Pituitary Gland
- master gland
- attached to hypothalamus via pituitary stalk
- sits in sella turcica
- secretes 8 hormones that regulate organ function
- critical to survival!
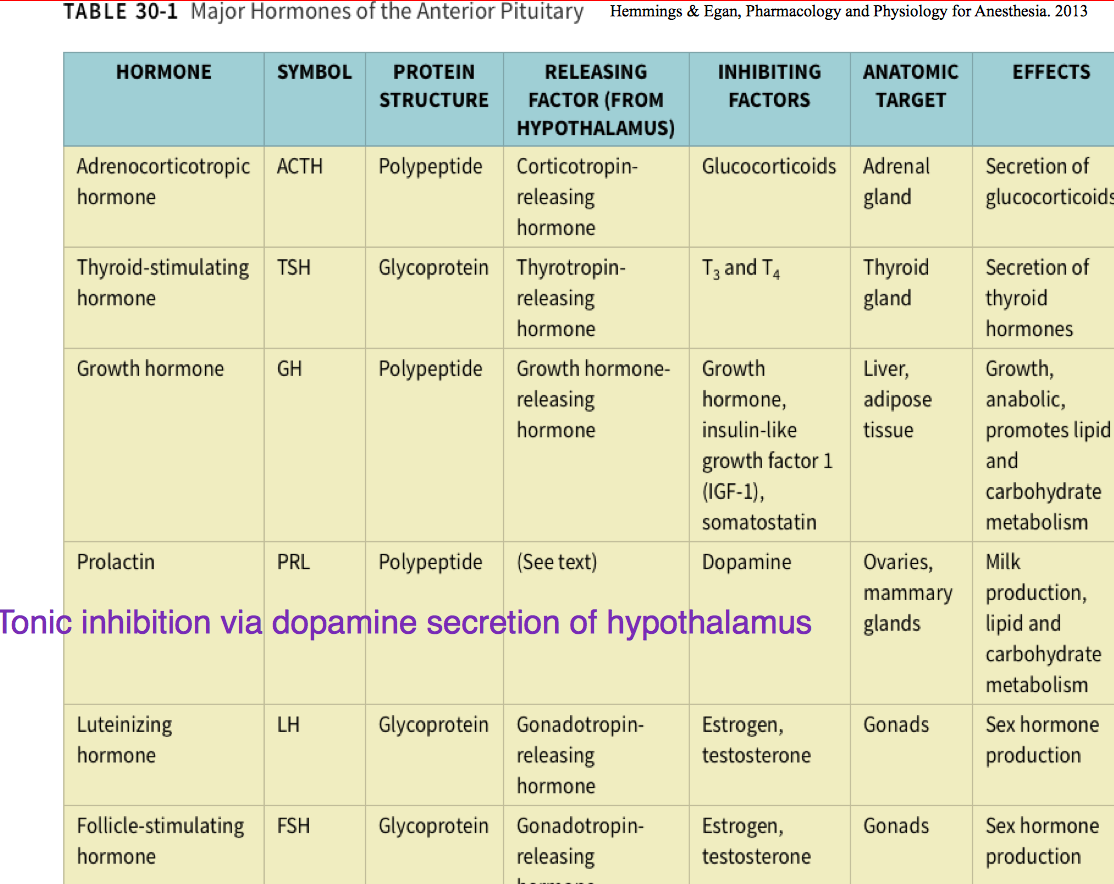
Anterior Pituitary (Adenohypophysis)
- arises from oral ectoderm
- produces ACTH, TSH, GH, PRL, LH, FSH, and MSH
Hyperpituitarism
- 2/2 anterior pituitary adenoma
- often asymptomatic
- presents in 3 distinct ways:
1) hormonal hypersecretion
2) local mass effects (including pituitary hypofunction 2/2 compression of normal gland - visual, sinus, or balance probs) - incidental discovery during imaging
Growth Hormone
- secreted from anterior pituitary in pulsatile manner
- under control of somatostatin and GH releasing hormone
- high in childhood, max in puberty, dec w age
- stimulates longitudinal growth of bones, bone density, condrocyte formation and increases muscle mass
- acts on liver to stimulate gluconeogenesis and promote fat breakdown
Gigantism (childhood) and Acromegaly (adults)
2/2 hypersecretion of GH by ant pit
- leads to increased production of IGH-1 by liver
- gigantism due to growth plates (epiphyses) not closing
- acromegaly inadulthood = cardiac dx, HTN, ventricular hypertrophy
- increased size of soft tissue, mouth, tongue, lips = OSA and upper airway obstruction
Giganitsm and Acromegaly Visual
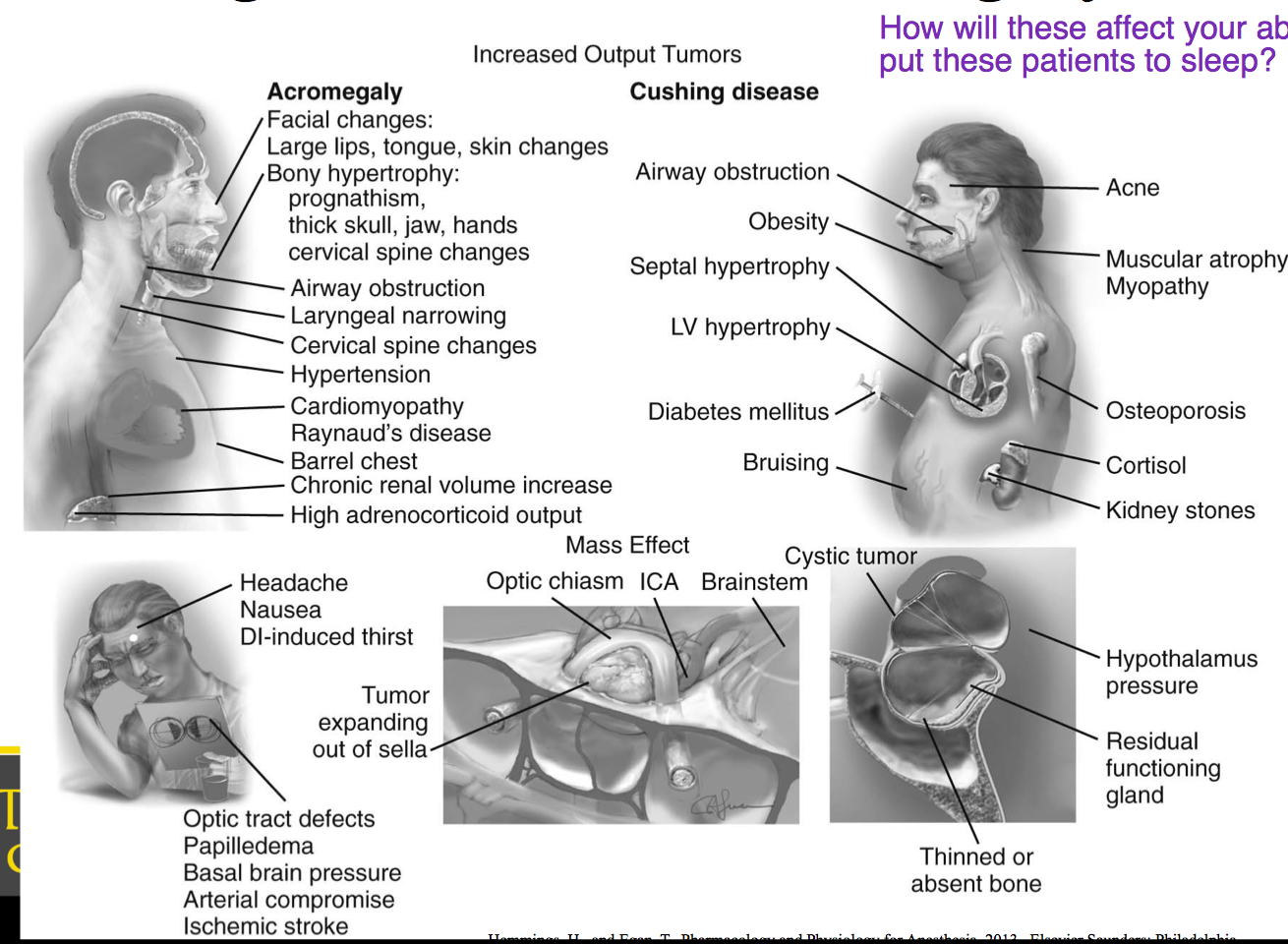
Cushings Disease
- unregulated hypersecretion of ACTH by pituitary adenoma
- hypercortisolism
• Systemic HTN is most common manifestation, secondary to LV hypertrophy
–concentric remodeling of heart
• Glucose intolerance occurs ~~>60% of patients
– Diabetes Mellitus occurs in 1/3 of patients
• Moon Facies
– High incidence of OSA~ Surprisingly despite this there is no association w/ more difficulty w/ intubation. Always be prepared!
Posterior Pituitary (Neurohypophysis)
- Not a secretory gland. A collection of axon terminals – arise from supraoptic and paraventricular nuclei of the hypothalamus
- Principal responsibility is secretion of Oxytocin and Vasopressin (ADH)
- Primary stimulus for ADH secretion = Plasma Osmolarity
– Other factors include
• Left atrial distention, circulating blood volume, exercise, and certain emotional states
ADH
- Controls water secretion and extracellular fluid osmolality
– more potent vasoconstrictor than angiotensin II
Oxytocin
– Promotes milk letdown and uterine smooth
muscle contraction
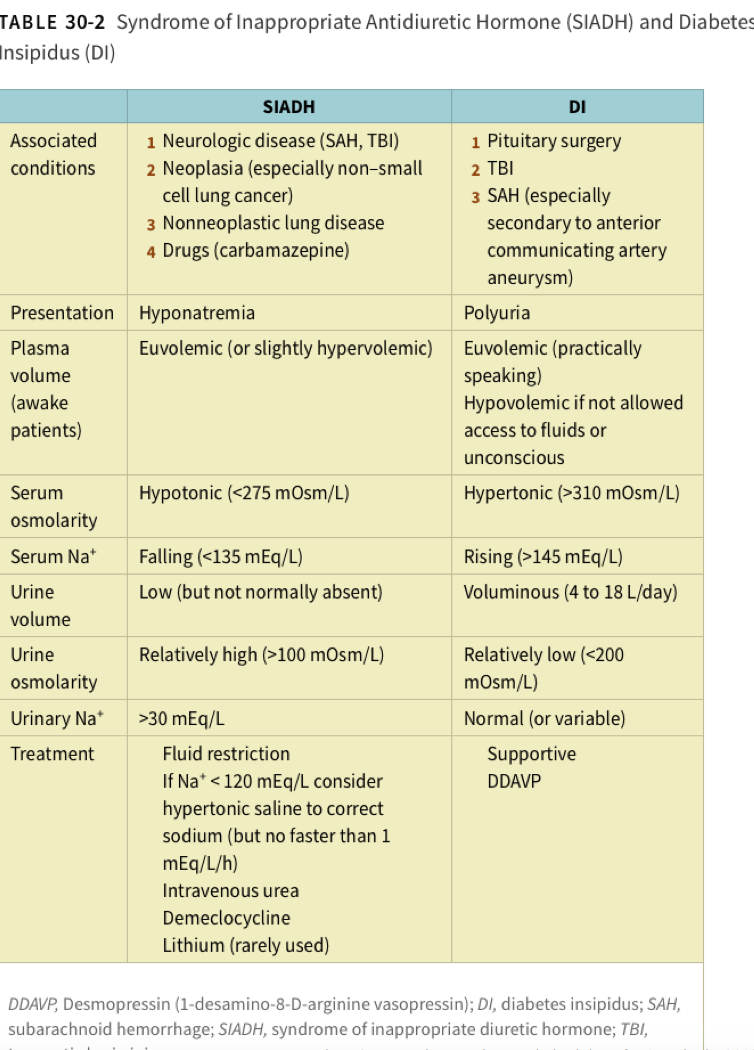
DI
- absence of ADH secretion (commonly associated w pituitary surgery)
- transient
- symptoms: polyuria, thirst, polydipsia
SIADH
- high levels of ADH
- associated w CNS injury, trauma, lung CA
- symptoms: hyponatremia (seizures)
SIADH vs DI Chart
Hormones of the Anterior Pituitary Chart
Vasopressin
- posterior pituitary hormone
- powerful vasoconstrictor
- stimulates g-protein coupled receptors (V1) in VSM
- acts on renal collecting ducts, increasing permeability to water (more concentrated urine) mediated by V2 receptors
- V3 receptors found on anterior pituitary (2nd messenger system, have role in secreting ACTH)
- desmopressin (DDAVP) is synthetic, long acting analogof vasopressin
Oxytocin
- posterior pituitary hormone
- synthesized in supraoptic and paraventricular nuclei of hypothalamus
– Transported down long axons into the posterior pituitary for release
– Physiologic functions of Oxytocin~ Stimulate cervical dilation and uterine contractions during labor
• Allows milk to be let down into the subareolar sinuses during lactation
– Adverse effects = water retention and hyponatremia
• IV admin causes vasodilation and subsequent hypotension w/ reflex tachycardia
Parathyroid Physiology
• 4 small glands (pea sized)
– Located posterior to thyroid gland
– Rich vascular supply
• Inferior thyroid artery
– Chief cells primarily secrete Parathyroid hormone (PTH) in response to hypocalcemia
PTH
- plays chief role in bone remodeling and Calcium homeostasis
– Stims bone resorption which releases Ca into the blood stream
- It also causes Ca reabsorption into the circulation and phosphate excretion via the kidney
- PTH facilitates Vitamin D conversion to its activated form
What is the net result of interactions of PTH, Ca, Vit D and Calcitonin?
- maintenance of normal plasma Ca concentration!
– This helps maintain normal cell function, nerve transmission, membrane stability, bone integrity, coagulation and intracellular signaling
– Normal Calcium levels are 8.5 – 10.5 mg/dl (2.1-2.6 mM)
Primary Hyperparathyroidism
• Primary- Excess PTH production
– Most often d/t parathyroid gland hyperplasia or tumor
• This increases bone resorption and extracellular Ca
– Clinical Signs = Hypercalcemia, hypophosphatemia, nephroliathisis, osteoporosis, fatigue, weakness, and difficulties w/ cognition
• Treatment- Surgical excision of the parathyroid glands or tumor
Secondary Hyperparathyroidism
Generally a complication of chronic renal failure, but can be d/t any disease causing hypocalcemia
Anesthetic Considerations
• Thorough preop eval to focus on effects of hypercalcemia and the degree of cardiovascular and / or renal complications
– pre-op EKG
- Show shortened PR and QT intervals (avoid zofran)
- Potential for cardiac arrhythmias
- Pts may be hypertensive and hypovolemic (severe hypercalcemia)
– Focus should be on emergence in terms of potential concerns
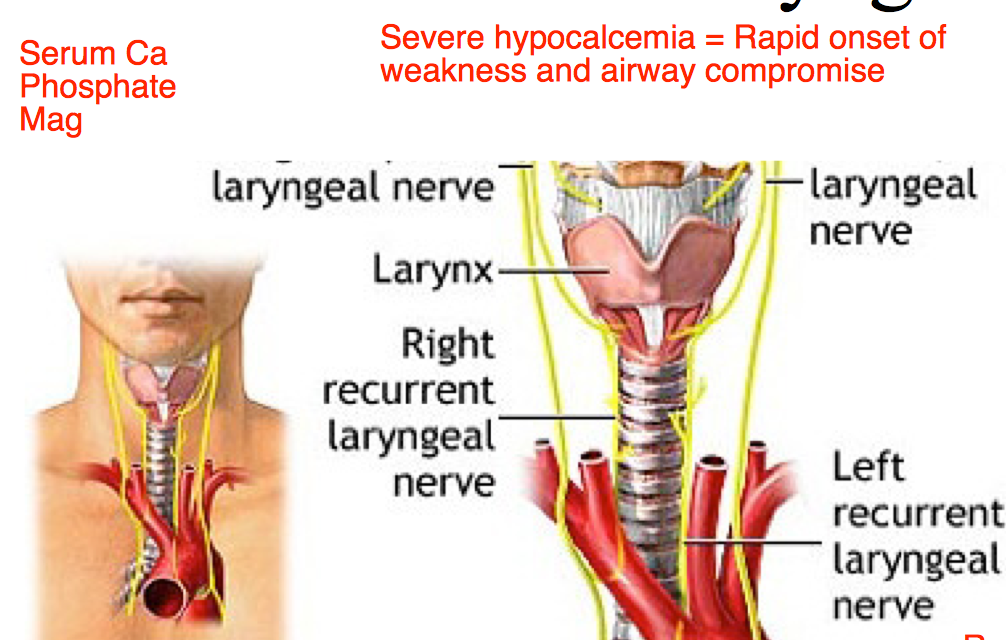
• Surgery on thyroid or parathyroid glands can result in damage to recurrent laryngeal nerve, airway swelling and hematoma formation
– Can lead to devastating consequences!
Recurrent Laryngeal Nerve
- Sensory innervation below true cords and into upper trachea
- Motor innervation to all intrinsic laryngeal muscles except cricothyroid and external branch of superior laryngeal nerve
Innervates ALL muscles of larynx except crycothyroid which is external laryngeal nerve.
If paralyzed, VC will be abducted causing strider and hoarseness.
If partially paralyzed, adducted, causing obstruction and lesion, possible aspiration risk
Recurrent Laryngeal Nerve Injury
• Can occur with intubation, neck surgery, stretching of neck
– Thyroid or cervical spine surgery
• Unilateral vs Bilateral
– Unilateral causes cord on injured side to assume midline position= hoarseness – Bilateral causes both cords to close to midline (adducted) position = aphonia and airway obstruction occurs **** • Airway emergency





