Discuss some key aspects of a good MSK history
- Assess severity of symptoms
- What’s impact on every day life?
- If injured, what was mechanism?
- Distinguish inflammatory vs non-inflammatory causes of joint pain (e.g. when is stiffness)
- Identify mechanical symptoms
- Identify any red flags
- Identify potentially significant problems e.g. cancer, psoriasis, gout etc…
- Identify FH of any MSK conditions
- Identify occupation triggers e.g. repetitive movements, lifting, posture etc..
- ICE
… and of course usual questions such as timing, aggrevating factors, relieving factors etc…
State some MSK pathologies that require urgent admission to A&E
- Cauda equina syndrome
- Metastatic spinal cord compression
- Spinal infection
- Septic arthritis
State some MSK pathologies that require urgent referral to appropriate specialists
- Primary or secondary cancers
- Insufficiency fracture
- Major spinal relaed neurologial defiit
- Cervical spondylotic myelopathy (CSM)
- Myositis (refer urgently to rheumatology)
- Giant cell arteritis (urgent referral to rheumatologist on same day if possible, if not in 3 working days. Commence steroid therapy if have to wait)
State some red flags of cauda equina syndrome
- Bilateral sciatica
- Perianal numbness
- Bowel or bladder dysfunction
- Uni- or bi-lateral lower limb motor and/or sensory abnormality
- Erectile dysfunction
Remind yourself:
- What cauda equina syndrome is
- Why it is an emergency
- Cauda equina is compressed
- Complications if untreated:
- Paralysis
- Sensory abnormalities
- Bladder and bowel dysfunction
- Sexual dysfunction
What can you give to patients who are at risk of cauda equina syndrome?
CES cards (highlights symptoms that pt should be concerned about and advises them when to seek medical attention)
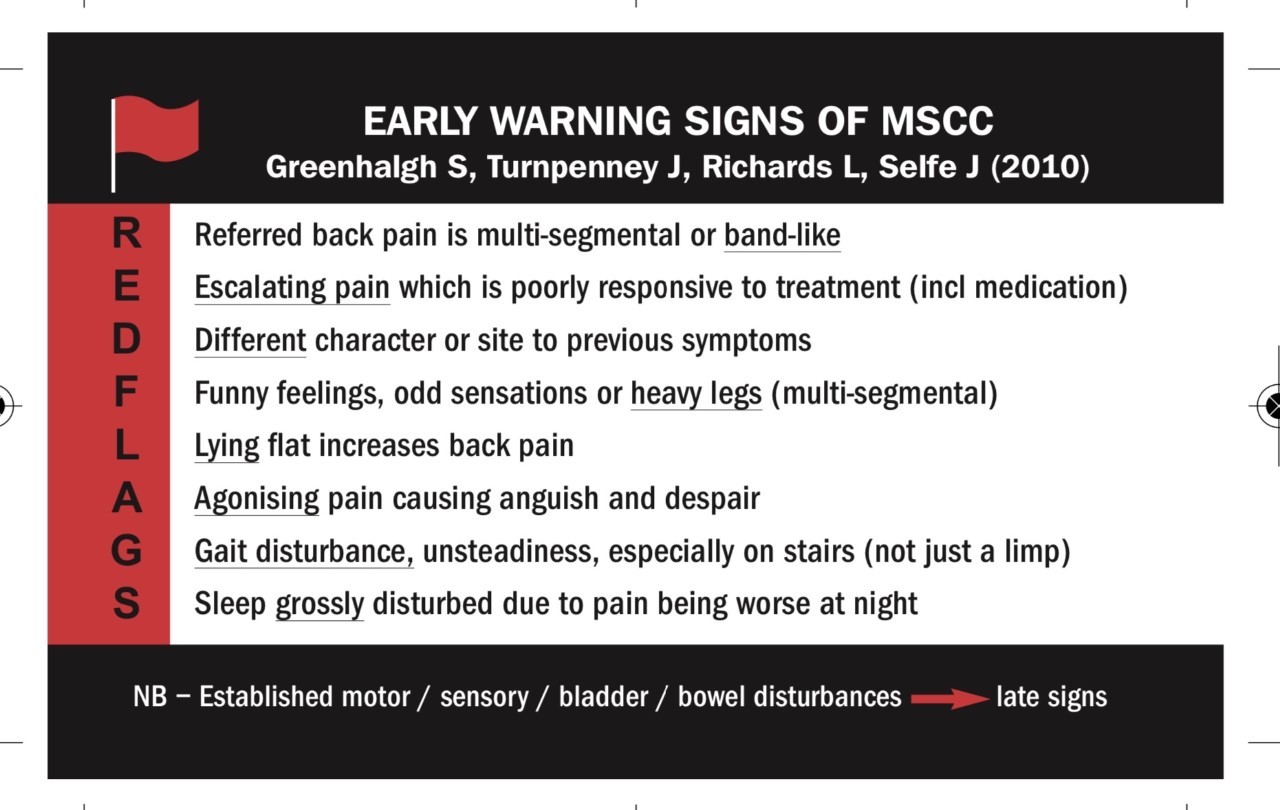
State some red flags of metastatic spinal cord compression
- Spine pain with band like referral
- Escalating pain
- Gait disturbance (not just a limp, unsteadiness that is even worse on stairs)
- Pain worse on lying flat
- Sleep disturbance due to pain
- Funny feelings/odd sensations or heavy legs
- Past medical history of cancer
State some red flags of a spinal infection?
- Spinal pain
- Fever
- Worsening neurological symptoms
- Risk factors e.g. immunosupression, primary soure of infection, personal or family history of TB
State some red flags of septic arthritis
- Sudden onset of a hot, swollen joint
- Multidirectional restriction in movement
- Fever
*NOTE: septic arthritis may present as painful limp or loss of function in upper limb- don’t necessarily have hot swollen joint
State some red flags of primary or secondary cancers affecting the MSK system
- History of cancer (breast, prostrate, lung, kidney, thyroid are most likely to metastasise to bone)
- Escalating pain
- Night pain
State some red flags of an insufficiency fracture of the spine
- Sudden onset of pain (usually in thoraco-lumbar region)
- Pain varies (usually severe and localised to area of fracture)
- History of low impact trauma
- Risk factors e.g. osteoporosis
What is a stress fracture?
Insufficiency fractures are a type of stress fracture (fracture caused by repeated stress over time) in abnormal bone e.g. weakened bone due to osteoporosis.
State some red flags/criteria for major spinal related neurological deficit
- Spinal pain
- Associated limb symptoms (e.g. new onset or progressively worsening limb weakness present for days/weeks)
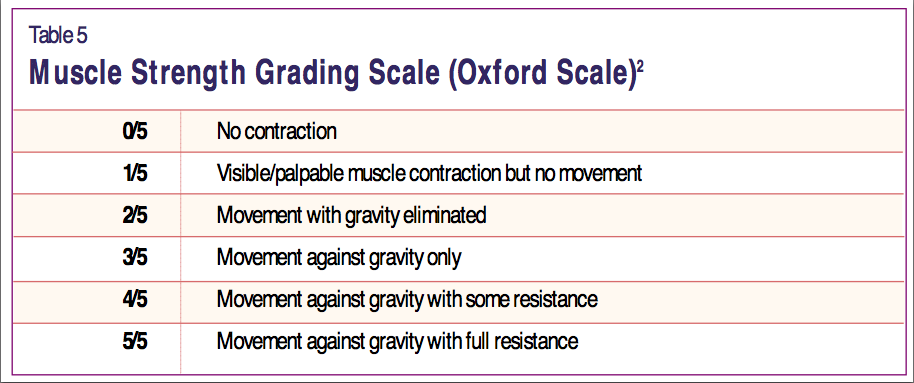
- Less than grade 4 on Oxford muscle grading system and associated with >1 myotome
What is the Oxford Scale for muscle grading?
Quick method of assessing and grading muscle power. Scale is from 0-5 (note: may see +/- signs to indicate more or less power but not enough of a change to alter the number).
State some red flags for cervical spondylotic myelopathy (CSM)
- History of cervical spondylosis
- Pain getting worse
- Lack of coordiation
- Heaviness or weakness in arms
- Pins & needles in arms
- Problems walking
- Loss of bladder or bowel control
You should consider serious pathology as a differential diagnosis when a patient presents with any of what 3 criteria?
- Escalating pain & progressively worsening symptoms that do not respond to conservative management or medication as expected
- Systemically unwell (e.g. fever, weight loss)
- Night pain that prevents sleep due to escalating pain and/or difficulty lying flat
State some situations in which you would refer a patient to rheumatology
Wouldnt’ learn whole list; idea that anyone with a rheumatological condition that needs long term managment e.g. RA, psoriatic arthritis, autoimmune, spondyloarthritis, GCA (although this is urgent referral)
- Suspected rheumatoid or psoriatic arthritis: persistent synovitis (i.e. hot, swollen joints), early morning stiffness >30 mins, +/- increased CRP/ESR, +/- RF/anti-CCP
- Suspected new onset of autoimmune connective tissue disease
- Myalgia not secondary to viral infection or fibromyaglia that is worse proximally, worse in morning, >30 mins stiffness… could have polymyalgia rheumatica or myositis
- Temporal arteritis
- Suspected spondyloarthritis
What are the likely causes of limited or painful active movement but full, pain-free passive movement?
If active movement is painful or limited but passive movement is pain-free and has full range of motion this would suggest pathology is with the mechanisms that produce injury e.g. muscles, nerves. If there is e.g. a foreign object in joint obstructing movement, movement would be reduced and painful on both active and passive movement.
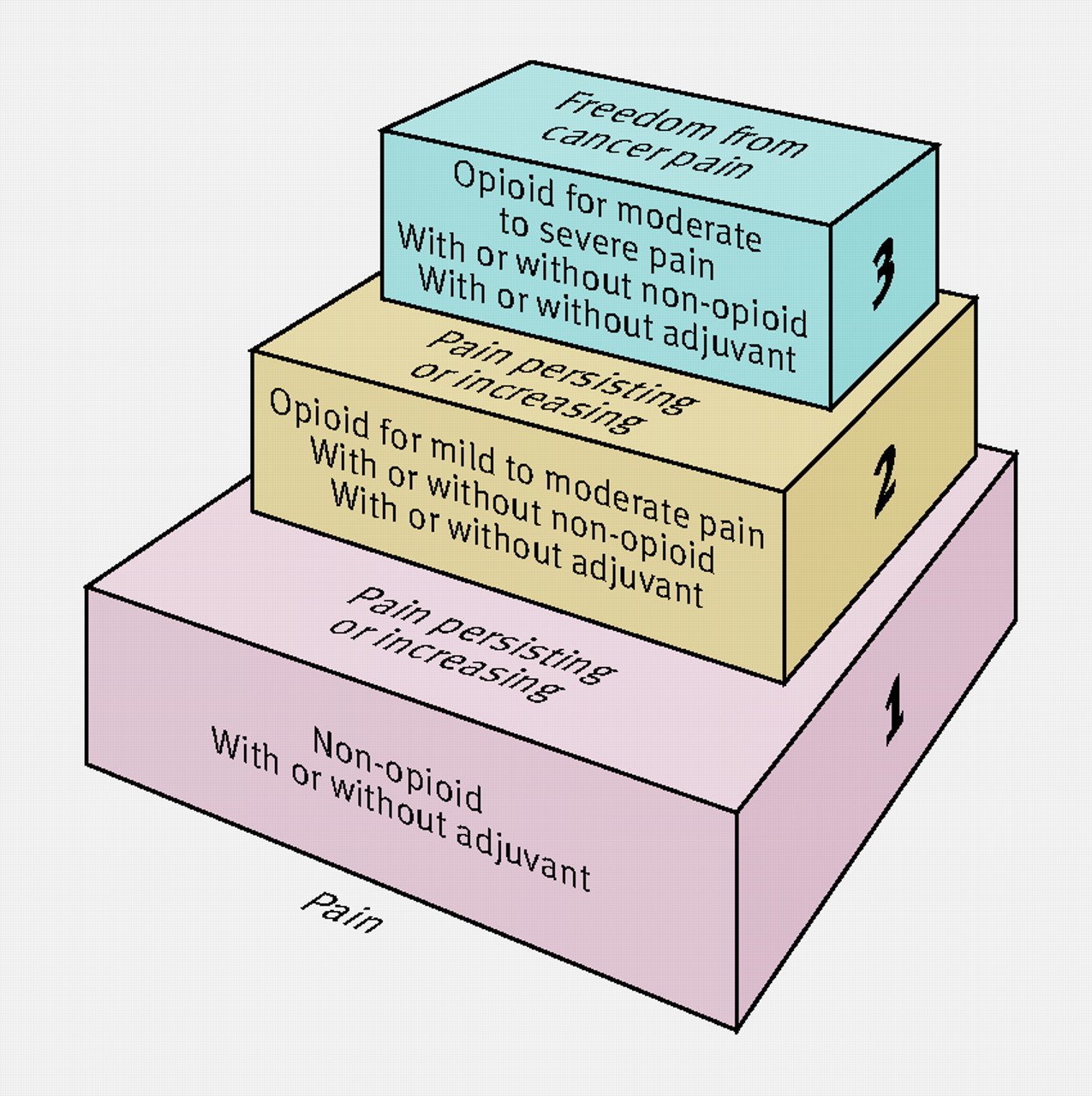
Describe the WHO pain ladder
The three main principles of the WHO analgesic ladder are: “By the clock, by the mouth, by the ladder”
Define stiffness
Inability to move with ease and without pain
Discuss the use of the WHO analgesic ladder in chronic MSK pain
If opiods are used for chronic pain, patient can become both tolerant and dependent on the opioids; opioids then no longer help the pain but the pt is addicted
What are mechanical symptoms of knee?
What have they traditionally ben thought to represent and is there evidence to contradict this view?
- Mechanical symptoms inlcude locking (inability to bend or straighten knee), catching, popping and feeling of ‘giving way’ in knee
- Traditionally they were thought to represent meniscal tears however recent studies show that mechanical knee symptoms are equally as common among patients with and without meniscal tears.
Remind yourself of the bursa in the knee (6)
**Suprapatellar bursa is extension of synovial cavity
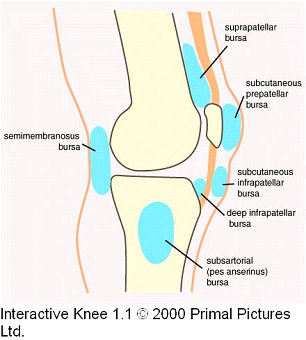
Which bursa of the knee are most commonly inflamed?
- Suprapetallar: extension of synovial cavity therefore suprapatellar bursitis is not a sign of localised irritation but a sign of a knee effusion which indicates knee pathology. Causes include: RA, OA, infection, gout, repetitive microtrauma
- Pre-patellar: “housemaids knee” history of repeitive trauma (usually) or blunt trauma
- Infra-patellar: “clergyman’s knee” caused by repetitive trauma in more upright position than housemaids knee
- Semi-membranous bursa: attached to posterior capsule of knee and may communicate with knee joint via small opening; therefore in a knee effusion you may get swelling of this bursa- presents as Baker’s/popliteal cyst
- Pes anserinus/subsartorial:



-
Remote Consulting9
-
Acute Emergencies & Pre-hospital Care61
-
Safeguarding26
-
MSK47
-
Paediatrics96
-
Minor Illness36
-
Health Promotion54
-
Men's & Women's Health76
-
Dermatology123
-
ENT79
-
Contraception & Sexual Health93
-
Mental Health81
-
Diabetes61
-
Hypertension, CKD & Hyperlipidaemia76
-
Asthma & COPD76
-
IHD & Heart Failure54
-
Palliative Care25
-
Medicines Optimisation16
-
ENT 261
-
STIs42
-
Scoring Systems & Emergency Drugs52
