SIGN guidelines support this approach, suggesting screening all sexually active patients aged 15-24 years
- relies heavily on opportunistic testing
45 year old with intracapsular #NOF otherwise well (not given Garden classification) - management?
Options
Hemiarthroplasty
Dynamic hip screw
Cannulated screws
Cannulated screws
Garden 1 and 2
Cannulated screw
Garden 3 and 4
Ain’t hemi anymore
Between greater lesser
DHS is better
If below the neck should fail
Inter medullary nail
NOT DHS- ‘If you can get adequate fixation with the least amount of metal then it’s ideal, specifically in a patient in which you want to maximise bone salvage and minimise instrumentation’
NOF The hip is a common site of fracture especially in osteoporotic, elderly females. The blood supply to the femoral head runs up the neck and thus avascular necrosis is a risk in displaced fractures.
Features:
- pain
- shortened and externally rotated leg
The Garden system:
- Type I: Stable fracture with impaction in valgus.
- Type II: Complete fracture but undisplaced.
- Type III: Displaced fracture, usually rotated and angulated, but still has bony contact.
- Type IV: Complete bony disruption.

Patient has cough, apical cavitating lesions, haemoptysis, firm LN in neck. What test?
Options:
Auramine stain of sputum
Sputum culture and sensitivity for AAFB
LN biopsy
Auramine stain of sputum -> next step in management
Sputum culture and sensitivity for AAFB -> Confirm diagnosis and treatment specifically
Ziehl-Nielsen or auramine staining of a sputum smear may demonstrate the presence of acid-fast bacilli in vitro culture of the sputum may take 4 to 7 weeks to provide a result; a further 3 weeks is required to identify drug sensitivity
Diagnosis Latent TB: Do a Mantoux test. If +ve (or non-reliable) consider interferongamma testing
Active TB: If CXR suggests TB, take sputum samples (≥3, with one early morning
sample, before starting treatment if possible) and send for MC&S for AFB (acid-fast
bacilli resist acid on Ziehl–Neelsen (ZN) staining). If spontaneously produced sputum cannot be obtained, bronchoscopy and lavage may be needed.
Active non-respiratory TB: Try hard to get samples: sputum, pleura & pleural fl uid,
urine, pus, ascites, peritoneum, bone marrow or CSF. Send surgical samples for
culture. Microbiologist should routinely do TB culture on these, even if it is not requested. All patients with non-respiratory TB should have a CXR to find coexisting respiratory TB. Incubate cultures for up to 12wks on Lowenstein–Jensen medium.
PCR: Allows rapid identifi cation of rifampicin (and likely multidrug) resistance.
Histology: The hallmark is the presence of caseating granulomata.
CXR signs: Consolidation, cavitation, fi brosis, and calcifi cation.
Immunological evidence of TB may be helpful:
- Tuberculin skin test: TB antigen is
- injected intradermally and the cell-mediated response at 48–72h is recorded. A +ve test indicates immunity. It may also indicate previous exposure or BCG. A strong+ve test probably means active TB. False –ve tests occur in immuno suppression (miliary TB, sarcoid, AIDS, lymphoma).
- Quantiferon TB Gold® and T-spot-TB® tests measure the delayed hypersens itivity reaction developed after contact with M. tuberculosis;they use specifi c, complex M. tuberculosis antigens and are better than older Mantoux tests, which rely on reactions to serial dilutions of TB antigen.












