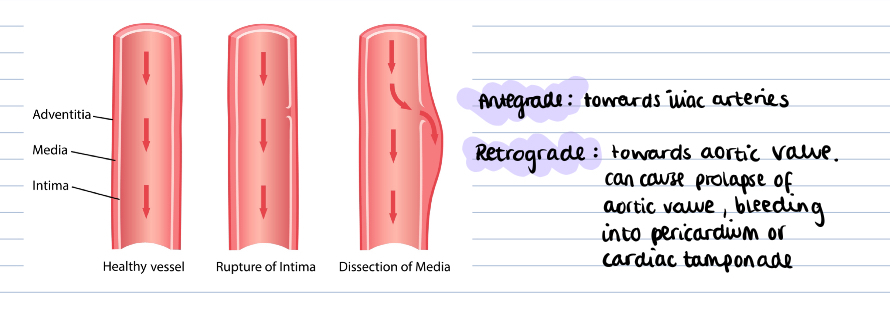
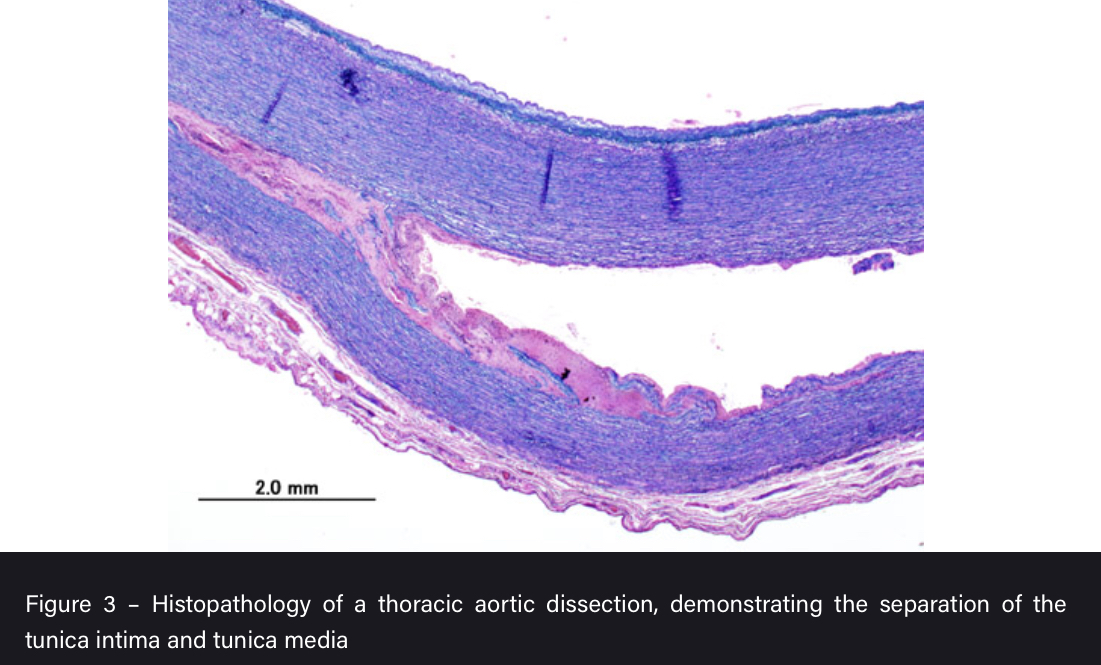
What is an aortic dissection?
A tear in the intimal layer of the aortic wall causing blood to flow between the tunica intima and media, splitting the two apart
Acute < or equal to 14 days to diagnosis
Chronic > 14 days to diagnosis
How can aortic dissections be classified?
Stanford Classification
A - Debakey Type I and II involving ascending aorta
B - Debakey Type III and do not involve ascending aorta
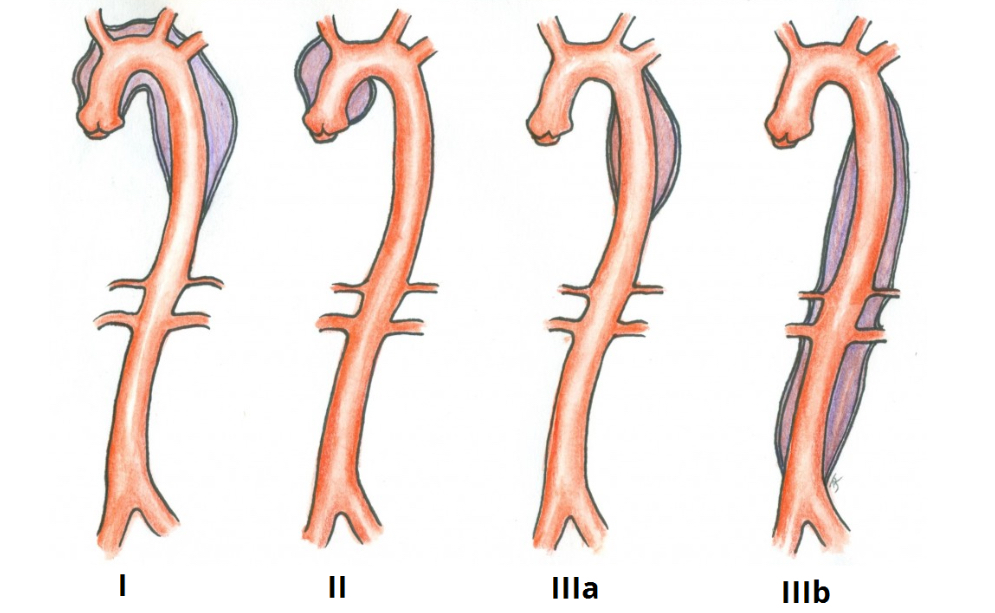
DeBakey Classification
I - originates in ascending aorta and propagates to at least aortic arch
II - confined to asending aorta
III - originates distal to subclavian artery in descending aorta
What are some risk factors for an aortic dissection?
- Hypertension
- Atherosclerotic diease
- Male
- Connective tissue disorders (Marfan’s and EDS in younger pt)
- Bicuspid aortic valve
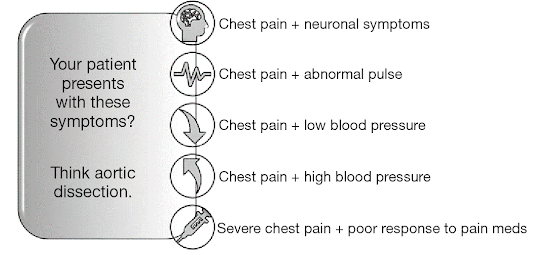
What are the clinical features of an aortic dissection and what are some differentials?
- Tearing chest pain that usually radiates to back
- Tachycardia, hypotension, aortic regurg murmur
- Signs of end-organ hypoperfusion e.g reduced urine output, lower limb ischaemia
DD: MI, PE, Pericarditis, MSK back pain
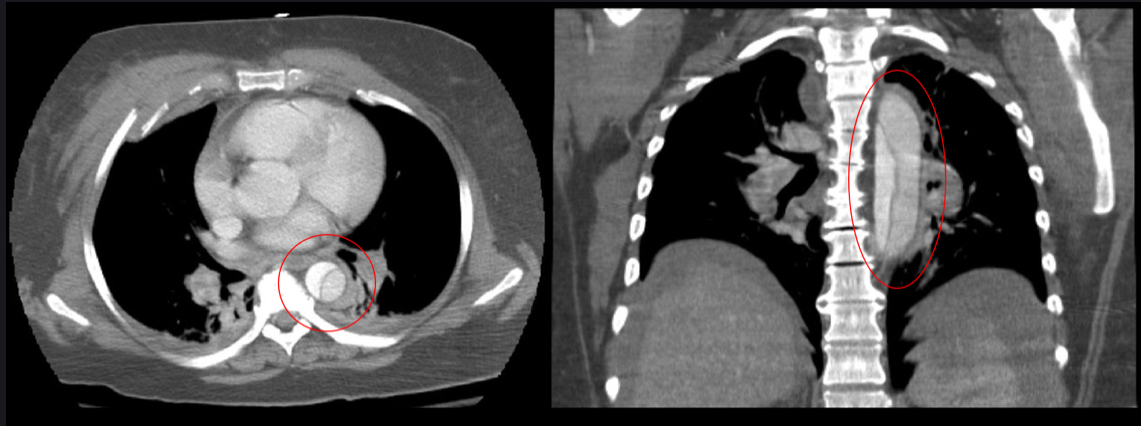
How do you investigate a suspected aortic dissection?
- Bloods (FBC, U+Es, LFTs, troponin, coagulation) with crossmatch of at least 4 units
- ABG
- ECG to rule out cardiac pathology
- CT angiogram diagnosis gold standard 1st line
- Can do transoesophageal ECHO
How should you manage an aortic dissection generally?
- Initial: high flow oxygen, IV access with 2 large bore cannulas, fluid resus with target BP<110
- Stanford A: managed surgically as worse prognosis
- Standford B: can be managed medically if uncomplication
- Lifelong antihypertensive therapy and surveillance imaging at 1,3,12 months
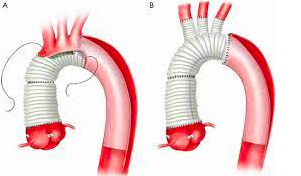
How are Type A dissections managed?
- Transfer to cardiothoracic centre
- Remove ascending aorta and replace with synthetic graft
- Reimplant branches of aortic arch to graft
How are Type B dissections managed?
MEDICALLY DUE TO RISK OF RETROGRADE DISSECTION IF MANAGENED SURGICALLY
1st line: IV beta blockers (labetolol) or CCB to lower systolic pressure and minimise dissection
Complicated: if rupture, ischaemia, pain or uncontrollable HTN then surgical repair
What are some complications of aortic dissections?
- Aortic rupture
- Aortic regurgitation
- MI if coronary artery dissection
- Cardiac tamponade
- Stroke or paraplegia if cerebral or spinal artery involved
- Type B can become chronic and form aneurysm