Embolism- types of thromboembolism- types of thrombus and embolism
An embolism is a detached intravascular solid, liquid of gaseous mass that is carried by the blood from its point of origin to a distant site, where is causes dysfunction or infarction.
Types of thrombi
Important features
Mural thrombi
Thrombi occurring in the heart chambers or aortic lumen. MI, arrhythmias, dilated CMPs predispose to mural thrombi.
Arterial thrombi
Occlusive, found in coronary, cerebral and femoral arteries.
Venous thrombosis (phlebothrombosis)
Occlusive, veins of lower extremities most often involved
Vegetations (thrombi on heart valves)
Blood borne bacteria or fungi adhere to previously damaged valves.
Type of embolus
Pulmonary embolus
Originate from DVTs and are the most common type of embolus. Rarely, a venous embolus passes through interatrial or interventricular defect and gains access to the systemic arterial circulation- paradoxical embolus.
Systemic thromboembolism
Most arise from intracardiac mural thrombi, 2/3rds of which are associated with left ventricular wall defects. Most lodge in the lower extremities or the brain.
Fat and marrow embolism
Microscopic fat globules can occasionally be found in the pulmonary vasculature after fractures of long bones (associated with hematopoietic bone marrow).
Air embolism
Gas bubbles within the circulation can coalesce to form frothy masses that obstruct vascular flow and cause distal ischemic injury. Decompression sickness is a common type of gas embolism in divers.
Myocarditis: common types including infective and toxic myocarditis
Myocarditis is a group of conditions in which an infectious micro-organism and/or primary inflammatory processes cause myocardial injury. Viral infections are a common cause of myocarditis- coxsackie viruses A and B and other enteroviruses. HIV, CMV, influenza are some less common cause of viral myocarditis. Non viral causes include protozoan and parasitic infections such as typanosoma cruzi and toxoplasmosis. Some drugs such as cancer therapy, lithium, chloroquinine.
Morphology
Grossly the heart appears normal or dilated, some hypertrophy may be present. It is often flabby with pale foci or minute haemorrhagic lesions. Mural thrombi may be present.
Microscopically, active myocarditis is characterised by oedema, interstitial inflammatory infiltrates and monocyte injury.
Clinically the disease can be completely asymptomatic or lead to heart failure and arrhythmias.
- Syphilitic cardiovascular disease
Syphilitic aortitis accounts for 80% of the cardiovascular manifestations of tertiary syphilitic disease. The pathogenesis of this disease is unknown, but it is thought the immune response has a role to play. Aortitis leads to slowly progressive dilation of the aortic root and arch, which causes aortic valve insufficiency and aneurysms of the proximal aorta.
Population research in CVD (e.g. Framingham study).
- Framingham study:
- What is it: long-term and ongoing cardiovascular cohort study of residents in Framingham Massachusetts (began in 1948) – now on 3rd generation of participants à before this study not much known about CV risk fx
- Framingham study: major findings
- Smoking increased heart disease
- Increased BP (even borderline HTN) and cholesterol increase risk
- Exercise decreases risk of heart disease
- Obesity increases risk
- High HDL – reduces risk
- Afib associated with increased mortality and increased stroke risk
- Menopause found to increase risk of heart disease
- Psychological fx found to affect heart disease
- CRP increased – RR of CV event much higher
- Framingham risk score
- 10 yr CV risk of an individual can be estimated with the Framingham risk score (based on major findings of study)
- limitations: only predicts future coronary heart disease events not risk of stroke, TIA and heart failure
- Brief review of concepts of primordial prevention, primary prevention, secondary prevention and tertiary management.
- PRIMARY: promotion of health and prevention of illness (e.g. regular exercise, good diet)
- SECONDARY: early detection/screening and prompt intervention to correct any mishaps from good health or to treat early signs (cholesterol and BP control and regular checks)
- TERTIARY: reduce complications and suffering from illness (medications, surgery e.g. CABG)
- Role of population screening for risk factors in clinical settings.
- Early intervention – primary and secondary rather than tertiary prevention – cheaper on health system, lower morbidity and mortality
- Gives patients time to change their behaviors – encourage them that it’s never too late
- How do we change people’s behaviour / lifestyle to prevent lifestyle diseases? Health Promotion.
- Ottawa charter: 5 action areas for health promotion
- Build healthy public policy
- Create supportive environments
- Strengthening community action
- Developing personal skills
- Reorienting health care services toward prevention of illness and promotion of health
- Need multisector involvement, need to enable health equity to allow individuals to become empowered to control the determinants that affect their health, need to advocate for health as a resource for social and developmental means
- Motivational interviewing techniques
Acute Coronary Syndrome – Practical Management
- Provide oxygen, insert bilateral 20g cannula into cubital fossa and draw bloods, administer Morphine 2.5mg IV, aspirin 150-300mcg.
- 12-lead ECG, BP, P, O2 Sats, GCS (out of 15)
- Based on ECG findings provide GTN
- GTN contraindicated – inferior STEMI – RV infarction – relying on blood pressure for preload
- Look for ST elevation in V1 and larger ST elevation in Lead 3 than Lead 2
- Provide beta blockers
- Perform CXR
- Give reperfusion therapy if:
- ST elevation 1mm in 2 contiguous limb leads
- ST elevation 2mm in 2 contiguous precordial leads
- New LBBB pattern
- Types: PCI or if not available, Fibrinolysis
Note: don’t give the fibrinolysis if they’ve had a recent stroke or any kind of intracranial injury because will bleed everywhere
Blood Tests:
- FBC – anemia, infection, Hb if going for surgery
- EUC – K+, renal hypoperfusion (urea, creatinine)
- LFT – if suspected Gall Bladder pathology
- Lipase – to rule out Pancreatitis
- Troponin (TnI or TnT) – repeat at 4 hours
- Elevated 3-4 hours after heart attack
- Creatine kinase MB (CK-MB)
- Detectable 3-6 hours post heart attack, peak 12-24, normal by 48-72 hours.
- Normally undetectable or very low
Call Cardiology:
- Percutaneous Coronary Intervention – Angioplasty/Stent
- CABG
- Fibrinolysis
Medications MOA:
- GTN – Nitric Oxide – activates guanylate cyclase = increase in cGMP – close Ca++ channels, dephosphorylation myosin light chain = vasodilation
- So decrease in venous return, decrease preload, decrease work of heart so requires less O2
- Beta blockers eg Atenolol, Bisoprolol – Bind circulating adrenaline and noradrenaline
- Antagonists of beta adrenergic receptors in SA node, AV node, ventricular muscle = decreased influx of Ca++
- So beats slower, not as forceful contraction so less O2 demand, longer diastole so heart gets more blood supply
- Aspirin/Clopidogrel – to reduce incidental thrombus formation
Clinical Features of chest pain
- Angina Pectoris
- Blockage = decreased O2 = switch from mitochondrial oxidative phosphorylation to anaerobic glycolysis = increased lactic acid and decreased pH = sensed by sympathetic nerve fibres = pain
- Stable Angina: chest/neck/shoulder/arm pressure/pain brought on by exercise and relieved by rest
- Unstable Angina: pain that comes on at rest
- Myocardial Infarction: associated with nausea and diaphoresis – results in permanent damage to myocardium
Process of care
- What advice should a GP give if this patient rings for help?
- Reassure the patient and remind them to remain calm
- Tell the patient (or whoever is present with patient) to call 000 immediately (tell them to describe their symptoms and state that they could be having a heart attack)
- If aspirin is available, tell the patient to take 1 adult-strength or 2-4 low-dose aspirin (aspirin prevents blood from clotting)
- Wait for an ambulance; tell the patient not to drive themselves
- How is ACS best managed in a rural setting? What facilities would exist locally e.g. Ravenshoe, Hughenden or Emerald?
- ABCDE (with defibrillator on hand), followed by a targeted history and examination
- Establish venous access with an IV cannula and attach a cardiac monitor and pulse oximeter to the patient
- In a rural setting, a patient with acute chest pain or other symptoms suggestive of acute coronary syndrome should receive a 12-lead ECG, and the results analysed by a clinician within 10 minutes of the first emergency clinical contact
- Give aspirin 150-300 mg orally unless contraindicated by known hypersensitivity
- Give GTN 150-300 g sublingually, and add morphine 2.5-5 mg IV with an antiemetic (e.g. metoclopramide 10 mg IV) if pain persists
- Commence heparin for all patients with a suspected NSTEMI or unstable angina
- In rural and remote areas, fibrinolysis may start before hospital arrival
- Sending blood is futile as results will take several days to return (if blood was to be taken – FBC, coagulation profile, ELFTs, cardiac biomarker assay such as cardiac troponin I or troponin T and lipid profile)
- Organise urgent transfer to a regional hospital (Townsville Hospital) - in a rural or remote setting the management of ACS is usually considerably more complex and involves general practitioners or community health centres, prehospital care providers, retrieval services (such as Careflight and the Royal Flying Doctor Service) and regional and metropolitan referral hospitals
Acute percutaneous coronary intervention [PCI: angiography, angioplasty, stenting]; and stenting, thrombolysis [if immediate PCI unavailable], urgent surgery, anticoagulation [short term and long term].
- Percutaneous coronary intervention (PCI)
- Angioplasty: used to treat blockages in the coronary arteries and restore normal blood flow to hear – catheter delivered via peripheral artery (femoral or radial) to provide access to coronary arteries
- Expandable balloon used to dilate vessel by expanding at site of blockage (usually inflating and deflating multiple times)
- Stenting: metallic stents also can be deployed at site of blockage to improve vessel diameter and maintain patency as just expanding using balloon can result in re-stenosis of vessel if stent not used
- Stents = metal mesh tubes to dilate affected arteries
- Can be either drug-eluting or bare-metal
- Coronary angiography: what we see in cath lab – x-ray imaging of coronary arteries using contrast agents injected into bloodstream
- able to see flow of blood as well as any blockages in arteries
- see through a number of different views or axes of the heart
- patient stays awake, will receive LA into site of catheter, as well as benzodiazepines if required for relaxation (?GTN?)
- Indications:
- To improve anginal symptoms in patients with unacceptable angina and at least 1 significant coronary artery stenosis (i.e. more than 70% diameter)
- In stable IHD to improve survival
- To improve anginal symptoms in patients with unacceptable angina and at least 1 significant coronary artery stenosis (i.e. more than 70% diameter)
- Thrombolysis (for STEMI)
- Pharm approach (fibrinolytics) to revascularisation that can be used for patients with STEMI who are not candidates for mechanical revascularisation such as PCI
- Pt. may not be able to reach facility that conducts PCI within 120 minutes
- Pt. may prefer thrombolysis over mechanical revascularisation
- Absolute contraindications:
- Hx of intracranial haemorrhage, known structural cerebral vascular lesion, ischaemic stroke within past 3 months, suspected aortic dissection, active bleeding, intracranial/intraspinal surgery within past 2 months, severe uncontrolled hypertension
- Choices of fibrinolytic agents include tenecteplase and reteplase
- Adjunctive anti-thrombotic therapy is also recommended including aspirin, unfractioned heparin and enoxaparin
- Pharm approach (fibrinolytics) to revascularisation that can be used for patients with STEMI who are not candidates for mechanical revascularisation such as PCI
- Urgent surgery
- Prompt surgery indicated for most mechanical complications after STEMI e.g. acute papillary muscle rupture, or ventricular septal rupture
- Urgent CABG indicated for patients w/ STEMI and coronary anatomy not amenable to PCI if ongoing or recurrent ischaemia, cardiogenic shock, severe heart failure, or other high-risk features
- Anticoagulation
- Short term
- Aspirin as soon as STEMI is suspected
- Loading dose of P2Y12 inhibitor ASAP or at time of PCI
- E.g. clopidogrel
- Primary PCI -> IV unfractionated heparin
- Fibrinolytics -> IV unfractionated heparin, aspirin + clopidogrel
- Do not use NSAIDs
- Long term
- ?
- Short term
Discharge management and cardiac rehabilitation
- Discharge management
- Initiate long-term management plan for all patients with ACS
- Medicines
- Chest pain action plan
- Warning signs of heart attack, when and how to take GTN, self-admin of aspirin, when to call ambulance
- Identify risk factors and refer to secondary prevention programs
- Consider guideline-recommended medicines for all patients with ACS
- Combination of antiplatelet agents, beta blocker, statin, and ACE inhibitor recommended for most patients unless contraindicated
- All proven to reduce subsequent cardiac events and death
- Combination of antiplatelet agents, beta blocker, statin, and ACE inhibitor recommended for most patients unless contraindicated
- Identify risk factors and refer all patients with ACS to secondary prevention programs
- Refer all patients to cardiac rehab program (proven effective intervention and reduces risk of further cardiac events)
- Provide smoking-cessation advice
- Provide tools for pt. self-management
- Communicate management plan to patient, carers and community healthcare providers
- Adherence to therapy
- Long-term management
- Initiate long-term management plan for all patients with ACS
- Cardiac rehab
- Helps patient adopt healthy lifestyle, feel more confident, connect with people, prevent recurrence of cardiac events
- Aims = maximise physical, psychological and social functioning in people w/ cardiac disease; introduce/encourage behaviours to minimise further cardiac events and conditions
- Can be face-to-face, over the phone, online, in group, in hospitals or in own home
- Inpatient rehab:
- ASAP after admission to hospital
- Basic information and reassurance
- Action plan, psychological issues, social factors
- Supportive counselling
- Reassurance and support for pt and family as part of routine daily care
- Mobilisation and resumption of activities of daily living
- Balance b/w risk and effects of bed rest
- Promotes self-confidence
- Discharge planning
- Outpatient rehab:
- Assessment, review and follow-up
- Low or moderate intensity physical activity
- Education, discussion and counselling
- Anatomy and phys of heart, heart disease, risk factors, psychological issues, social factors, management of symptoms, action plan to ensure early response to symptoms of a possible heart attack, medications, cardiac health myths, importance of follow-up
- Physical activity supervision, emergency procedures and equipment
- Risk of cardiac even in low to moderate physical activity is low and benefits are high
- Exercise and testing
- Monitoring and evaluation
https://www.heartfoundation.org.au/images/uploads/publications/Recommended-framework.pdf
Diagnostic Imaging
Coronary Angiography:
- Involves arterial catheterisation under X-ray guidance so that the catheter may be guided to the heart.
- Contrast dye is ejected into a cardiac chamber or blood vessel so that blood flow throughout the coronary vessels may be observed.
- The extent, severity of coronary stenoses, thrombus and calcification may be determined
- Information for planning, conduction and evaluation of coronary intervention and bypass graft surgeries can be done using coronary angiography.
Nuclear scanning techniques:
- Gamma-emitting radionuclides with a short half-life has made it possible to study cardiac function non-invasively (e.g. technetium tetrofosmin)
- Are being superseded by superior imaging techniques
- Blood pool imaging
- Isotope injected intravenously à mixes with circulating blood
- Gamma camera detects the amount of radiation-emitting blood in the heart in different phases of the cardiac cycle
- Can be used to measure ventricular ejection fractions
- Size and shape of the cardiac chambers can also be assessed
- Myocardial perfusion imaging
- Scintiscans of the myocardium are obtained at rest and during stress after administration of an intravenous radioactive isotope.
- PET can be used for more quantitative information – can also assess myocardial metabolism
Echocardiography:
- Cardiac ultrasound
- An ultrasound transducer is placed on the chest wall so real time images may be seen as a 2D slice
- Allows rapid assessment of structure and function
- EF and ventricular thickness can be estimated
- Diagnosis and quantification of severity of valve disease can be conducted
- Identification of vegetations in endocarditis
- Identification of structural heart disease in atrial fibrillation, cardiomyopathies or congenital heart disease
- Detection of pericardial effusion
- Identification of structural heart disease or intracardiac thrombus in systemic embolism
- Doppler echocardiography
- Uses Doppler principle – sound waves reflected from moving objects undergo a frequency shift – the greater the frequency shift the faster the object is moving
- Speed and direction of blood can be detected in heart chambers and blood vessels
- Can detect valvular regurgitation – turbulence and reverse in blood flow can be observed
- In stenosis – blood accelerates through narrow orifice – can observe this
- Transoesophageal echo:
- Transthoracic sometimes produces poor images – especially if patient overweight or has obstructive airways disease
- Some structures difficult to visualise in transthoracic
- Left atrial appendage, pulmonary veins, thoracic aorta and interatrial septum
- Uses endoscope like ultrasound probe – passed into oesophagus under light sedation à positioned behind the LA
- Can see congenital abnormalities, mitral valve dysfunction, aortic dissection, smaller vegetations, systemic embolism
Exercise echo or stress echo:
- For patients who are unsuitable for exercise stress testing – e.g. mobility problems, pre-existing bundle branch block
- Echo is performed before and after infusion of a moderate to high dose of an inotrope, such as dobutamine
- Myocardial segments with poor perfusion become ischaemic and contract poorly under stress (wall motion abnormality observable)
Cardiac CT:
- 320 slices per rotation can be taken à high resolution imaging
- Can see the cardiac chambers, great vessels, pericardium and mediastinal structures and masses
- Can be performed using timed injection of X-ray contrast to produce clear images of blood vessels and associated pathologies
- Contrast very useful for aortic dissection and pulmonary embolisms
- Can quantify coronary artery calcification – index of cardiac risk
- Has a high negative predictive value in patients with chest pain and low-moderate likelihood of disease.
- Some scanners can assess myocardial perfusion
MRI cardiac imaging.
- No radiation – cross-sectional images of the heart, lungs and mediastinal structures
- Provides better differentiation of soft tissue structures than CT but is poor at demonstrating calcification
- When gated to ECG produces moving images of the heart and mediastinal structures during the cardiac cycle
- Very useful for aortic dissection, heart anatomy definition, infiltrative conditions of the heart and great vessels in patients with congenital heart disease
- RV hard to visualise in echo (retrosternal position) – but can be seen in MRI
- Myocardial perfusion and viability can be seen when a contrast agent is injected – areas of hypoperfusion seen
- Better resolution than nuclear medicine techniques
- Later redistribution of contrast à identifies scarring and fibrosis
How do we know that research is valid?
- Validity can be expressed in different ways Internal/Criterion validity – what goes on within a study (whether the researcher tested what was meant to be tested) and External/Ecological validity – what happens outside of the study (how well the findings can be generalised to other situations and people).
- To maximise validity, any potential confounding or extraneous variables need to be minimised. So to ensure your findings are valid, the research itself needs to be as tightly controlled as possible to avoid other variables other than those being measured affecting the results. If findings do not solely show the effect of one Independent variable on a Dependent variable, the research’s validity is reduced.
- To ensure validity, instruments and methods used during research must first be reliable. Without reliability, results cannot be accurate and therefore the study cannot measure what it was intended to measure, reducing the validity of the study itself. If data is not reliable, through inaccurate data collection/experimental methods, the results automatically cannot be valid.
- Data such as qualitative data can be reliable because of the depth and detail involved, but does this lend itself to validity? Qualitative data can be valid as it is true to life, but perhaps only valid for one person or a small minority? It’s very difficult to generalise Qualitative data to the larger population, but does this mean that data is still valid? Or are the findings therefore invalid as a whole?
- To know whether your findings are valid, surely you must question all aspects of research as to how methods could invalidate findings. Only when these factors have been eradicated to the best of the researchers’ ability can your findings be valid.
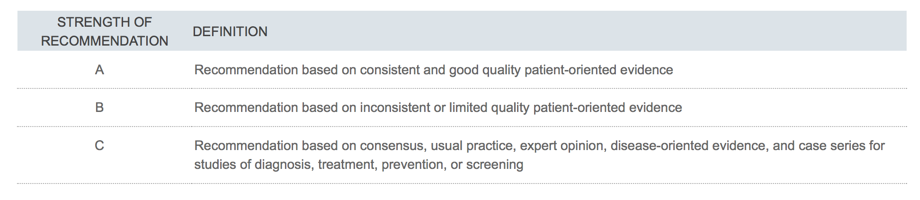
What is strength of evidence? (EBM).
Outline the principles of evidence based medicine.
The practice of EBM involves five essential steps first, converting information needs into answerable questions; second, finding the best evidence with which to answer the questions; third, critically appraising the evidence for its validity and usefulness; fourth, applying the results of the appraisal into clinical practice; and fifth, evaluating performance.
Motivational interviewing about the modifiable risk factors: T2DM, HTN, Diet, physical activity, and smoking habit.
Informed consent is when the patient make decision about their management after they have been given pertinent information about their current illness. It is an ethical and legal obligation.
Complication of MI he should know: Sudden cardiac death, embolism from mural thrombus to vital organs, arrhymias (palpitation), SOB due to ventricular failure, ventricular wall rupture.
Patient from a rural town so difficult to get advance management such as percutaneous coronary intervention, and cardiac myocytes death occur after 24 hours.
Its better if family and doctors are involved in making decision. Family members will know his wishes and doctor can provide advice based on his clinical experiences. But final decision has to come from patient.
Probably do not have ample time to think because chest pain occurred recently and want to thrombolyse or PIC ASAP to savage the area at risk.
Ask the patient for the reason of the decision to check if he understands the advantages and disadvantages of the management.
Previous medical consultations may compromise your medical treatment‐patient
compliance/second opinion/patients understanding of the seriousness of their medical
condition. How do you deal with this? Let the patient know the seriousness of this condition - SCD.
Is difficult to be certain patient is rushed into making a decision in an emergency.
If patient cannot give informed consent in an emergency, always act on the interest of the patient. This can be sourced from third parties such as his wife who may know his wishes, they have the power to object treatment for the patient. Resuscitate unless wish is stated on advance health directive.
Patients might like to know what is MI, PIC and thrombolysis. The advantages and disadvantages of the management plan.
