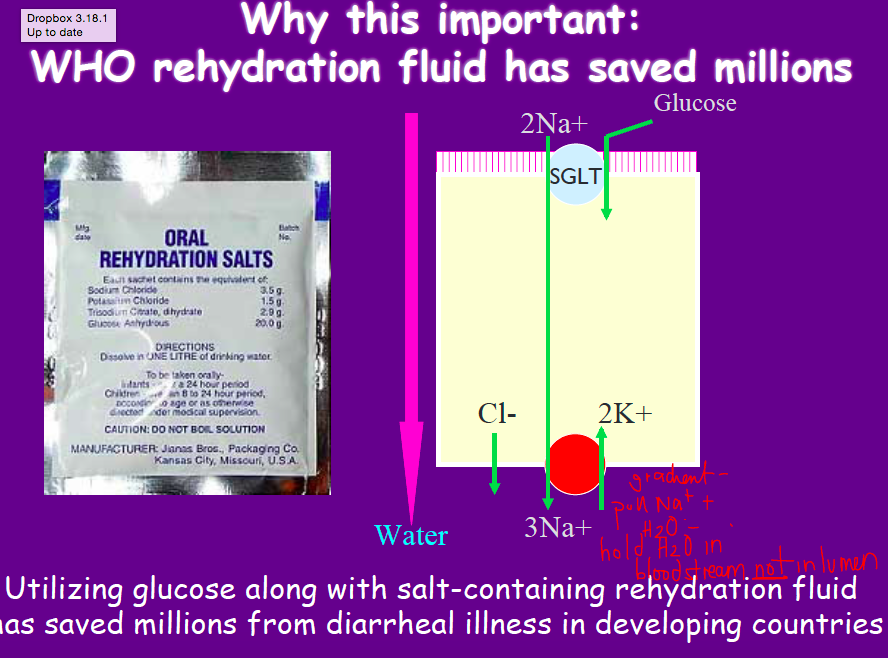
WHO rehydration fluid
SGLUT!
use glucose with salt - take up Na better
cellulose digestion
So what ends up happening is that in your diet you have a whole bunch of indigestible carbohydrates. In particular cellulose. Cellulose your body actually has no native mechanism to break down into its constituent monosaccharides. There is a whole range. When you eat a green banana you can’t digest 75% of whatever you’re eating. Whereas in white rice you can digest a lot of it.
Now when cellulose is passed through your GI tract it’s not digested but when it gets to the colon the bacteria within your colon can actually digest it and break down the cellulose into not really monosaccharides but short chain fatty acids.
Short chain fatty acids are actually an energy source that your body can use. Cellulose it can’t use but it’s broken down into short chain fatty acids which it can use.
And in fact when you look at the cellulose products, butyrate, which is one of the short chain fatty acids produced is actually the primary energy source for the colonocytes.
In fact they almost get none of their energy from any blood supply.
PAT1
classic amino acid transporter on brush border
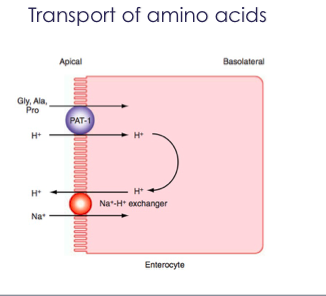
Again here this is just a picture that demonstrates that.
So PAT1 looks at things like glycine, alanine and proline.
So these are the smaller amino acids which symport with hydrogen.
Ach receptor?
m3 - on parietal cells
absorption of peptides
di and tri peptides appear to use the same transporter Pept 1
in the small bowel only!
only expressed on absorptive epithelium and driven by H+
parasympathetic of GI
excitatory
cholinergic
vagus nerve controls motor function of upper gi tract
saccral nerves control distal colon and rectum
fewer neurons to small intestine
Severe Combined immunodeficiency
stem cell defects in lymphoid maturation
effects seen in infancy and patients usually die young
malabsorption and diarrhea
microtubules
composed of tubulin
imp for structural support
directs vesicles through cell
maintain polarity of polarized epithelia
3 functions of CCK
- 3 functions
1. Increases secretion of pancreatic enzymes
2. Relaxes sphincter of Oddi
3. Conctracts gallbladder à bolus of concentrated bile à goes down the biliary tree à into the intestinal lumen!
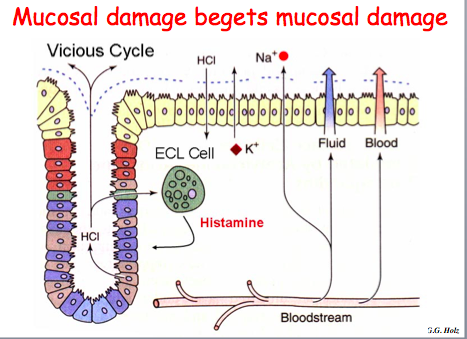
NSAIDs and mucosal damage
Now,clearly if you damage this mucous layer, it’s a problem. there are a number of things that can actually reverse this process. One of the most important is prostaglandin inhibitors PGI, and the PGI that you guys know best are NSAIDs. Asprin, Ibuprofen, those sort of things. And what those do is they inhibit prostaglandins. One of the effects is you produce less mucous. And now the HCl doesn’t necessarily just sit on top of a mucous layer, it actually can sit up against the surface of these epithelial cells and damage them. It can cross the mucosa into the lamina propria, where it starts hitting cells such as the ECL cells—and remember, I said that the ECL cells produce histamine, and we’ll discuss that a little bit more, but histamine is one of the primary secretagogues of acid secretion. So you set up a vicious cycle whereby HCl is allowed access to the epithelial cells; it can trigger a lot more acid production; you can damage this mucosa greatly, and actually develop peptic ulcers.
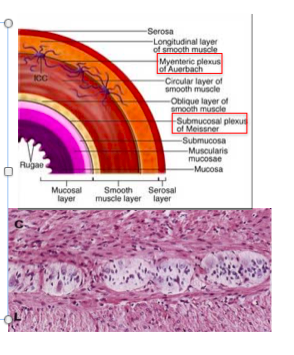
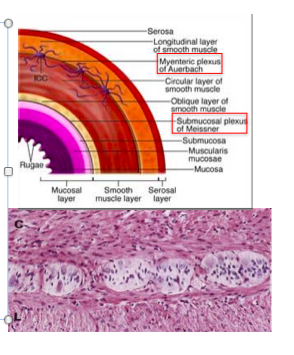
Auerbach’s plexus
•Between the internal and external muscle layers of the muscularis propria is the myenteric (Auerbach’s) plexus
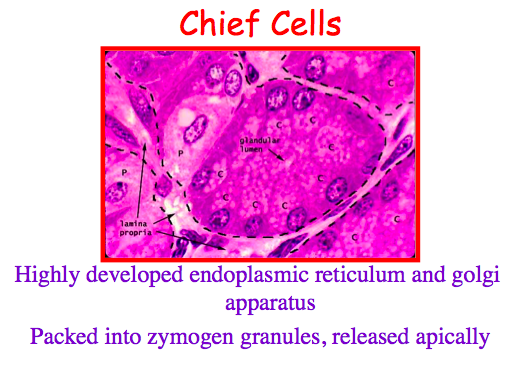
chief cells
make pepsinogen
highly developed ER and golgi
packed into zymogen granules and released apically
Chief cellà Pepsinogenà Pepsinà breakdown proteins.
Let’s now turn a little bit to the enzymatic secretion, and the cell we’re concerned about here is the chief cell. So as you’ll recall, the chief cell is present throughout the oxyntic mucosa, as well as being present in the antral mucosa to a minor degree. And this is a gastric gland. And this little tiny white area here in the middle is actually the lumen. And unlike the G cells, all these granules containing pepsinogen are all present at the apical surface of the cell. So here you can tell that these cells are producing the substances that are going to be released out into the lumen, not into the bloodstream. These cells are have very highly-developed endoplasmic reticulum and golgi apparatus, because they’re spending a lot of time producing these enzymes, which are proteins.
So, what they release is pepsinogen. And whenever you hear something “-ogen,” like trypsinogen, chymotrypinogen, you know that you’re dealing with a pro-enzyme. So, like those pancreatic enzymes we discussed yesterday, pepsinogen is produced as a proenzyme—it’s not released in the active form, it has to be activated in the lumen of the digestive tractform, needs to be activated.
Ie why zymogen is released in packets. You don’t want it to be activated inside the cell and it will cause self digestion of the cell. Being in packet prevents activation inside the cell.
H2 receptor
histimine receptor on parietal cells
(H1 is allergy)
Vitamin K
utilized in liver to catalyze post-trnaslational modifications of blood clotting factors
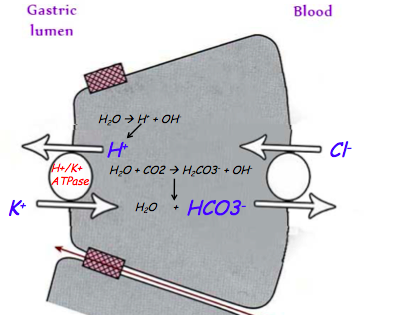
parietal cell - how secretes H+?
- Na/K creates gradient
- decreased Na in cell causes Na to enter the cell and huge decrease in Na in the lumen!
- Na electrochem gradient causes Cl to enter lumen
- Now, as Cl is pumping out into the lumen, it’s also coming in basolaterally through an anti-porter in exchange for bicarb. So you’ve got Cl coming in at this moment as well, and it’s getting replaced with HCO3. So this is an electroneutral process, right(Both Cl and HCO3 are negative). You haven’t changed the neutrality of the cell. But what you’ve done is you’ve pumped out HCO3, rendering this cell more acidemic, or more of an acid pH, because you lost HCO3, an alkaline agent, out basolaterally. This makes the cell more acidic, allowing you to then pump out the H+ ions that were liberated when you broke down carbonic acid into HCO3 and H+(Inside the cell using Carbonic anhydrase). The pump that does it is the H/K-ATPase. This is the 2nd important pump you have to remember, 1st was Na/K ATPase. you’re pumping all of this acid out, all of these protons out against a very steep gradient, so you still need a lot of ATP to do it. So you use the H/K-ATPase. Out of all the pumps and channels that you just heard about, this is the one to remember, because this is the most important pump in the parietal cell. This is the one that plays the major role in pumping out acid. So DO remember that. So Cl is exchange for the HCO3- and then Cl and H+ are pumped out into the lumen.
L cells
GLP-1
inhibits acid secretion
stimulant of pepsinogen secretion
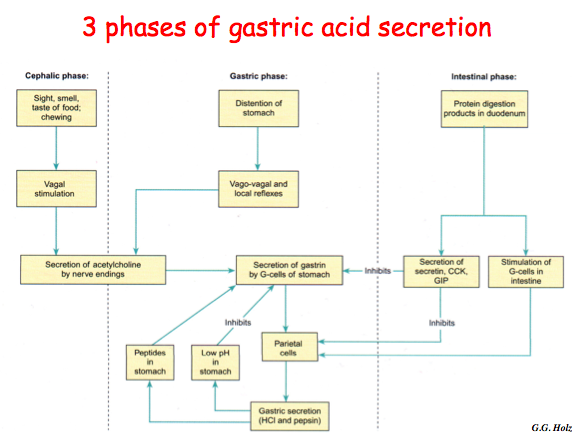
acetylcholine!!
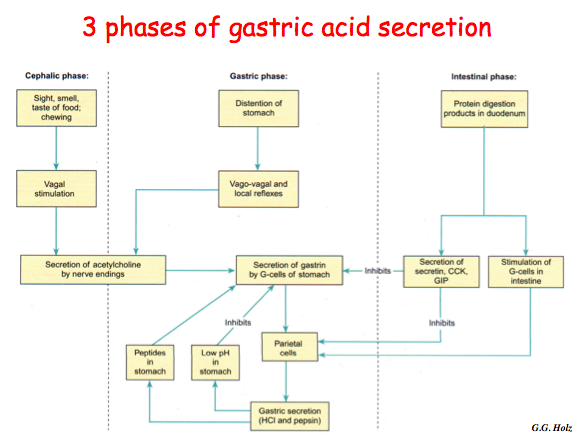
cephalic and gastric phase
acid triggers a local cholinergic effect
gastrin and CCK may also help
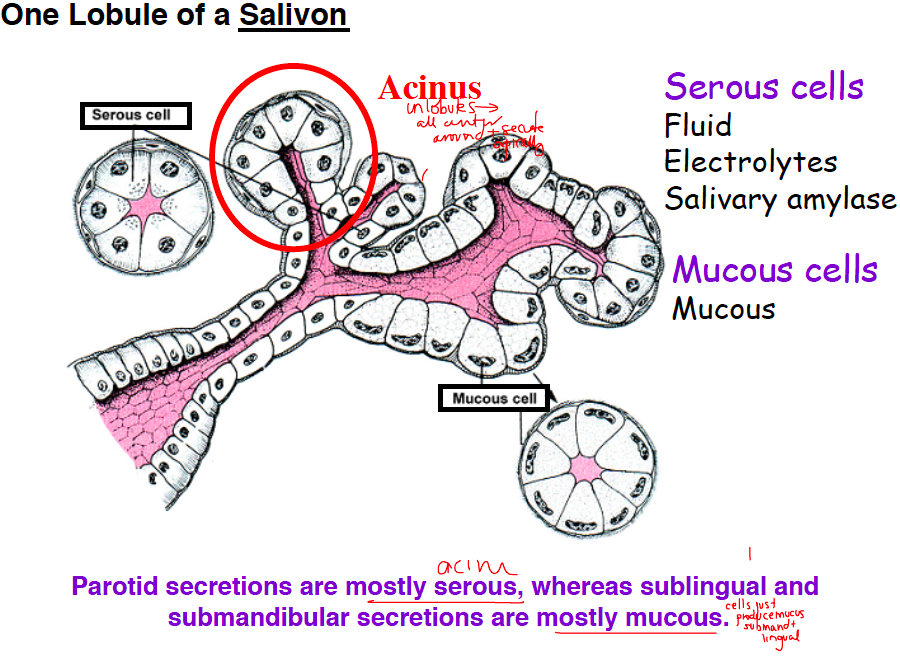
functions of saliva
digestive (starch, taste)
protective (lubricate, buffer, clean)
immuno (IgA and other proteins)
intestnial phase of gastric acid secretion
- protein digestion products in duodenum
- secretion of secretin/CCK/GIP
- inhibits parietal cells
turns off
parotid vs sublingual/submandibular secretions
parotid = mostly serous (acini)
sublingual/mand = mostly mucous
meissner’s plexus
•Below the muscularis mucosae is the submucosal (Meissner’s) plexus
–Relays information to and from the epithelia
- Meissners plexus = immediately under submucosa
- Role is to take information from lumen and send it to brain to affect function of epithelium
gastric phase of gastric acid secretion
- distention of stomach
- vasovagal reflexes
- secretion of Ach by nerve endings
- secretion of gastrin by g cells
- parietal cells
- gastric secretion
fat pancreatic enzymes
lipase, PLA2, choleteral esterase
breaks TGs and PPLs into 2 monoglycerides and fatty acids
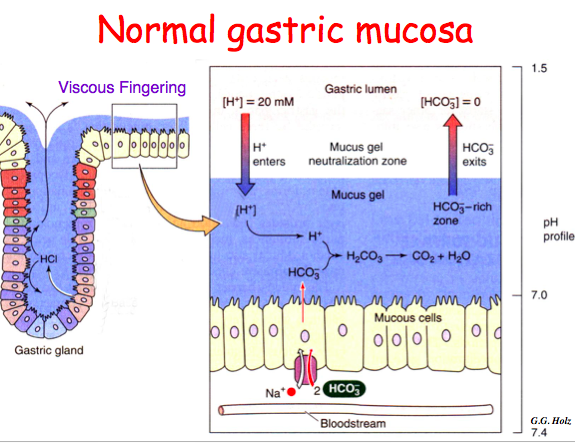
viscous fingering
movt of acid through the mucos layer), where it just sort of chews its way through the mucous and reaches and sits on top (exact mechanism is unknown but very important that it happens as these surface cells are as prone to acid damage as any other cells in the body).