What is induction of labour (IOL)?
to instigate labour artificially - 3 main stages
1) using medications and/or devices to “ripen cervix”
2) this is followed usually by artificial rupture of membranes (performing an amniotomy)
3) then, synthetic oxytocin can be used to initiate contractions and bring about labour
How often is labour induced?
Approx 1 in 5 pregnancies
Is induction of labour risky business?
It is indeed
Thats why in induced labour, there is always fetal monitoring
For IOL, a key part is ripening the cervix
How can this be done?
Prostaglandins pessary (vaginal)
Balloon
What is the Bishop’s score?
A clinical score used to guide us on when to do an amniotomy (break the waters)
The higher the score - the more progressive the change in the cervix and the more likely induction is to be successful
What are the criteria for bishops score?
What score is considered fdavourable for amniotomy?
Dilation
Effacement (length of cervix)
Position
Consistency
Station (no clue)
A SCORE OF 7 is favourable
Once an amniotomy has been performed - what is the next step?
IV oxytocin can be given to achieve adequate contractions (unless contractions start spontaneously)
The aim is 4/5 contractions every 10 mins
Why do we induce labour? (ie what are the indications)
Diabetes
If term +7 days
Maternal need for planning of delivery - eg if on anticoagulants
Fetal reasons - growth concerns, oligohydramnios
Social/maternal request
When talking about intra-partum complications during induced labour - they can be categorised as being under:
The powers
The passage
The passenger
What complications fall under these?
The powers:
- inadequate uterine activity
- hyperstimulation of uterus
The passage:
- Cephalopelvic disproportion (CPD)
- other obstructions - eg fibroids
The passanger:
- Malposition
- Malpresentation
- fetal distress
How is progress in labour evaluated?
COmbination of abdominal and vaginal examinations to assess:
Cervical effacement
Cervical dilatation
Descent of fetal head thru pelvis
On examination, what features would suggest sub-optimal labour progress in the active first stage?
In the active first stage of labour - sub-optimal progress is defined as:
- < 0.5cm per hour in primigravid women
- < 1cm per hour for parous women
How is inedequate uterine activity dealt with?
IV oxytocin can be used to increase the strength and duration of contractions
However, before this is given - it is important to exclude an obstructed labour
What is cephalopelvic disproportion?
This is when the fetal head is too large to negotiate through the maternal pelvis and be born - even when in the correct fetal position
Genuine CPD is quite rare
What are the signs of CPD?
Caput - which is swelling at the top of the babies head
Moulding - when the cranial sutures of the baby overlap
What are other forms of obstruction, other than CPD?
Placenta praevia - placenta covering cervix
Fetal anomalies - eg hydrocephalus
Fibroids
Describe what malposition is?
When the fetal head is in a suboptimal position for labour and a relative CPD occurs
Much more common than malpresentation
Normal position - Occipito-anterior
Malposition - Occipito-transverse, occipito-posterior
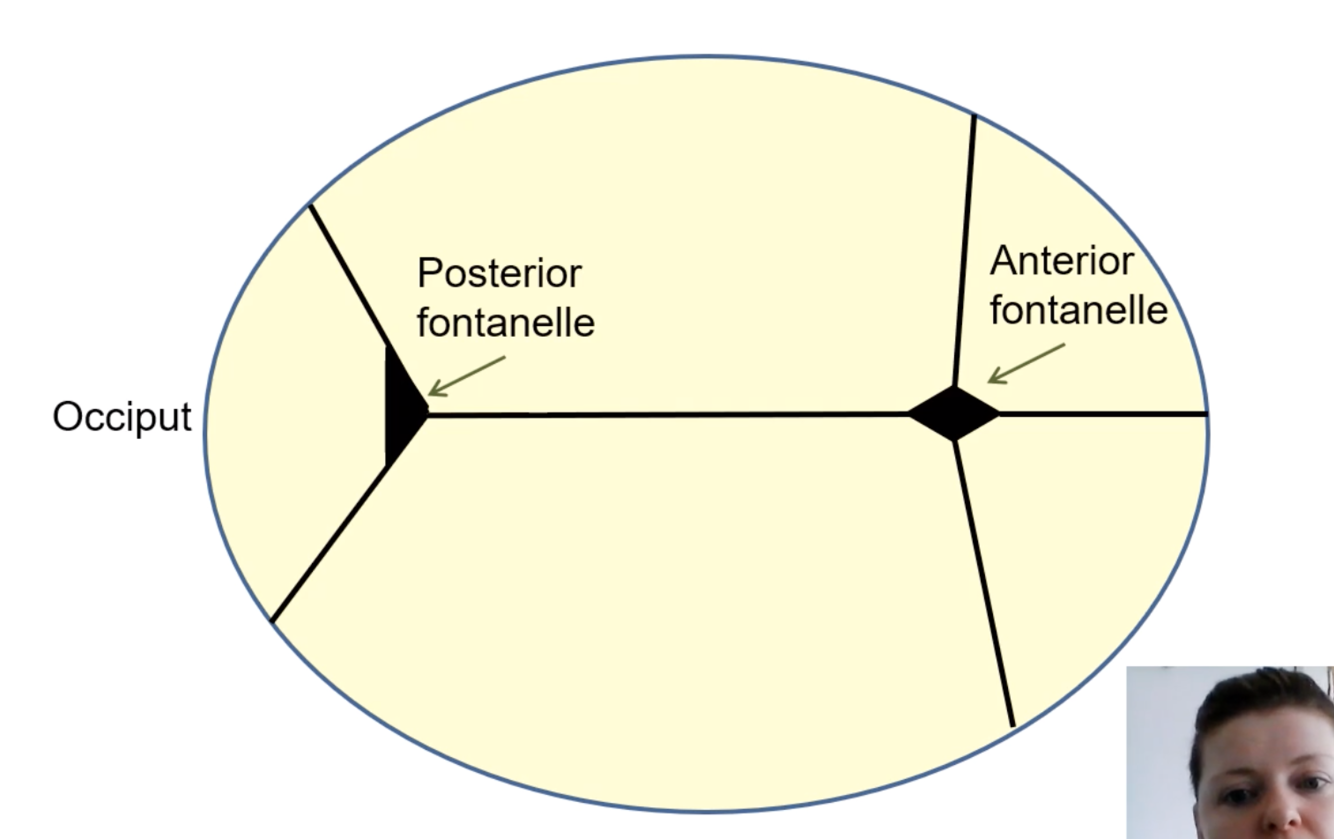
How is the position of the baby (way it faces) felt to determine if malposition?
Using the fontanelles of the fetal skull
Anterior fontanelle - diamond shaped
Posterior fontanelle - triangular
By feeling these we can determine which position the baby is facing
What are the main causes of fetal distress
Hypoxia
Infection
Cord prolapse
Placental abruption
Vasa praevia
Uterine hyper-stimulation (causes hypoxia)
Often no cause
How is fetal monitoring done?
Low risk:
- Intermittent auscultation of fetal heart
- HHD or pinard’s stethoscope
High risk (incl induced labour, meconium, diabetes etc):
- Cardiotocography (CTG)
Fetal distress:
- Fetal blood sampling
- Fetal ECG
When is fetal blood sampling done and why is it useful?
Speculum used to take fetal blood sample from scalp. Cervix must be at least 4cm dilated
Can give us:
- pH & base excess
- lactic acid
- pH gives measure of likely hypoxaemia
Used when abnormal CTG/worry of fetal distress
What are the types of operative deliveries?
Instrumental:
- Forceps / Ventouse
- 15% of deliveries
Elective (planned) C section:
- C section performed before labour
- 20-30%
Emergency C section:
- 20-25%
What are the 3rd stage complications of giving birth?
(3rd stage = birth –> delivery of placenta)
Retained placenta
Post partum haemorrhage:
- 4 Ts - Tone, trauma, tissue, thrombin
Tears:
- Graze
- 1st
- 2nd
- 3rd degree - involving anal sphincter complex
- 4th degree - involving rectal mucosa
-
Male basic Physiology (BJ)17
-
Male basic Physiology 2 (BJ)14
-
Female reproductive physiology16
-
Embryology - male24
-
Embryology - female20
-
Antenatal Care (bj)35
-
Pharmacology in preggo25
-
Physiology in Pregnancy31
-
Sexual helf - Genital symptoms17
-
Sekshuwal helf - STIs11
-
Normal labour18
-
Less normal labour23
-
Obstetric emergencies14
-
Common pathologies of pregnancy15
-
Common genital syndromes (non-STI)25
-
Maternal and perinatal mortality21
-
Complications of pregnancy 139
-
Complications of pregnancy 2 (preeclampsia)18
-
Complications of pregnancy 2 (management of PET)10
-
Complications of pregnancy 2 (other stuff)15
-
Infertility 1 & 2 (Pphysiology and diagnosis)25
-
Infertility 3 (management)15
-
Menstrual disorders (unfinished)21
-
Menstrual Disorders (copy)26
-
Menstrual Disorders - Dysfunctional Uterine Bleeding16
-
Contraception33
-
Pharmacology29
-
Pelvic Organ Prolapse9
-
Female Urinary Incontinence13
-
Genetics13
-
Menopause24
-
Secondary Amenorrhoea5
-
Cervical Screening22
-
FGM15
-
Ovarian Cancer18
-
Endometrial Cancer16
-
Vulval Cancer16
-
Breast Anatomy23
-
Breast Radiology & Cytology12
-
Breast Pathology24
