What is the difference between substance use, harmful use and dependence?
Most people will use some sort of drug (i.e. caffeine). The issues become more troublesome when there is increasing regular use and start develop a necessity to the drug, or start self-medicating (i.e. take alcohol when they are sad). This can become a spiralling dependence, but this is a small number compared to those who use drugs experimentally. When people become dependent, it is very hard to become independent of the drug.
What is the ICD-10 criteria for Dependence Syndrome?
- A strong desire or sense of compulsion to take the substance
- Difficulties in controlling substance taking behaviour in terms of its onset, termination or levels of use.
- A physiological withdrawal state when substance use has stopped or been reduced
- Evidence of tolerance: need to take more to get same effect
- Progressive neglect of alternative interests
- Persisting with substance use despite clear evidence of overtly harmful consequences.
The key thing is number 2: lack of control. If they don’t have control, they are very likely to be dependent. The relationship with their drug has changed. Who has the control, you or the drug? The drug is all or nothing - a key distinguishing factor; alcoholics can actually go days without drinking, but when they drink, they will drink excessively.
What is the change for Dependence Syndrome Changes from DSM IV - DSM V, and why is it controvertial?
Abuse and dependence are now combined into a single disorder of graded clinical severity - substance use disorder (mild, moderate, and severe).
- Prof Lingford-Hughes does not agree with this as she believes the difference between abuse and dependence exists, and centres on control over the drug; where dependenders have no control over the drug.
- “Dependence” as a label for compulsive, out-of-control drug use has been problematic. Is confusing to physicians and has resulted in patients with normal tolerance and withdrawal being labelled as “addicts” and not getting adequate medication e.g. for pain.
Describe the classical neurobiological model of of Substance Misuse
The key system we need to know about is the dopaminergic mesolimbic system. This allows for natural rewards such as food, sex to increase dopamine levels in a part of the brain called the ventral striatum (in human literature as NAcc is not seen in man) or nucleus accumbens (in animal literature). The neurones start in the midbrain at the ventral tegmental area. Other neurones from the VTA project to the frontal lobe (mesocortical pathway). Together they are called the mesocorticolimbic pathway.
Drugs of abuse, hijack this system, and increase the level of dopamine in the nucleus accumbens. All the drugs do it, you need to know the mechanisms of how they do. Only cocaine and amphetamine modulate the dopaminergic synapses, the rest affect dopamine indirectly.
- Cocaine blocks dopamine re-uptake
- Amphetamine also blocks dopamine re-uptake as well as enhances release of DA
- Alcohol, opiates, nicotine and cannabis increase the level of dopamine firing in the VTA
How can you use imaging to infer striatal DA release?
The model of addiction centering on dopamine release into the NAcc (ventral striatum) is confirmed by PET and SPECT studies. Using [C-11]Raclopride (a D2 antagonist used to treat schizophrenia), you can measure the availability of D2 receptors, which is used to indirectly measure DA relase into the striatum.
Discuss the evidence arround the theory that the euphoric effects of DA underpin the addiction to drugs.
FOR:
- In 1994, when it was demonstrated that intravenous infusion of central stimulant drug and SPECT or PET imaging (of dopamine receptor availability) could be used to indirectly measure DA release in the human striatum, they found that the magnitude of this increase was shown to predict the euphoria produced by the drug.
- HOWEVER, central stimuants specifically act on DA system, so this increase is expected. This finding shows an association rather than proof that change in striatal DA mediates the high.
AGAINST:
- While this may be true for stimulants, studies showed that for alcohol, cannabis and ketamine, these substances did not inevitably induce dopamine release in humans.
- No relationship between striatal dopamine release after cannabis, and any behavioural, subjective or physiological effects of cannabis. (Bossong et al 2009)
- In the case of alcohol, impulsivity and intoxication were linked top dopamine level, but not a drug high.
- Several studies have found that opiate administration was not associated with striatal dopamine release, despite producing a euphoric high. (Nutt, Lingford-Hughes et al 2015, Nature)
What are the three ways/observations the dopamine system is linked to addiction?
- Dopamine and the drug high. Suggested that the euphoria mediated by dopamine release is responsible for the positive conditioning-led learning of addiction.
- Lower striatal dopamine receptor availability indicates the effects of abuse of the Dopamine system. Therefore, they take more drugs to achieve the same high.
- Reward - deficiency. There is a blunted striatal dopamine response after pharmacological challenge. Therefore, they take more drugs to achieve the same high.
Discuss the evidence around the hypothesis that lower D2/3 availability is linked to dependence vulnerability
FOR:
- For cocaine and methamphetamine users, there is a reduction of DA receptor availability, which has been shown to be due to decreased D2/3 expression.
AGAINST:
- No differences in receptor availability between individuals who smoke, and healthy non-smokers irrespective of gender.
- No evidence of changes in striatal DA availability in cannabis addiction.
- Seminal papers by Volkow et al (1999,2002) show that the individuals with low striatal D2/D3, reported more pleasurable effects from stimulants!
Discuss the evdience around the hypothesis that a blunted dopamine system is linked to a vulnerability to developing addiction.
FOR:
- Evidence of blunted striatal DA release after methylphenidate and opiates.
- Young people with high familial risk of addiction but not yet dependent, showed they had reduced amphetamine-induced DA release than matched controls.
- This may indicate that DA release predicts vulnerability to addiction rather than being the cause of addiction, and dopamine release if anything, has a role in resilience against becoming dependent.
AGAINST:
No blunting of DA release was found in cannabis dependence after amphetamine challenge.
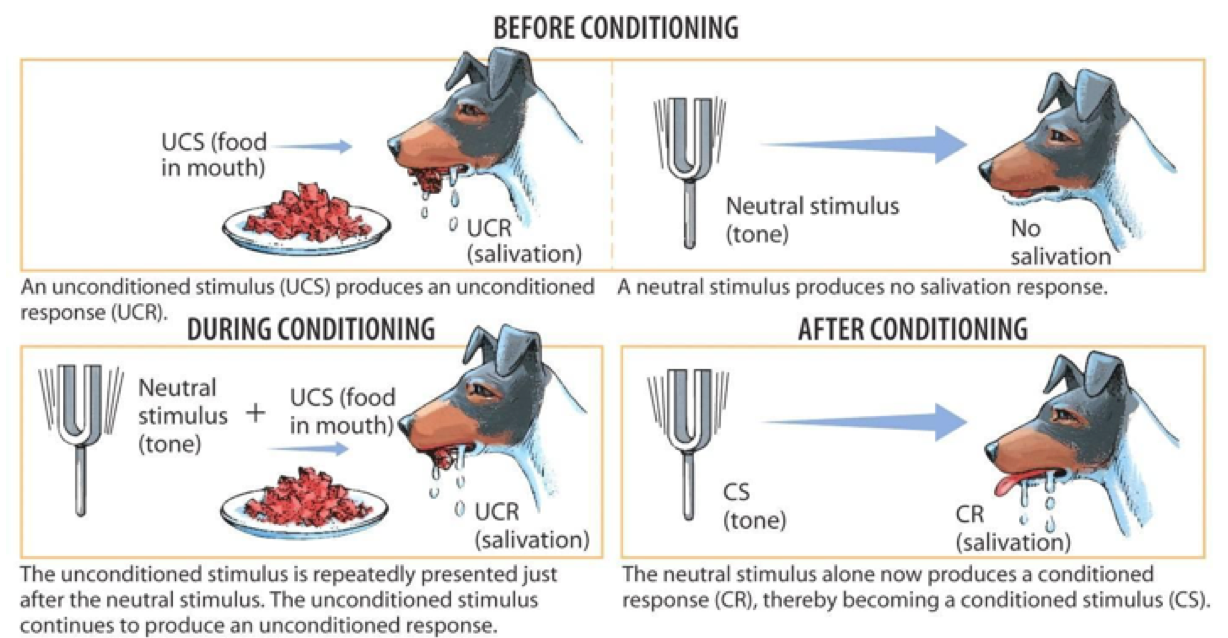
Describe the process of conditioning
In classical conditioning you are associating one stimulus with other stimulus that usually has a response. In the case of pavlov’s dog this is the ring of a bell (uncoditioned stimulus) is associated with food which produces an unconditioned response (salivation). After time, the bell and food become associated so that the bell becomes a conditioned stimulus to salivation (conditioned response).
Describe the role of GABA in addiction
GABA inhibits the dopaminergic neurones of the VTA. The GABA-B receptor is the key system. Baclofen is a typical agonist. It is shown to improve abstinence rates in alcohol dependence. Other drugs that increase GABA levels have similar effect.
The basal release of dopamine is not harmful, only the phasic release. GABA acts as a break. Phasic firing of the dopamine neurones tells the brain this a good/interesting thing, implicated in conditioning.
Describe the role of opiate receptors in addiction.
- Mu receptors inhibitory receptors on GABA-ergic neurones that project to the VTA dopaminergic neurones to act as a ‘GABA break’ to phasic dopaminergic firing. So Mu receptor activation blocks this GABA break, leading to increased DA in the NAcc –> pleasure.
- Kappa receptors ??location ??mechanism cause dysphoria. The kappa receptors are like a negative feedback trying to halt the pleasure.
During aquision of dependence behaviour: Alcohol stimulates the opiate receptors ?mu more than kappa? this increase in mu/dopminergic activity leads to an increase in kappa receptors. In dependence, your kappa system becomes dysregulated.
This high kappa tone persists after alcohol is stopped being consumed, leading to dysphoria/withdrawal. This effect drives relapse, and more alcohol is needed to counter the kappa tone. This kappa dysphoria may be what is driving the impulsivity that is seen when there is increased DA (due to kappa stimulation).
Describe the role of cannabis in addiction/dependence
The GABA break is also regulated by the cannabinoid system. The CB1 receptor is on the GABA neurone, and is also inhibitory. Similar to the mu system. However, difficult to show that it changes dopamine levels.
The active susbtance in cannabis is delta9-tetrahydrocannibol, but also has other active substances such as cannabidiol (which may be antipsychotic). CB1 and CB2 receptors are G-protein coupled.
- CB1 is mainly found in brain, neuronal with a few on the microglia
- CB2 is mainly found in immune cells and the liver and spleen.
Our endogenous cannabinoids are anandamine and 2-AG
What are the stages of the addiction cycle?
- Binge/intoxification. Here the stimulus-response habits are formed.
- Withdrawal/negative affect. This has a function of negative reinforcement.
- Preoccupation/craving. Involves representation of contingencies, outcomes, their percieved values and subjective states.
What are the neurocircuitry involved of the stages of addiction?
- Binge/intoxification. Here the stimulus-response habits are formed.
- Role of the reinforcing effects of drugs that engage the reward neurotransmitters and associated mechanisms in the nucleus accumbens. Mainly by dopamine and opioid peptides.
- Withdrawal/negative affect. This has a function of negative reinforcement.
- The negative states of withdrawal may engage the activation of the amygdala, and subsequent release of corticotroping releasing factor (–> stress of cortisol).
- Preoccupation/craving. Involves representation of contingencies, outcomes, their percieved values and subjective states.
- This is mediated by the processing of conditioned reinforcement and the contextual information by the hippocampus and the executive control by the prefrontal cortex.
What is contingency management?
Contingency management is using incentives/rewards to encourage the frequency of positive behaviour (in the case of addiction – abstinence). It is based on the theory of operant conditioning, whereby positive reinforcement of a behaviour will increase the probability that the operant (voluntary) behaviour will take place.
Describe the principles and practice of contingency management.
- Developing a strategy/therapeutic approach. The goal is to establish a clear contingent relationship between achieving the target behaviour and the reinforcement:
- Select a positive behaviour consistent with treatment goals which is under voluntary control and can be regularly and unambiguously measured. For heroin, this behaviour can be abstinence, which is measured through urinalysis.
- Develop a clear reinforcement schedule that promotes the chosen behaviour. The patient should have a choice in what reward they want. Provide simple, clear information explaining the procedures to patients.
- Measure whether the target behaviour is achieved. This should be done in an objective and consistent manner. Should also be done frequently.
- If the target behaviour is achieved, reward should be given immediately. Furthermore, the magnitude of the reward must be sufficiently large to compete with the other behaviour. There should be an element of escalation where each positive step is rewarded, but attainment of more significant treatment goals involves greater reward.
- Reinforcement must be withheld if the target behaviour is not achieved. However, you must remain with a positive and empathetic approach for all interactions, and neutral but not punitive for undesired results.
Describe the theory of operant conditioning
BF Skinner argued that human behaviour was best understood by looking at the causes of an action and its consequences. Skinner’s theory of “Operant conditioning” identified different forms of reinforcement that increase or decrease the likelihood of a behaviour being repeated:
- Positive reinforcement - increasing the behaviour by providing a reward. E.g. giving a voucher if behaviour is attained.
- Negative reinforcement - increasing the behaviour by removing an averse stimulus when a behaviour occurs. E.g. less intense supervision if behaviour is attained.
- Positive punishment - decreasing the behaviour by administering an averse stimulus
- Negative punishment / extinction - decreasing the behaviour by not administering a reward.
Discuss the moral and ethical issues raised by the use of financial (and other) incentives in contingency management of addiction
The use of financial incentives in healthcare is controversial because:
- Bribery: paying people to act against their wishes
- However, they are being offered rewards to achieve outcomes that are most desirable, not forced into acting against wishes
- Coercion: compels people to behave using pressure/duress
- But it is voluntary, with a prospect of gain, not loss
- Paternalistic: undermines individual autonomy
- But it could be said to facilitate autonomy when it makes it more likely that people act in line with their originally considered preferences (people who actually wanted to quit smoking)
- Unfair: people should not be paid to do what they should do
- But it is potentially a more effective way of changing behaviour and improving health
- Waste of money: poor use of the public purse, where there are many competing demands
- But there are potentially large health benefits from a modest increase in health expenditure. Also may be more effective than current strategies, plus saves a lot of money in the long-term
Describe the evidence of efficacy of contigency management
- Retention: Contingency management is significantly more effective in retaining cocaine users in treatment than counselling alone.
- Methadone maintenance: Has the most substantial evidence base, proving large and consistent effects. Participants remain abstinent for up to 6 months, and is cost-effective.
- Higgens et al 1994, found higher abstinence in cocaine users when vouchers and lottery tickets where given. Involved urinalysis and counselling.
- Adherence to physical health interventions. Contingency management doubled (2x) the rate of HepB vaccination and TB testing, and tripled the rate of 6 month return.
How does fMRI measure neuronal activity?
fMRI exploits changes in magnetic properties of the blood, e.g. as oxygen is removed. This can be detected using an MRI measure known as the blood oxygen level dependent (BOLD) signal. The BOLD signal is the ratio change in oxyhaemoglobin to deoxygaemoglobin in the venous blood. As neuronal activity in response to a particular thought process requires oxygen, the BOLD signal at that location during that process will increase.
- At the very low and very high levels of activity, it’s not a linear gradient (though it is linear in the middle)
The BOLD signal is, indirectly, a measure of neuronal activity. We can infer that these correlate to an increase in certain neurotransmitter systems due to the anatomical correlates of activity, but we cannot say unequivocally.
What are the higher-order processes of interest in the study of addiction?
The higher-order processes of interest in the study of addiction are:
- Behavioural control
- Decision making
- Emotional reactivity
- Reward sensitivity
These are systems we believe are compromised in those who are likely to develop addiction disorders, as well as compromised because of neurochemical disturbances caused by drug intake. These neurochemical disturbances may disappear with abstinence, allowing patients to engage in better decision making and reward sensitivity. Importantly we may be able to develop drugs to treat these neurochemical disturbances.
What is cognitive control?
Cognitive control refers to the process that allows behaviour to vary adaptively from moment to moment - e.g. response inhibition. Cognitive control can inhibit behaviours and impulses. The prefrontal context is predominantly responsible for this top-down control.
What are the major players in the cognitive control networks?
Major players in cognitive control networks include:
- anterior cingulate cortex/pre-supplementary motor area (ACC/pSMA)
- dorsolateral prefrontal cortex (DLPFC)
- inferior frontal junction (IFJ)
- anterior insular cortex (AIC)
- dorsal pre-motor cortex (dPMC)
- posterior parietal cortex (PPC)



