Lady with falciparum. Other than doxycycline, what other abx would you give her?
Options:
Chloroquine
Quinine
Proguanil
Pyrimethamine
Quinine
Non-artemisinin based combinations: Quinine plus tetracycline/doxycycline
Feature of severe malaria
- schizonts on a blood film
- parasitaemia > 2%
- hypoglycaemia
- acidosis
- temperature > 39 °C
- severe anaemia
- complications:
- cerebral malaria: seizures, coma
- acute renal failure: blackwater fever, secondary to intravascular haemolysis, mechanism unknown
- acute respiratory distress syndrome (ARDS)
- hypoglycaemia
- disseminated intravascular coagulation (DIC)
Uncomplicated falciparum malaria
- strains resistant to chloroquine are prevalent in certain areas of Asia and Africa
- the 2010 WHO guidelines recommend artemisinin-based combination therapies (ACTs) as first-line therapy
- examples include artemether plus lumefantrine, artesunate plus amodiaquine, artesunate plus mefloquine, artesunate plus sulfadoxine-pyrimethamine, dihydroartemisinin plus piperaquine
Severe falciparum malaria
- a parasite counts of more than 2% will usually need parenteral treatment irrespective of clinical state
- intravenous artesunate is now recommended by WHO in preference to intravenous quinine
- if parasite count > 10% then exchange transfusion should be considered
- shock may indicate coexistent bacterial septicaemia - malaria rarely causes haemodynamic collapse
Which of the DMARDs cause retinopathy?
Options:
Hydroxychloroquine
Prednisolone
Sulfasalazine
Leflunomide
Hydroxychloroquine
Rheumatoid arthritis drug side effects
- Hydroxychloroquine
- Retinopathy
- Corneal deposits
- Methotrexate
- Myelosuppression
- Liver cirrhosis
- Pneumonitis
- Sulfasalazine
- Rashes
- Oligospermia
- Heinz body anaemia
- Interstitial lung disease
- Leflunomide
- Liver impairment
- Interstitial lung disease
- Hypertension
- Prednisolone
- Cushingoid features
- Osteoporosis
- Impaired glucose tolerance
- Hypertension
- Cataracts
- Gold
- Proteinuria
- Penicillamine
- Proteinuria
- Exacerbation of myasthenia gravis
- Etanercept
- Demyelination
- Reactivation of tuberculosis
- Infliximab
- Reactivation of tuberculosis
- Adalimumab
- Reactivation of tuberculosis
- Rituximab
- Infusion reactions are common
- NSAIDs (e.g. naproxen, ibuprofen)
- Bronchospasm in asthmatics
- Dyspepsia/peptic ulceration
Which of the DMARDs cause azoospermia and bone marrow suppression?
Options:
Sulfasalazine
Azathioprine
Methotrexate
Leflunomide
Sulfasalazine
- Hydroxychloroquine
- Retinopathy
- Corneal deposits
- Methotrexate
- Myelosuppression
- Liver cirrhosis
- Pneumonitis
- Sulfasalazine
- Rashes
- Oligospermia
- Heinz body anaemia
- Interstitial lung disease
- Leflunomide
- Liver impairment
- Interstitial lung disease
- Hypertension
- Prednisolone
- Cushingoid features
- Osteoporosis
- Impaired glucose tolerance
- Hypertension
- Cataracts
- Gold
- Proteinuria
- Penicillamine
- Proteinuria
- Exacerbation of myasthenia gravis
- Etanercept
- Demyelination
- Reactivation of tuberculosis
- Infliximab
- Reactivation of tuberculosis
- Adalimumab
- Reactivation of tuberculosis
- Rituximab
- Infusion reactions are common
- NSAIDs (e.g. naproxen, ibuprofen)
- Bronchospasm in asthmatics
- Dyspepsia/peptic ulceration
Lady with tremor, weight loss, proptosis and exophthalmos. Has ophthalmoplegia. What is likely cause?
Options:
Rectus muscle thickening
Retrobulbar tumour
Cavernous sinus syndrome
Rectus muscle thickening
as seen in thyroid eye disease
Pathophysiology: it is thought to be caused by an autoimmune response against an autoantigen, possibly the TSH receptor → retro-orbital inflammation –> glycosaminoglycan and collagen deposition in the muscles
(frequently: inferior rectus > medial rectus > superior rectus) sparing their tendinous insertions, and is usually bilateral and symmetrical.
Features
- the patient may be eu-, hypo- or hyperthyroid at the time of presentation
- exophthalmos
- conjunctival oedema
- optic disc swelling
- ophthalmoplegia
- inability to close the eye lids may lead to sore, dry eyes. If severe and untreated patients can be at risk of exposure keratopathy
Prevention
- smoking is the most important modifiable risk factor for the development of thyroid eye disease
- radioiodine treatment may increase the inflammatory symptoms seen in thyroid eye disease. In a recent study of patients with Graves’ disease around 15% developed, or had worsening of, eye disease. Prednisolone may help reduce the risk
Management
- topical lubricants may be needed to help prevent corneal inflammation caused by exposure
- steroids
- radiotherapy
- surgery
69 year old guy with two previous TIAs and AF. What do you start him on?
Option:
Warfarin
Aspirin
Clopidogrel
Aspirin + Modified release dipyridamol
Warfarin or NOAC (Dabigatran, Rivaroxaban, Apixaban)
nb Direct oral anticoagulants (direct thrombin/Xa inhibitors) are used in the prevention of stroke secondary to non-valvular AF
Post ischaemic stroke prophylaxis:
- clopidogrel is now recommended by NICE ahead of combination use of aspirin plus modified release (MR) dipyridamole in people who have had an ischaemic stroke
- aspirin plus MR dipyridamole is now recommended after an ischaemic stroke only if clopidogrel is contraindicated or not tolerated, but treatment is no longer limited to 2 years’ duration
- MR dipyridamole alone is recommended after an ischaemic stroke only if aspirin or clopidogrel are contraindicated or not tolerated, again with no limit on duration of treatment
- Stoke secondary to AF:
- following a stroke or TIA warfarin or a DOAC should be given as the anticoagulant of choice.
- If valvular AF, Warfarin must be used
- Aspirin/dipyridamole should only be given if needed for the treatment of other comorbidities
- in acute stroke patients, in the absence of haemorrhage, anticoagulation therapy should be commenced after 2 weeks. If imaging shows a very large cerebral infarction then the initiation of anticoagulation should be delayed
- following a stroke or TIA warfarin or a DOAC should be given as the anticoagulant of choice.

Lady with hx of AF presents to A&E with fast AF, pulmonary oedema and peripheral oedema. What do you give initially?
Options:
Furosemide and warfarin
Furosemide and Ramipril
DC cardioversion (if an option)
Cardioversion indicated in Peri-arrest rhythms: tachycardia
- shock: hypotension (systolic blood pressure < 90 mmHg), pallor, sweating, cold, clammy extremities, confusion or impaired consciousness
- syncope
- myocardial ischaemia
- heart failure
Furosemide and ?warfarin
- nb.acute pulmonary edema may increase sensitivity to ACE inhibition or angiotensin blockade, including risks of hypotension and renal dysfunction*
- warfarin will initiall decrease the INR (increase risk of clotti**ng) – it is often recommended that heparin should be administered in the ED if a AF patient is going to be admitted to hospital for expedited elective cardioversion (AF duration < 48 hours, or AF duration > 48 hours with a negative TEE study)*
Management options in acute heart failure include:
- oxygen
- diuretics
- opiates
- vasodilators
- inotropic agents
- CPAP
- ultrafiltration
- mechanical circulatory assistance: e.g. intra-aortic balloon counterpulsation or ventricular assist devices
Drug management of heart failure:
- first-line= ACE-inhibitor + beta-blocker
- second-line= aldosterone antagonist, angiotensin II receptor blocker or a hydralazine in combination with a nitrate
- third line= cardiac resynchronisation therapy or digoxin* or ivabradine (in pt on ACE-inhibitor, beta-blocker + aldosterone antagonist, with HR > 75/min and a left ventricular fraction < 35%)
- diuretics should be given for fluid overload
- offer annual influenza vaccine
- offer one-off** pneumococcal vaccine
30 something man with joint pain - sacroilitis and distal interphalangeal joint pain?
Options:
Ank spond
Psoriatic arthritis
Rheumatoid arthritis.
Psoriatic arthropathy
correlates poorly with cutaneous psoriasis and often precedes the development of skin lesions. Around 10-20% percent of patients with skin lesions develop an arthropathy with males and females being equally affected
Types*
- rheumatoid-like polyarthritis: (30-40%, most common type)
- asymmetrical oligoarthritis: typically affects hands and feet (20-30%)
- sacroilitis
- DIP joint disease (10%)
- arthritis mutilans (severe deformity fingers/hand, ‘telescoping fingers’)
Management
- treat as rheumatoid arthritis
- but better prognosis
nb ankylosing spondylitis: affects axial spine
Guy on prednisolone presents with darkened red reflex and problems with night vision. What does he have?
Cataracts
opacities in lens, cornea or vitreous results in loss of red reflex
Presentation
- Increasing myopia
- Blurred vision → gradual visual loss
- Dazzling in sunshine / bright lights
- Monocular diplopia
Cause
Majority
- age related
- UV light
Systemic
- diabetes mellitus
- steroids
- infection (congenital rubella)
- metabolic (hypocalcaemia, galactosaemia)
- myotonic dystrophy
- Down’s syndrome
Ocular
- trauma
- uveitis
- high myopia
- topical steroids
Classification
- Nuclear: change lens refractive index, common in old age
- Polar: localized, commonly inherited, lie in the visual axis
- Subcapsular: due to steroid use, just deep to the lens capsule, in the visual axis
- Dot opacities: common in normal lenses, also seen in diabetes and myotonic dystrophy

Lady from some Pakistan or somewhere with HTN controlled on amlodipine and BP of 150/90 has retinal findings: blot haemorrhages and yellow deposits (hard exudates I think) on macula. What is this?
Options:
Hypertensive retinopathy
Diabetic retinopathy
NOTE: Drusen seen in age related macular degeneration
Background diabetic retinopathy
- microaneurysms (dots)
- blot haemorrhages (<=3)
- hard exudates
Pre-proliferative retinopathy
- cotton wool spots (soft exudates; ischaemic nerve fibres)
- > 3 blot haemorrhages
- venous beading/looping
- deep/dark cluster haemorrhages
- more common in Type I DM, treat with laser photocoagulation
Proliferative retinopathy
- retinal neovascularisation - may lead to vitrous haemorrhage
- fibrous tissue forming anterior to retinal disc
- more common in Type I DM, 50% blind in 5 years
Maculopathy
- based on location rather than severity, anything is potentially serious
- hard exudates and other ‘background’ changes on macula
- check visual acuity
- more common in Type II DM
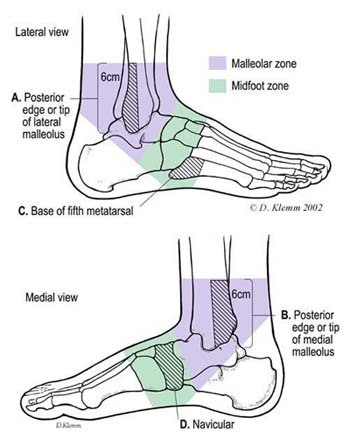
Footballer inverts his ankle and presents with foot pain, surprised he has no ankle pain. What does he have?
Options:
Fractured base of 5th metatarsal
Damaged ligaments
Fractured base of 5th metatarsal
is caused by forcible inversion of the foot in plantar flexion
Associated with Lisfranc injury
Guy jumps and lands on his knee (repeated question)
Options:
medial meniscus tear
patella fracture
damage to ACL
patella fracture

Pulmonary adenocarcinoma Ca met to liver via what route?
Options:
Transcoelomic
Direct invasion
Haem
Lymph
Heamatogenous
Spread:
- local: to pleura, left recurrent laryngeal and phrenic nerve, pericardium, oesophagus, sympathetic chain, and brachial plexus
- Lymphatic: to mediastinal and cervical nodes. Compression of the SVC by massive mediastinal node involvement produces gross oedema and cyanosis of the face and upper limbs
- Blood: to bone, brain, liver and adrenals
- Transcoelomic: pleural seeding and effusion
Cancers which matastasise heamatogenously = Folicular, Renal Cell Ca, Hepatocellular carcinoma
- *Hematogenous–Hepatoma**
- *S**preading – Sarcoma
- *Cancers –Choriocarcinoma**
- *R**eign – Renal cell carcinoma
- *F**oolishly – Follicular carc. of the thyroid
Lady playing squash suddenly runs, hears a crack from behind ankle then pain whenever she tries to plantar flex. What happened?
options:
Ruptured Achilles
Fractured talus
Fractured calcaneus
Achilles tendon rupture
..suspected if the person describes the following whilst playing a sport or running; an audible ‘pop’ in the ankle, sudden onset significant pain in the calf or ankle or the inability to walk or continue the sport.
An examination should be conducted using Simmond’s triad, to help exclude Achilles tendon rupture. This can be performed by asking the patient to lie prone with their feet over the edge of the bed. The examiner should look for an abnormal angle of declination; Achilles tendon rupture may lead to greater dorsiflexion of the injured foot compared to the uninjured limb. They should also feel for a gap in the tendon and gently squeeze the calf muscles if there is an acute rupture of the Achilles tendon the injured foot will stay in the neutral position when the calf is squeezed.
An acute referral should be made to an orthopaedic specialist following a suspected rupture.
Middle aged lady presenting with atypical chest pain – what would be used to decide pre test probability she has ischaemic heart disease?
Options:
Epidemiological evidence of something
Case control study on atypical chest pain RFs
Clinical experience
Exercise ECG
Epidemiological evidence of something
Evidence based medicine works by deciding pre-test probability of something and then doing tests and changing the probability of that thing accordingly.
Pretest Probability
- Definition
- Pretest Probability is defined as the probability of a patient having the target disorder before a diagnostic test result is known. It represents the probability that a specific patient, say a middle-aged man, with a specific past history, say hypertension and cigarette smoking, who presents to a specific clinical setting, like Accident and Emergency, with a specific symptom complex, say retrosternal chest pressure, dyspnoea and diaphoresis, has a specific diagnosis, such as acute myocardial infarction.
- Application
- The pretest probability is especially useful for four things:
- interpreting the results of a diagnostic test,
- selecting one or more diagnostic tests
- choosing whether to start therapy:
- * a) without further testing (treatment threshold);
- * b) while awaiting further testing;
- deciding whether it’s worth testing at all (test threshold)
- Calculation
- The probability of the target disorder, usually abbreviated P(D+), can be calculated as the proportion of patients with the target disorder, out of all the patients with the symptoms(s), both those with and without the disorder:
- P(D+) = D+ / (D+ + D-)
- where D+ indicates the number of patients with target disorder, D- indicates the number of patients without target disorder, and P(D+) is the probability of the target disorder.
- The probability of the target disorder, usually abbreviated P(D+), can be calculated as the proportion of patients with the target disorder, out of all the patients with the symptoms(s), both those with and without the disorder:
- Example:
- A group of investigators in North America studied the underlying diseases found in patients presenting to a primary care setting with persistent dizziness. They studied a total of 100 dizzy patients, finding 16 had dizziness from psychiatric conditions.
- Thus, 16 / 100, or 16 per cent, is the estimate of of disease probability for psychiatric conditions from this study.
- So, if this information proves valid and applicable to your practice, if IF one of your patients presents to a primary care setting with persistent dizziness, the P(D+) of a psychiatric cause might be estimated at 16 per cent.
Person with 4cm head of pancreas ca that has invaded mesenteric vessels. How do you manage?
options
ERCP and biliary stent
PTC drainage
Whipple’s
Vit k
Abx
ERCP and biliary stent
Management
- less than 20% are suitable for surgery at diagnosis
- Resectable:
- a Whipple’s resection (pancreaticoduodenectomy) is performed for resectable lesions in the head of pancreas.
- Side-effects of a Whipple’s include dumping syndrome and peptic ulcer disease
- adjuvant chemotherapy is usually given following surgery
- a Whipple’s resection (pancreaticoduodenectomy) is performed for resectable lesions in the head of pancreas.
- Palliation:
- ERCP with stenting is often used for palliation

Son of 75 year old lady requests home visit for mother who has recent behavioural changes. Sometimes gets confused and sees people in the room who aren’t there. Recent loss of appetite. Cause?
options:
Lewy body dementia
Alzheimer’s
Acute Confusional State
Depression with psychosis
Acute confusional state
is also known as delirium or acute organic brain syndrome. It affects up to 30% of elderly patients admitted to hospital.
Features - wide variety of presentations
- memory disturbances (loss of short term > long term)
- may be very agitated or withdrawn
- disorientation
- mood change
- visual hallucinations
- disturbed sleep cycle
- poor attention
(if not an option, potentially LBD)
Guy post-op with delirium and morphine epidural in situ, what is best initial management?
Options:
Put in well lit side room
Haloperidol
Discontinue morphine epidural
Put in a well lit side room
Management of Acute Confusional State
- treatment of underlying cause
- modification of environment
- haloperidol 0.5 mg as the first-line sedative or olanzapine
Guy with short history of back pain and painless black lesions on his feet appear. What ix do you do?
Options:
Arteriogram
CT abdo
CT abdo with contrast
Abdominal aortic aneurysms occur primarily as a result of the failure of elastic proteins within the extracellular matrix. Aneurysms typically represent dilation of all layers of the arterial wall. Most aneurysms are caused by degenerative disease. After the age of 50 years the normal diameter of the infrarenal aorta is 1.5cm in females and 1.7cm in males. Diameters of 3cm and greater, are considered aneurysmal. The pathophysiology involved in the development of aneurysms is complex and the primary event is loss of the intima with loss of elastic fibres from the media. This process is associated with, and potentiated by, increased proteolytic activity and lymphocytic infiltration.
symptomatic
- pain in the abdomen, loin or lower back
- abdominal pain may spread to the back
- require urgent referral for investigation and management because they may indicate impending rupture
- patient may feel a pulsatile mass in the abdomen
- features of limb ischemia - caused by distal embolisation
- lower extremity oedema
- rarely seen caused by compression of the inferior vena cava
Investigations
- ultrasonography
- non invasive, low cost method with the sensitivity and specificity close to 100%
- measures the size of the aorta in longitudinal as well as in anteroposterior and transverse directions
- modality of choice for initial assessment, follow up, screening and surveillance
- should have a low threshold for arranging abdominal ultrasonography in patients at risk.
- CT
- can visualise
- the proximal neck (the transition between the normal and aneurysmal aorta)
- any extensions of the aneurysm (to the iliac areries)
- patency of visceral arteries
- the presence of blood within the thrombus (crescent sign) - is considered a predictive marker of imminent rupture
- helical CT and CT angiography can provide additional anatomical details - useful if an endovascular procedure is considered
- can visualise
- resonance angiography (MRA)
- safer than conventional arteriography since it does not use nephrotoxic contrast material
- plain radiography
- calcified aneurysmal wall may be seen in some cases
Guy presenting to GP with nocturia. PSA 18, urinalysis trace blood and protein, urea and cr mildly elevated. What do you do?
Options:
Refer routinely to uro
Refer urgently to uro
Refer routinely to renal
Refer urgently to renal
Refer urgently to uro
refer men using a suspected cancer pathway referral (for an appointment within 2 weeks) for prostate cancer if their PSA levels are above the age-specific reference range
Management Programme are as follows:
- aged 50-59 >= 3.0 ng/ml;
- aged 60-69 >= 4.0 ng/ml;
- aged 70 and over > 5.0 ng/ml.
- (Note that there are no age-specific reference ranges for men over 80 years. Nearly all men of this age have at least a focus of cancer in the prostate. Prostate cancer only needs to be diagnosed in this age group if it is likely to need palliative treatment.)
exclude urinary infection before PSA testing. Postpone the PSA test for at least 1 month after treatment of a proven urinary infection (indicated by nitrite and leucocyte on urine dip)
?75 year old lady with 2.5cm firm breast lump not tethered to skin and no skin changes. Daughter 40 year old just had benign breast cyst diagnosed. What does the old lady have?
Options:
Ductal carcinoma
Breast cyst
Lobular carcinoma in situ
Ductal carcinoma
- Age, solitary, firm lump – increases likelihood of cancer vs benign cyst. Ductal (70%) more common than lobullary, proliferative breast disease with atypia = risk factor
Breast cyst
- 7% of all Western females will present with a breast cyst
- Usually presents as a smooth discrete lump (may be fluctuant)
- Small increased risk of breast cancer (especially if younger)
Commonest Single Breast Lumps
- Fibroadenoma
- Cyst
- Fat necrosis
- Cancer
Features of a Malignant Lump
- Irregular, nodular surface
- Poorly defined edge
- Hard / scirrhous consistency
- Painless
- Fixation to skin or chest wall
- Nipple involvement
In this patient AGE makes Ca more likely?
45 year old lady with spontaneous dark brown nipple discharge. Examination reveals only one duct producing discharge. What does she have?
options:
Intraductal papilloma
Duct ectasia
Intraductal papilloma
- Commoner in younger patients
- May cause blood stained discharge originating from a single duct
- There is usually no palpable lump
- NO risk of malignancy
- Growth of papilloma in a single duct
Duct ectasia
- Dilatation breast ducts.
- Most common in menopausal women
- Discharge typically thick and green in colour, which may be from single or multiple ducts (usually present age >50 years)
- Most common in smokers
Tall 28 year old man with radiofemoral delay and hypertension. BP 210/110. Has rib notching. What is underlying diagnosis?
Options:
Coarctation
Marfan’s
ED
Coarctation of the aorta
…describes a congenital narrowing of the descending aorta
more common in males (despite association with Turner’s syndrome)
Features:
- infancy: heart failure
- adult: hypertension
- radio-femoral delay
- mid systolic murmur, maximal over back
- apical click from the aortic valve
- notching of the inferior border of the ribs (due to collateral vessels) is not seen in young children
Associations
- Turner’s syndrome
- bicuspid aortic valve
- berry aneurysms
- neurofibromatosis
Marfans is associated with the following cardiac abnormalities:
- Aortic aneurysm and dissection
- Aortic root dilatation → regurgitation
- MV prolapse ± regurgitation
The post MI papillary muscle rupture question (repeated again)
Revision Qs:
How will this present?
List the complications of an MI
Acute mitral regurgitation
More common with infero-posterior infarction and may be due to ischaemia or rupture of the papillary muscle. An early-to-mid systolic murmur is typically heard and late systolic click. Patients are treated with vasodilator therapy but often require emergency surgical repair.
Death Passing PRAED st.
- Death: VF, LVF, CVA
- Pump Failure
- Pericarditis
- Rupture: myomalacia cordis
- Cardiac tamponade
- Papillary muscle / chordae → MR
- Septum
- Arrhythmias
- Tachycardias
- SVT
- Ventricular T/F
- Bradycardia
- sinus brady
- AV block
- Ventricular brady
- Tachycardias
- Aneurysm: ventricular
- Dressler’s Syndrome: pleuro-pericarditis
Young guy vomiting after a night out presents with chest and epigastric pain, left sided pleural effusion, subcutaneous emphysema. What happened?
Oesophageal rupture
Boerhaave syndrome: Severe vomiting → oesophageal rupture
Defined as: Complete disruption of the oesophageal wall in absence of per-existing pathology. Left postero-lateral oesophageal is commonest site (2-3cm from OG junction). Suspect in patients with severe chest pain without cardiac diagnosis and signs suggestive of pneumonia without convincing history, where there is history of vomiting. Erect CXR shows infiltrate or effusion in 90% of cases
- Other:*
- Mallory-Weiss syndrome: Severe vomiting → painful mucousal lacerations at the gastroesophageal junction resulting in haematemesis. Common in alcoholics*
- Plummer-Vinson syndrome: Triad of: dysphagia (secondary to oesophageal webs) + glossitis + iron-deficiency anaemia. Treatment includes iron supplementation and dilation of the webs*







