COPD - history?
P: dx date, symptoms, baseline ET
R: smoking, FH (alpha-1-AT), occupational exposures (dust, coal, fumes, gases). Risk factors for disease exacerbation: GORD, compliance, OSA, infection
I: spirometry, PFT, ABG, ECG/TTE - was it just GP diagnosis or had formal PFT?
C: adherence to therapy, follow-up, smoking cessation, understanding of action plan
M: action plan, pulmonary rehab, LAMA+LABA+ICS+prophylactic ABx, home O2, nebs, BiPAP, lung reduction surgery?
C: RVF, frequency of hospital admissions, ICU, steroids, NIV, resistant organisms, PTX, steroid side effects (topical, systemic), pulmonary HTN
P: current control, ET, mMRC SOB, exacerbation last 12 months, freq of FU, understanding of prognosis and ACD
How is the patient coping? How is it affecting them?
MRC dyspnoea scale?
0 - not breathless
1 - SOB when hurrying or walking up a slight hill
2 - more breathless compared with people of similar age, has to stop for breath when walking at own pace
3 - stops for breath at about 100m or few minutes only
4 - housebound, breathless when dressing
COPD - examination to comment on? (4)
COPD: cachexia, nicotine staining, flap, cyanosis, tracheal tug, prolonged FET
Chest: Reduced chest expansion, breath sounds, wheeze.
Features of steroid use: Cushingoid, ecchymosis
Pulmonary HTN
GOLD classification of severity of COPD? (Global initiatives for chronic Obstructive Lung Disease)
To diagnose COPD, FEV1/FVC <70%
GOLD 1 (mild): FEV 1 >80%
GOLD 2 (moderate): 50-80%
GOLD 3 (severe): 30-50%
GOLD 4 (very severe): <30%
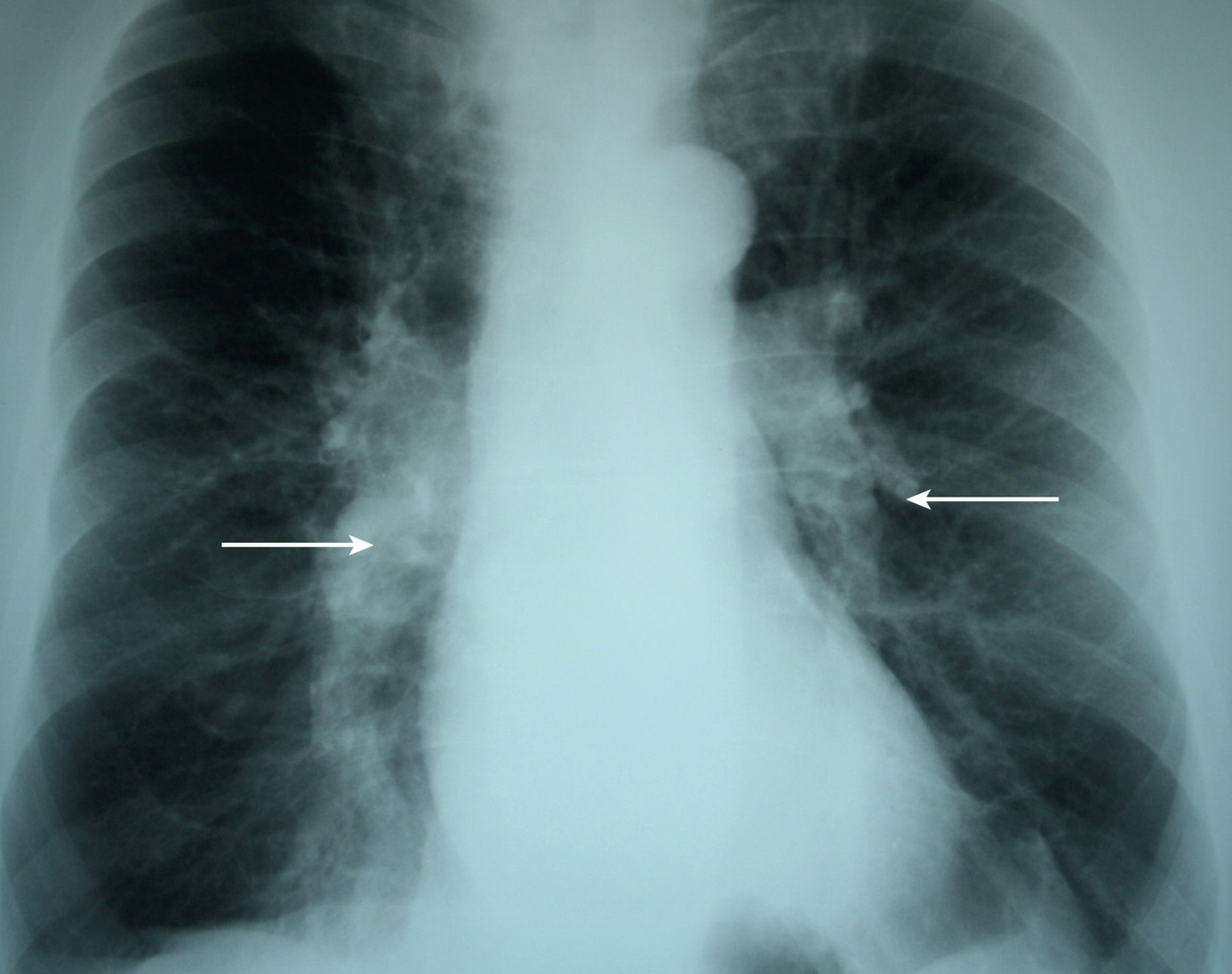
What are you looking for in CXR and CT chest in COPD patients?
CXR: hyperexpansion, increased retrosternal airspace (≥2.5cm), radiolucent bullae (specific for COPD), features of pulmonary HTN (prominent pulmonary arteries)
CT-chest: % of low attenuation area - correlates with severity of the disease
How would you investigate patient with COPD in the outpatient clinic presenting wtih exacerbation?
T: spirometry (irreversible obstruction), PFT (inc TLC, low DLCO), CXR (hyper-expansion, prominent pulmonary vasculature), CT chest (burden of emphysematous disease)
E: exclude infection (CXR, sputum culture), working up for alternative diagnosis - eosinophils (asthma), PE, ECG/Trop/TTE for ischaemia, consider anti-AT-1if FH, malignancy
Severity: PFT (FEV1), ABG (RF,acidosis), inflammatory markers (if infection)
Treatment baseline - spiro, PFT
Screen complications - ECG/TTE (pulmonary HTN), sputum (resistant organisms), bicarb (for TIIRF), polycythaemia, steroid complications, malnutrition (grip strength, BMI, serum albumin)
How would you manage this patient with COPD?
Goal: minimise exacerbation, maximise function, prevent complications
Confirm dx: spirometry (FEV1/FVC <70%, FEV1, check reversibility - is there ACOS), PFT (increased TLC, dec DLCO), CT chest (burden of emphysema)
A: screen secondary causes/exacerbating factors: GORD, infection, anaemia, HF, depression that makes adherence worse. Exclude antitrypsin deficiency.
T: Non-pharm
- Smoking cessation**** (NRT, psychological counselling, encouragement, drugs, e.g. bupropion)
- Educate: prognosis, complications, importance of consistent adherence
- Exercise & reduce weight - improve’s patient’s wellbeing
- Optimise inhaler techniques, maximise adherence - involve family, GP and reminders
- Chest PT, Pursed lip breathing (to provide physiological PEEP), adequate hydration, hand-held fan
- Infection prevention: hand/food hygiene, vaccinations, avoiding contacts
- Modify COPD action plan as per current presentation
- Refer to pulmonary rehabilitation: improves QOL, reduce hospital admissions, depression, fatigue (if not available, PT can do home based exercise)
- LTOT - prolongs life in hypoxic patients (as per criteria), if ≥15h / day
- Home NIV for severe chronic CO2 retention
T: Pharm - As per GOLD guideline, ABx prophylaxis, Consider Bullectomy (localised disease), lung transplant (once FEV1 <25%)
Ensure FU and screen for complications
- Continuous support and encouragement, especially RE: smoking
- Screen & tx osteoporosis, Malnutrition
- Screen for pulmonary HTN (diuretics) and resistant organisms
- Advance Care Planning - discuss EOL issue when FEV1 <25% or BMI <18 → referral to palliative care
What constitutes COPD action plan? (i.e. how would you modify patient’s action plan? - 3)
Breathlessness increases → increase bronchodilator
Breathlessness increases and interferes with ADLs → short course of corticosteroids
Increased sputum production → PO ABx
What are the features of poor prognosis in COPD? (7)
Low BMI
Hypoxia
Hypercapnoea
Recurrent exacerbations
Older age
Pulmonary HTN
Decline in FEV1
Side effects of theophylline? (4)
Oesophageal reflux
Cardiac arrythmia
Nausea
Insomnia
Not very effective
What are indication for supplemental O2 for air-travel in this COPD / chronic lung disease patient?
- SpO2 <92% (at sea level)
- Already on O2 → increase by 1-2L (if >4L cannot go air travel)
- SpO2 ≥ 92% at rest + SpO2 <85% on 6MWT → HAST (Hypoxic Altitude Stimulation Test)
- If HAST positive (i.e. desaturate <85%) → O2
indication for Lung transplant in COPD patient? (4)
FEV1 <25% - End-stage disease
No other significant organ failure / comorbidity
Age <65
Have not had previous thoracic surgery
(1-year survival >80% in this group)
What is your approach to prevent deterioration of COPD (pharmacological)?
Goals: prevent deterioration and manage exacerbation.
Prevent deterioration
- LAMA – tiotropium (glycopyrronium, aclidinium), LABA: salmeterol, eformoterol or VLABA: Indacterol (once daily administration) - review after 6 weeks
- If persistent dyspnoea then combination LABA + LAMA
- Use fixed-dose combi-inhalers to improve adherence to drug therapy
- FLAME trial - Indacaterol–glycopyrronium was more effective than salmeterol–fluticasone in preventing COPD exacerbations in patients with a history of exacerbation during the previous year N Engl J Med 2016; 374:2222-2234
- If FEV1 <50% and >2 exacerbations per year add ICS
- Reduce symptoms, improve quality of life and reduce exacerbations
- But adverse effects are real: pneumonia, easy bruising, cataracts, OP
- If FEV1 < 40% and patient still symptomatic, consider adding low dose theophyline (100mg BD)
- Modest bronchodilator effects
- New data suggesting low dose may have anti-inflammatory and immunomodulatory effects
- Consider long term home oxygen therapy when:
- pO2 < 59mmHg with pulmonary hypertension/RHF
- pO2 < 55mmHg
- Mortality benefit only with ≥ 16 hours/day
- Portable oxygen not shown to have mortality benefit
- Azithromycin
- Shown to reduce exacerbations (Albert et al, NEJM 2011)
- Indicated for use in severe COPD with freq exacerbations
- Does not alter OS
- SEs: Hearing problems, pro-arrythmogenic, Increased colonisation with macrolide resistant organisms
- Manage exacerbations - early recognition and prompt treatment
