Acute rheumatic fever (ARF)
Aetiology
- GAS infection (Beta haemolytic) à Strep. pyogenes
- URTI à pharyngitis and multisystemic infection
NOTE: need 3 factors to be present
- Genetic susceptibility
- Autoimmune response
- Environment with GAS (acquire infection)
Pathogenesis
- Molecular mimicry – auto Ab attack host Ag as well as GAS M protein
- Affects heart, joints, brain, blood vessels (complex deposition)
- Inflammation and immune cell activation
Gross features
Pancarditis
- Pericarditis: fibrinous bread and butter appearance from vasodilation à fibrin deposition
- Myocarditis: Aschoff bodies (see microscopy)
- Endocarditis: ulcers on valve free edge from high pressure à expose self Ag à autoAb deposition à inflammation
Microscopic features
Active inflammation – Aschoff bodies in all 3 layers
- Fibrinoid necrosis
- Activated macrophages (Anitschkow caterpillar cells) and giant cells
- T lymphocytes à considered ‘chronic inflammation’
Extra cardiac manifestations
- Pericardial rub- sounds like walking on snow
- Fever, SOB (hear failure, declined cardiac output
- Mitral/ valve regurgitation (systolic and pansystolic murmurs)
- Erythema marginatum, subcutaneous nodules, polyarthritis of large joints, syndenham’s chorea
Rheumatic Heart Disease
Aetiology
Successive episodes of ARF causing cumulative heart damage
Pathogenesis
- Repeated inflammation from GAS à healing and scar formation
- Long term effects solely involve endocardium à valve stenosis and regurgitation from scarring à valve insufficiency
- Mitral valve most prone: exposed to highest pressures in heart à wear and tear à exposure of self Ag à more inflammation from GAS
Gross features
Valve leaflet thickening
- Commissural fusion of leaflets à ‘fishmouth appearance’ à stenosis
- Short, thick, fused chordae tendinae
Microscopic features
- Fibrous scarring (collagen bundles)
- Neovascularisation- release of angiogenesis factors during healing
- Calcification
Clinical features
- Loud S1 (valve cusps widely apart at systole onset)
- Palpable S1 (tapping apex beat)
- Mitral stenosis
- Mitral facies : low CO and pulmonary HTN à cutaneous vasodilation (cheeks and acral cyanosis)
- Dyspnoea, orthopnoea, PND
- Oedema, ascites
- Fatigue (pulmonary HTN)
- Haemoptysis (ruptured bronchial veins à pulmonary HTN)
Complications
Mitral stenosis à LA pressure overload à LA dilation à AF
- LA dilation and AF predispose to thrombosis à large mural thrombus
- Embolus à stroke
- If severe obstruction à heart failure from no systemic blood flow
- Subacute bacterial endocarditis (SBE)- septic emboli, septicaemia, renal/spleen infarcts
SEVERE RHD: Pulmonary congestion from LA overload à pulmonary HTN à pulmonary vessel changes à increased RV afterload à RV hypertrophy
Bacterial endocarditis:
Colonisation of the heart valves by bacteria. Destructive lesions causing valve dysfunction. At risk if alcoholic, immunosuppressed, IVDU, neutropenic.
Acute and Sub-acute endocarditis
ABE (Acute Bacterial Endocarditis)
SBE (subacute bacterial endocarditis)
Clinical features
- Rare, elderly, IVDU
- High virulence- Staph. aureus
- Normal valve
- Morbidity and mortality even with AB treatment / surgery
- Common, any age
- Low virulence- Strep. viridans
- Abnormal valve- calcific/RHD
- Infected wks-months
- Recover post AB treatment
Clinical signs
- Rapid fever
- Chills
- Lassitude
- Murmurs if left side heart affected
- Microemboli à petechiae, splinter haemorrhages, Janeway lesions, Osler nodes
- Flu-like
- Fatigue
- Weightloss
- Splenomegaly
Complications
- Glomerulonephritis- complex deposition
- Haematuria, albuminuria, renal failure
same
- Congenital heart diseases (common) – ASD, VSD, PDA, FT
ASD
VSD
PDA
FT
Epidemiology
most common presentation of CHD as adult
most common CHD however many close spontaneously in childhood
7% of all CHD
most common cause of cyanotic CHD
5% of all CHD
Aetiology
abnormal atrial septation
incomplete septation of ventricles
rarely can get acquired VSD post MI or trauma
lack of closure of PDA at birth
risk fx for non-closure = maternal rubella syndrome, prematurity, hypoxia
due to abnormal anterior superior displacement infundibular outflow tract portion of the interventricular septum
may be associated with Digeorge syndrome (microdeletion of chromosome 22)
relevant embryology
on septation: 1st to develop is septum primum with the ostium secundum in it, then the septum primum with the foramen ovale
normally ductus arteriosus closes at birth due to increased arterial oxygenation, decreased pulmonary vascular resistance and decreased local levels of prostaglandin E2 - becomes ligamentum arteriosum
Features
fixed hole between atria after birth allowing communication between L&R atria
fixed hole between ventricles (membranous part of ventricle rather than muscular portion)
note: can be part of TOF
patent ductus arteriosus (hole between left pulmonary artery and aorta)
4 features:
- Pulmonary stenosis
- Overriding aortic receives blood from both ventricles
- RVH
- VSD
may have PDA or ASD = protective
Classification
most common is ostium secundum (90%)
3 types:
Ostium secundum: due to inadequate formation of septum secundum
Ostium primum: due to failure of septum primum to fuse with endocardial cushions
Sinus venosus (caval): absence of normal tissue btwn right pulmonary vein and right atrium
R to L or L to R shunt
left to right shunt
left to right shunt
left to right shunt
right to left shunt
Cyanotic or acyanotic
acyanotic
BUT: L-R shunt = exposure of low pressure, low resistance pulmonary circulation to increased pressures and volumes - leads to adaptive changes to increase lung vascular resistance in order to protect the pulmonary bed –> pulmonary HTN –> reversal of shunt from R –>L = cyanotic (EISENMENGER SYNDROME) –> clubbing, polycythemia
cyanotic except can be acyanotic with mild pulmonary stenosis
Clinical fx
usually asymptomatic
if symptomatic: dyspnea on exertion, fatigue, arrhythmias (palpitations) due to right atrial enlargement
small or large defects
asymptomatic w/ small
large defects: RV hypertrophy, pulmonary HTN and CCF (can get shunt reversal and cyanosis)
small defect: asymptomatic
large defect: pulmonary HTN
cyanosis
polycythemia (increased RBCS)
fallot’s sign (learn to squat to increase afterload and decrease R-L shunt)
Tet spells – cyanotic episode after crying/feeding
Complications
Eisenmenger syndrome
high pressure shunt can predispose to infective endocarditis
Eisenmenger syndrome
high pressure shunt can predispose to infective endocarditis
can predispose to LRTI
high pressure shunt can predispose to infective endocarditis
increased risk of infective endocarditis and paradoxical embolization
Important examination/diagnostic findings
abnormal heart sounds: S2 = widened, fixed split pattern (because normal respiratory variation in systemic venous return venous return is countered by reciprocal changes in volume of blood shunted across ASD)
may get systolic murmur in pulmonary area or mid-diastolic murmur in tricuspid area (due to increased volume of blood across valve)
harsh pansystolic murmur heard best at left sternal border
may be palpable thrill
continuous machinery like murmur
loud systolic ejection murmur in pulmonary area (pulmonary stenosis)
CXR: large, boot shaped heart due to RVH
Basic management
surgical/intravascular ASD closure
surgical VSD closure if doesn’t close spontaneously
indomethacin (anti-PGE2 – which keeps PDA patent)
surgical repair
- Other valvular disorders – e.g. aortic stenosis, mitral valve prolapse
- Aortic stenosis
- triad of aortic stenosis: syncope/ dizziness, chest pain, SOB
- causes: senile calcific aortic stenosis, calcification of congenitally deformed valve, post-inflammatory scarring (RHD)
- calcific aortic stenosis = most common cause, can be senile or related to congenital bicuspid valve
- risk fx: congenital abnormality –> bicuspid aortic valve (normally 3 cusps)
- calcification + fibrosis/scarring from progressive age associated wear and tear
- thick, irregular, fibrosed valves with nodules of calcification
- can present with LVH and hypertrophy
- Mitral valve prolapse
- Mitral valve balloons into LA
- Causes:
- MI
- Primary: congenital degeneration
- Marfans syndrome – fibrillin mutation
- On clinical examination: MID-SYSTOLIC ejection click +/- mitral regurgitation – caused by abrupt tension on redundant valve leaflets and chordae tendinae as the valve attempts to close
Cardiomyopathies = intrinsic myocardial dysfunction due to structural or electrical abnormality w/o significant inflammation
Dilated
Hypertrophic
Restrictive
Epidemiology
most common
least common
Type of dysfunction
systolic dysfunction
diastolic dysfunction
diastolic dysfunction due to decreased ventricular compliance (stiff ventricle due to fibrosis/substance deposition)
Morphology
Gross: flabby enlarged heart with 4 chamber dilation, often mural thrombi
Gross: septum is thicker than ventricular free wall (uneven hypertrophy), banana lumen
Microscopic: hypertrophy and disorientation of myofibers with fibrosis
note: hypertrophy due to HTN is NOT hypertrophic cardiomyopathy – will be unilateral thickness of heart wall and normal array of muscle fibers
Gross: ventricles of normal size (or slightly enlarged)
no luminal dilation
firm/rigid myocardium
Aetiology:
PRIMARY: genetic (20-50%) – present at younger age, dystrophin defect
SECONDARY
alcohol *** (COMMON)
peri-partum
haemochromatosis
chronic anaemia
drugs (doxorubicin)
idiopathic
hyperthyroidism
viral infections (myocarditis)
100% Genetic defects of sarcomere proteins (defect in energy transfer from mitochondria to sarcomere and/or direct sarcomere dysfunction) – abnormal beta-myosin
main causes:
1) idiopathic
2) radiation induced fibrosis
3) amyloidosis (amyloid plaque deposition)
4) endomyocardial fibrosis (fibrosis of endocardium and myocardium due to nutritional deficiencies or inflammation from helminth infections)- CHILDREN
5) Loeffler endomyocarditis (hyper-eosinophilia peripherally and eosinophilic tissue infiltrates) – ADULTS
Clinical info
slowly progresses to CHF with very low LV ejection fraction
atrial fibrillation and stroke
DDx: ischaemic heart disease, valvular heart disease
SOB, CHF, atrial fibrillation and thrombosis (stroke)
who: common cause of sudden death in young athletes
DDx: hypertensive heart disease, aortic stenosis
DDx: pericardial constriction
Other info
type of DCM disorder = arrhythmogenic RV cardiomyopathy à only get dilation of right heart due to inherited.rare defect à often leads to ventricular tachycardia and fibrillation (arrythmogenic = creates arrhythmias)
Microcirculation and fluid balance
Fluid movement between vascular and interstitial spaces by two opposing forces:
Vascular hydrostatic pressure
Colloid osmotic pressure (produced by plasma proteins)
Normally, outflow of fluid produced by hydrostatic pressure at arteriolar end of microcirculation is neatly balanced by inflow due to slightly elevated osmotic pressure at the venular end – only small net outflow of fluid into interstitial space, drained by lymphatic vessels.
Key issues: upstream and downstream effects of valvular regurgitation and/or stenosis; effect of tachycardia; hyper dynamic cardiac states; the development and consequences of pulmonary hypertension; the determinants and consequences of atrial fibrillation
Upstream and downstream effects of valvular regurg and/or stenosis
- Stenosis = failure of valve to open completely, obstructing forward flow
- Insufficiency = failure of valve to close properly, allowing regurgitation (backflow) of blood
- Effects: ventricular hypertrophy, predisposing to ischaemia and angina; systolic and diastolic dysfunction collude to cause CHF and cardiac decompensation, syncope
Hyperdynamic cardiac states
- Hyperdynamic circulation = abnormally increased circulatory volume
- Hyperdynamic circulation can be due to: exercise or emotion, fever, pregnancy, thyrotoxicosis, anaemia
- Can often present with a collapsing pulse
Development and consequences of pulmonary hypertension
- Pulmonary circulation is low resistance and low pressure
- Pulmonary hypertension = pulmonary pressures reach 1/4th or more of systemic levels (normally around 1/8th of systemic pressures)
- Often secondary to a decrease in cross-sectional area of pulmonary vascular bed or increased pulmonary vascular blood flow
- Causes include:
- Chronic obstructive or interstitial lung disease
- Recurrent pulmonary emboli
- Previous heart disease e.g. mitral stenosis
- Pathogenesis:
- Mostly due to pulmonary endothelial cell and/or vascular smooth muscle dysfunction
- Endothelial cell dysfunction reduces production of vasodilatory agents and increase vasoconstrictive mediators in secondary pulmonary hypertension
- In primary form, e.g. uncommon familial form, there are other processes including TGF-beta signalling pathway
Determinants and consequences of atrial fibrillation
- Determinants: AF can be due to myocardial ischaemia (atrial infarction), mitral valve disease, thyrotoxicosis, hypertensive heart disease, sick sinus syndrome, pulmonary embolism, myocarditis, fever, acute hypoxia
- Uncoordinated chaotic atrial contractions reduce ventricular stroke volume and can also cause stasis and can form thrombi -> leading to strokes or infection in other organs.
What is left heart failure? What is right heart failure? What is bi‐ventricular cardiac failure? What are their main causes and the clinical features?
· Heart failure is the inability to adequately perfuse tissues and organs – i.e. Cardiac output does not meet the demands of the tissues and organs
· Left-sided heart failure – Heart failure due to inability of left ventricle
o There is a reduction in left ventricular output and an increase in left atrial and pulmonary venous pressure. An acute increase in left atrial pressure causes pulmonary congestion or pulmonary oedema; a more gradual increase in left atrial pressure, as occurs with mitral stenosis, leads to re ex pulmonary vasoconstriction, which protects the patient from pulmonary oedema. This increases pulmonary vascular resistance and causes pulmonary hypertension, which can, in turn, impair right ventricular function.
o Clinical features – Pulmonary oedema (bibasilar crackles, or clear, frothy sputum in cough), fatigue, SOB, pale
o Common causes – MI, hypertension, anaemia, HIV, AIDS, congenital birth defect, heart valve disease, drugs,
· Right-sided heart failure – Heart failure due to inability of right ventricle
o There is a reduction in right ventricular output and an increase in right atrial and systemic venous pressure.
o Clinical features – Elevated JVP, peripheral pitting oedema, hepatomegaly, SOB, fatigue, pale, cool peripheries
o Causes of isolated right heart failure include chronic lung disease (cor pulmonale), pulmonary embolism and pulmonary valvular stenosis.
· Biventricular heart failure – Heart failure due to inability of both ventricles
o Failure of the left and right heart may develop because the disease process, such as dilated cardiomyopathy or ischaemic heart disease, affects both ventricles or because disease of the left heart leads to chronic elevation of the left atrial pressure, pulmonary hypertension and right heart failure.
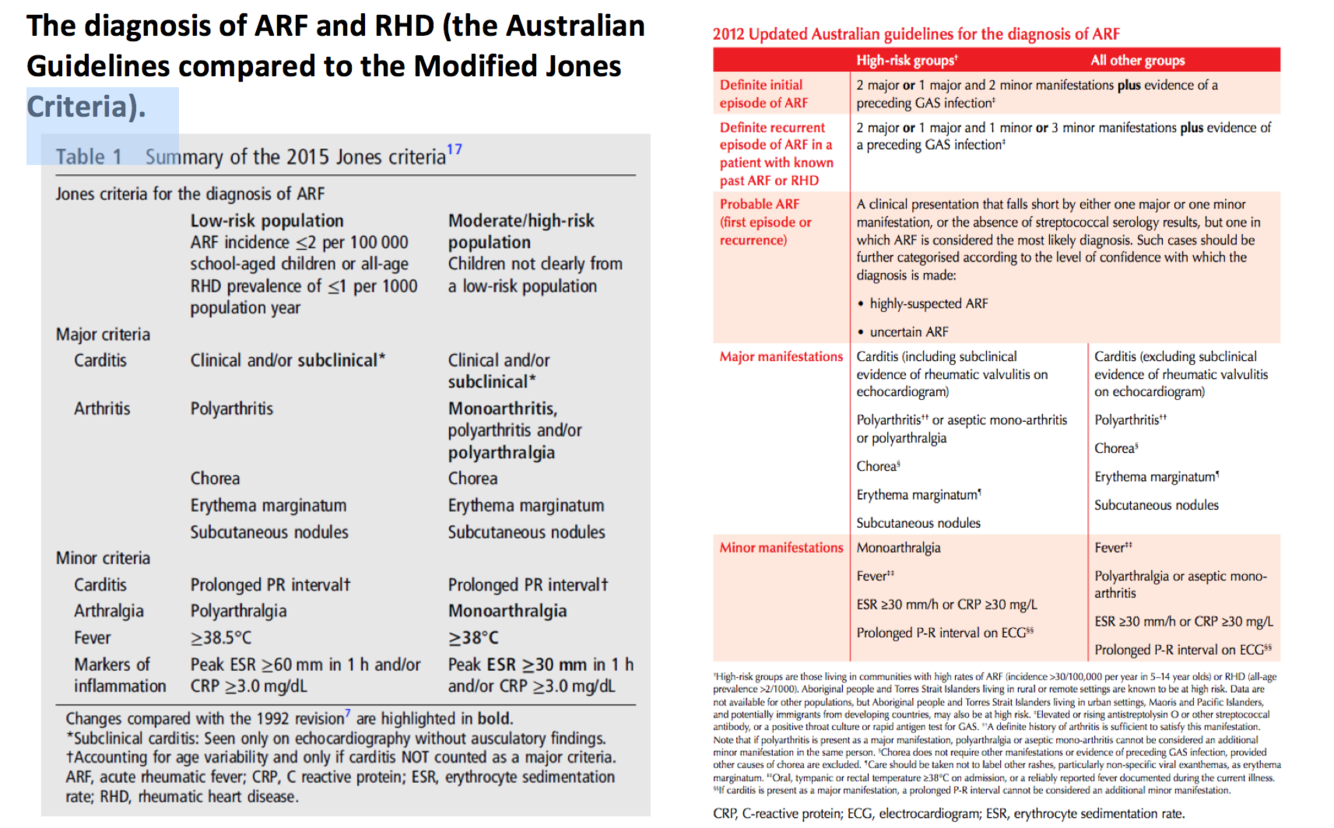
ARF and RHD Diagnosis
The diagnosis of ARF and RHD (the Australian Guidelines compared to the Modified Jones Criteria).
Valvular disorders
Mitral regurgitation: Pansystolic murmur. Acute – no dilatation of left atrium so large left v wave is seen and murmurs will be soft because atria pressure is high. Stroke volume is reduced so L ventricle hypertrophy to maintain CO resuling in punding of apex. Chronic stage – L atria dilatation -> pulmonary congestion and odema (worsening dyspnea). Secondary L ventricular failure -> fatigue due to reduce CO. Mid systolic click due to tensing of valve’s chordae tendineae.
Mitral stenosis: Early stage - Mid diastolic murmur with opening snap because of buildup of atria pressure. Loudest at end diastole from atrial contraction. Palpable left parasternal thrill due to left atria hypertrophy from pressure overload. Mitral facies due to dilatation of arteries and venous congestion. Pulse become weak due to decrease CO. Reactive pulmonary hypertension (loud P2). Late stage – the valve becomes less pliable so softer murmur. Atrial fibrillation (systemic emboli). Pulmonary edema and hypertension (worsening dyspnea) -> congestion lead to right ventricular failure.
Tricuspid regurgitation: Pansystolic murmur. Functional – when right ventricle is dilated. Organic – infective endocarditis. Signs of RHF.
Tricuspid stenosis: Mid diastolic murmur. Increase R atria pressure à hepatomegaly, ascites and dyspnea.
Pulmonary regurgitation: Decrescendo diastolic murmur.
Pulmonary stenosis: Mid systolic murmur. RHF signs. Fatigue and syncope.
Aortic regurgitation: Early diastolic decrescendo murmur best heard at left para sternum 4th intercostal space. Symptoms only appear after L ventricular failure at late stage. L ventricular hypertrophy (increase demand) and reduce diastolic pressure (reduce coronary perfusion) lead to angina and dyspnea.
Aortic stenosis: crescendo-decrescendo systolic murmur. Reduce CO -> fatigue. L ventricular hypertrophy from pressure overload. During exercise CO cannot increase due to restricted orifice – Demand > supply result in angina and SOB. S4 due to reduce L ventricle compliance. Ejection click (early systolic due to doming of abnormal valve.
Heart Murmurs
Infective Endocarditis
Acute caused by high virulence organisms - MRSA. Pyrexia, hematuria, sepsis and emboli ( present as petechiae ) of unknown origin, general malaise, and new mumurs.
Subacute caused by low virulence – Strep viridans. Persistent low grade fever and non-specific symptoms.
Diagnosis: Duke’s Criteria Major – 1. Positive blood culture with typical pathogens (strep viridans, abiotrophia and granulicatella species, strep bovis, Staph aureus, HACEK or enterococcus) 2 samples 12 hours apart. 2. Echocardiogram shows endocardial involvement. 3. New regurgitation. 4. +ve Q fever. Minor – 1. predisposed heart condition or IVDU (Note IVDU often result in right heart lesions). 2. Vascular phenomena – emboli or rupture. 3. Immunological phenomena – glomerulonephritis and osler node. 2major1minor. 1major3minor.
It’s important to understand the concepts of primordial, primary and secondary prevention of ARF/RHD - and tertiary management. How could you explain some of these concepts to Ms JM and her family?
Primordial prevention - aims to minimise risk factors for a disease in a population. This means preventing group A strep infections through improvement to environment, economic, social & behavioural conditions that are known to increase the risk of infections.
Examples - improved housing and reduced overcrowding.
Primary prevention - aims to prevent complications from a known problem. Includes early diagnosis of group A strep throat infections in people most at risk of ARF (typically children aged 5-14 years), & treatment with antibiotics, commonly penicillin.
Secondary prevention - early detection of disease & measures to prevent recurrent disease & worsening of the condition. This means preventing recurrent ARF which in turn prevents RHD or stops existing RHD worsening. Secondary prophylaxis with regular benzathine penicillin G is the only RHD control strategy shown to be effective.
Tertiary prevention - aims to prevent complications once a disease is established. In the vase of RHD, this means reducing symptoms to minimize disability & prevent premature death. Examples - heart valve surgery, medication to manage heart failure, & prevent stroke.
7. Revision of primary, secondary, tertiary and quaternary prevention.
Primary prevention - methods to avoid occurrence of disease. Most population-based health promotion efforts are of this type.
Secondary prevention - methods to diagnose and treat existent disease in early stages before it causes significant morbidity (stopping the progression of deterioration)
Tertiary prevention - methods to reduce negative impact of extant disease by restoring function and reducing disease‐related complications (returning of a patient to a status of maximum usefulness with a minimum risk of recurrence of the disorder).
Quaternary prevention - methods to mitigate or avoid results of unnecessary or excessive interventions in the health system.
- What are the likely long-term challenges of secondary prophylaxis for ARF/RHD?
Long term prophylaxis reduces the risk of progression to serious cardiac disease, potential need for valve surgery and warfarin risks (stroke, endocarditis, premature death). The challenges that present are:
- monthly clinic contact for a painful needle
- hard to commit to being in the right place
- having access to health care
- the needles are required every 28 days - difficult during school excursions, family holidays, going out bush, unexpected funerals to attend, etc.
- complications from IMI especially of needle administered poorly - hematoma, abscess
- potential for adverse penicillin reaction
- potential for other organisms to become penicillin resistant
