Surgical plan for correction of subvalvular aortic stenosis
- Diffuse form:
- (basically a septal myectomy or Ross kono
- or a Nicks procedure)
- Aortoseptal approach
- Preserve the aortic valve if normal
- Septal resection or patch
- Ross-Kono procedure vs a mechanical prosthesis
- Valve-preserving technique
- Incision through the left and non coronary commissure into the roof of the LA and across the mitral (Nicks procedure?)
- Replacethe mitral and patch the annulus/roof of the LA
- Reclose the aorta preserving the aortic root
- Aortoseptal approach
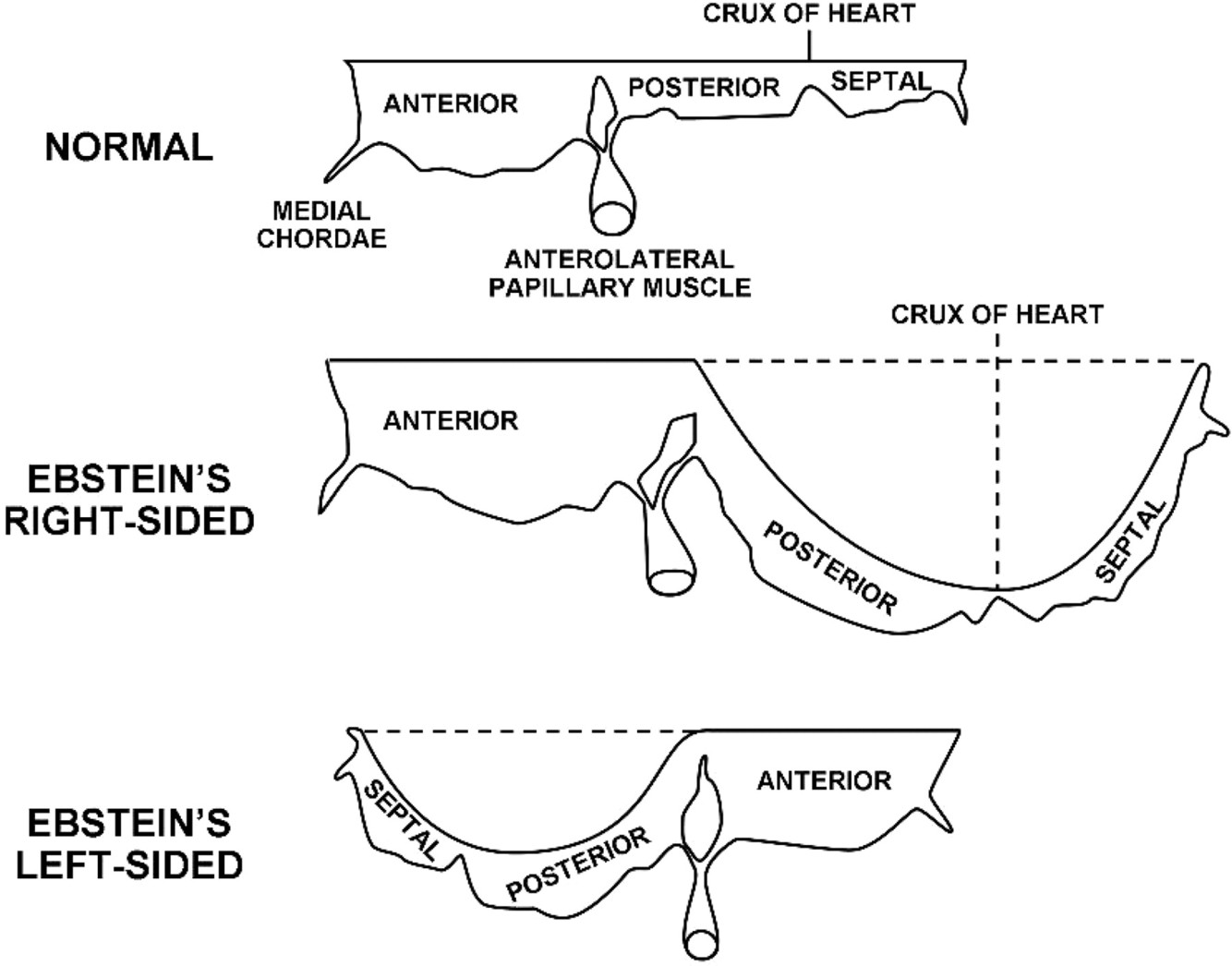
Ebstein’s Anomaly
Features of the tricupid valve
- Septal leaflet is always affected
- Posterior leaflet: almost always
- Anterior leaflet involvement is unusual, but is usually large and sail-like
- The leaflets are typically adherent to the RV wall
Chamber morphology in Ebstein Anomaly
- RA is dilated, with a PFO or ASD
- RV is atrerialized: thin and dilated
- Extreme form is Uhl’s Disease, with a large parachute RV
- Papillary: Shortened chordae to a small papillary muscle (which can be obstructive)
Ebstein Anomaly
Indications for early repair
- Anatomic pulmonary atresia
- Congestive heart failure
- Ventilator dependent
- Failed medical therapy
- Persistent cyanosis
Usually is two of these at once
GOS Ratio
GOS Score: Great Ormond Street ratio
Calculated from 4 chamber echo view
Area of the RA + arterilized RV / area of RV+LA+LV
Radio > 1 correlates with a poor px
General surgical strategy in the treatment of single ventricle syndromes
- First stage:
- palliation as a neonate
- Second stage:
- Palliation during the first year
- Third stage:
- Palliation (Fontan) between ages 1-5
Morphologic subsets of single left ventricle
Morphologic Subsets of Single ventricle physiology:
- Tricuspid atresia
- Double inlet left ventricle
- Mitral atresia
Tricuspid Atresia - standard anatomic classification
Types – Relate to the relationship of the great vessels
Type I (70%): Normally related great vessels
Type II (30%): D-Transposition
Subsets: status of the pulmonary valve
A: Pulmonary atresia
B: Pulmonary Stenosis
C: Normal pulmonary valve
Tricuspid atresia
Subset A
Subsets: status of the pulmonary valve
A: Pulmonary atresia
B: Pulmonary Stenosis
C: Normal pulmonary valve
Tricuspid atresia - subset B
Subsets: status of the pulmonary valve
A: Pulmonary atresia
B: Pulmonary Stenosis
C: Normal pulmonary valve
Morphogy of the tricuspid atresia physiology
- Muscular (70%)
- AV connection is absent.
- Membranous (three variants)
- Fiberous diaphragm blocks the AV orifice (imperforate valve membrane )
- Classic Ebstein anomaly which is imperforate
- AV septal type with imperforate Right side valve
Tricuspid atresia - what is the more comon form of AV valve discontinuity ?
- Muscular (70%)
- AV connection is absent.
- Membranous (three variants)
- Fiberous diaphragm blocks the AV orifice (imperforate valve membrane )
- Classic Ebstein anomaly which is imperforate
- AV septal type with imperforate Right side valve
Tricuspid atresia - what are the anatomic varriants of the less common type of discontiuity betwen the RA and RV ?
- Muscular (70%)
- AV connection is absent.
- Membranous (three variants)
- Fiberous diaphragm blocks the AV orifice (imperforate valve membrane )
- Classic Ebstein anomaly which is imperforate
- AV septal type with imperforate Right side valve
How does tricuspid atresia first present?
The presentation depends mainly on the subtype
Cyanosis is mainly type 1-
- Type 1A, 1B, tricuspid atresia
- DILV with reduced PVF (PS or pulmonary atresia)
Congestive heart failure:
- Type IIc – tricuspid atresia
- DILV with TGA from the rudimentary chamber
Tricuspid atresia - which patients typically present with cyanosis ?
Cyanosis is mainly type 1-
Type 1A, 1B, tricuspid atresia
DILV with reduced PVF (PS or pulmonary atresia)
Congestive heart failure:
Type IIc – tricuspid atresia
DILV with TGA from the rudimentary chamber
Tricuspid atresia
which variants present with Heart failure?
Cyanosis is mainly type 1-
Type 1A, 1B, tricuspid atresia
DILV with reduced PVF (PS or pulmonary atresia)
Congestive heart failure:
Type IIc – tricuspid atresia
DILV with TGA from the rudimentary chamber
Tricuspid Atresia
What is the second procedure?
Timing?
- Bidirectional caval pulmonary anastomosis
- Secondstage paliation is at 3-6 months
What patient is the ideal fontan candidate
- Age > 2 years
- LV morphology
- Mean PAP < 15mmHg
- PVR < 2WU
- Large un-obstruve PA’s
- No ventricular hypertrophy
- Normal EF (>50%)
- LVADP < 12mmHg
- No AV valve regurgitation
- No subaortic stenosis
Forntan operative mortality
< 5%
Fontan - 15 year survival
60-70%
Typical presentation of a HLHS
Clinical features/Diagnosis
Male (70% are male) presenting as a newborn with cyanosis and tachypnea
Gender predominance with HLHS
70% are male
Medical support of HLHS
- PGE-1 for ductal patency
- Maintain HCT 45-50%
- Balance pulmonary blood flow: proper respiratory maintenance allows for significant support
- FiO2 0.18 – 0.21 (not hi fio2) to give a systemic O2 sat of 70-75%
- Maintain higher than regular PCO2 40-50
- No atrial septostomy
Role of the ventilator in pre-op HLHS
Balance pulmonary blood flow: proper respiratory maintenance allows for significant support
FiO2 0.18 – 0.21 (not hi fio2) to give a systemic O2 sat of 70-75%
Maintain higher than regular PCO2 40-50


