Describe the pathophysiology, presentation and management of renovascular disease
Progressive narrowing of the renal arteries with atheroma causes reduced perfusion. GFR falls but tissue oxygenation of the cortex and medulla is maintained
Progression of RA stenosis to 70% causes cortical hypoxia and microvascular damage and activation of inflammatory and oxidative pathways.
Parenchymal inflammation and fibrosis progress and become irreversible and at this point, restoration of blood flow has no benefit
Presents with hypertension, pulmonary oedema, bruits, hx of vascular disease
Manage with BP control (not ACEi/ARB), statins, good glycaemic control if diabetic, smoking cessation, exercise, low sodium diet
Angioplasty only used if rapidly deteriorating renal failure, uncontrolled HTN or flash pulmonary oedema
Define acute kidney injury and describe factors contributing to its development
‘decline of renal excretory function over hours or days, recognised by the rise in serum creatinine and drop in urine output’
Pre-Renal - Circulatory Failure/Shock - Reduced Perfusion of the Glomerulus
Renal - Cells of the Kidney
Post-Renal - Obstruction
Define glomerulonephritis
Glomerulonephritis (GN) is a renal disease characterised by inflammation and damage to the glomeruli that allows protein (+/- blood) to leak out into the urine
State methods of assessing kidney function and their uses and limitations
- 24hr Urine Collection (g/24h)
- Cumbersome, not routinely used in clinical practice
- Protein:Creatinine Ratio (PCR) (mg/mmol)
- Albumin:Creatinine Ratio (mg/mmol)
- Estimation of GFR
- Based on plasma creatinine concentration
- Not suitable in AKI
- Affected by muscle mass
Describe the pathophysiology, presentation and management of amyloidosis
Deposition of highly stable insoluble protein material in extracellular space in the kidney, heart, liver and gut
AA = Systemic Amyloidosis - Treat underlying source of inflammation/infection
AL = Immunoglobulin fragments from haematological conditions (e.g. myeloma) - Treat the underlying haematological condition
State common types of renal stones
- Calcium (80%)
- Calcium Oxalate Monohydrate or Dihydrate
- Calcium Phosphate
- Infection (10%)
- Struvite
- Uric Acid Stone (5%)
- Not seen on X-Ray
- Others (1%)
- Cystine, Xanthine, Silica
State functions of the kidneys
Metabolic waste excretion
Endocrine functions
Drug metabolism/excretion
Control of solutes and fluid status
Blood pressure control
Acid/base balance
State indications for renal replacement therapy
Hyperkalaemia
Acidosis
Uraemia
Fluid Overload (hypertension, pulmonary oedema)
Describe the management of UTI
Treatment with antibiotics empirically while awaiting cultures and sensitivities
Oral therapy should be used unless severely ill, vomiting or in infants <3 months
Oral - Trimethoprim, Cephalosporin, Co-Amoxiclav, Nitrofurantoin
IV - 3rd Gen Cephalosporins (Ceftriaxone) or Aminoglycosides (Gentamicin)
Describe IgA nephropathy, its diagnosis and management
Most common type of GN in adults worldwide
Proliferative
Characterised by mesangial proliferation, increased IgA production and IgA deposition
Often presents 24-48hrs after a URTI
Can present with haematuria, hypertension and proteinuria (nephritic syndrome)
Biopsy needed for definitive diagnosis
Managed with anti-hypertensives, ACEi, steroids
Describe the pathophysiology of renal stone disease
- Abnormal Urine
- Too much calcium
- Too much acid
- Hypercalciuria
- Hyperoxaluria
- Stone inhibitors (citrate, magnesium)
- Obstruction
- Congenital or Acquired
- Infection
- Particularly urease-producing organisms
- Raises urine pH
Describe the two main congenital abnormalities of the kidneys and urinary tract
- Vesico-Ureteric Reflux
- Retrograde passage of urine from the bladder into the upper urinary tract
- May present with UTI and pyelonephritis
- Can result in renal scarring
- Low-grade VUR is more likely to spontaneously resolve
- Manage with antibiotic prophylaxis or STING procedure or open ureteric re-implantation surgically
- Bladder Outlet Obstruction
- Posterior Urethral Valve
- Antenatal hydronephrosis, UTI, poor urinary stream, renal dysfunction
- Manage with valve resection, antibiotic prophylaxis, CKD care
- Pelvi-Ureteric Junction Obstruction
- Abdominal mass, pain, haematuria, UTI
- Manage with pyeloplasty
- Vesico-Ureteric Junction Obstruction
- Anatomical or functional narrowing
- Antenatal dilation, UTI, abdominal mass, pain, haematuria
- May improve or resolve spontaneously
- May need resection
Describe the medical management of chronic kidney disease
- Treatment to slow renal disease progression
- Aggressive BP control (ACEi/ARB)
- Improved glycaemic control
- Exercise
- Sodium restriction
- Treatment of renal complications
- Manage anaemia (iron, B12, folate, EPO stimulator)
- Acidosis (sodium bicarb supplements)
- Oedema (fluid/sodium restriction, diuretic)
- Bone mineral disorders (Vit D supplements, phosphate binders)
- Other
- Statins
Describe other inherited cystic disorders of the kidneys
- Von Hippel Lindau
- Autosomal dominant
- Causes multiple benign and malignant neoplasms
- Renal cysts and multifocal renal cell carcinomas
- Tuberous Sclerosis
- Autosomal dominant
- Benign hamartomas of multiple systems (brain, eyes, heart, lung, liver, skin, kidney)
- Up to 80% have renal involvement with multiple cysts, angiomyolipomas (high risk of bleeding) and renal cell carcinoma
- Replacement of renal tissue leads to kidney failure
- Medullary Cystic Kidney Disease
- Autosomal dominant
- Cysts at the cortico-medullary junction
- Causes hyperuricaemia and gout
Describe the diagnosis of UTI/Pyelonephritis
- Multistix
- Useful for children >3 years
- +ve LE & Nitrite = UTI in 90%
- Microscopy/Flow Cytometry
- If -ve for pus cells and bacteria = No UTI
- Urine Culture
- Single Organism >= 105 CFU/ml
Define nephrotic syndrome
3.5g Proteinuria per 24h (Urine PCR>300)
Serum Albumin <30
Oedema
(Hyperlipidaemia)
Describe minimal change glomerulonephritis
Non-proliferative
Most common GN in children
Presents with nephrotic syndrome
Often idiopathic, but can be secondary to malignancy
Electron microscopy shows fused podocyte foot processes
Manage with supportive care (e.g. to reduce oedema) and prednisolone
Describe membranous glomerulonephritis, its diagnosis, management and prognosis
Presents with nephrotic syndrome
Non-proliferative
Caused by immune complex deposition, which results in complement activation against glomerular basement membrane proteins
Microscopic analysis shows thickened glomerular basement membrane
Immunofluorescence shows diffuse uptake of IgG
Treat underlying disease if secondary
Supportive non-immunological - ACi, statin, diuretics, salt restriction
Immunotherapy can be used if disease progresses (steroids, cyclosporin)
1/3rd spontaneously remit, 1/3rd have chronic membranous GN, the remaining 1/3rd progress to end-stage renal failure
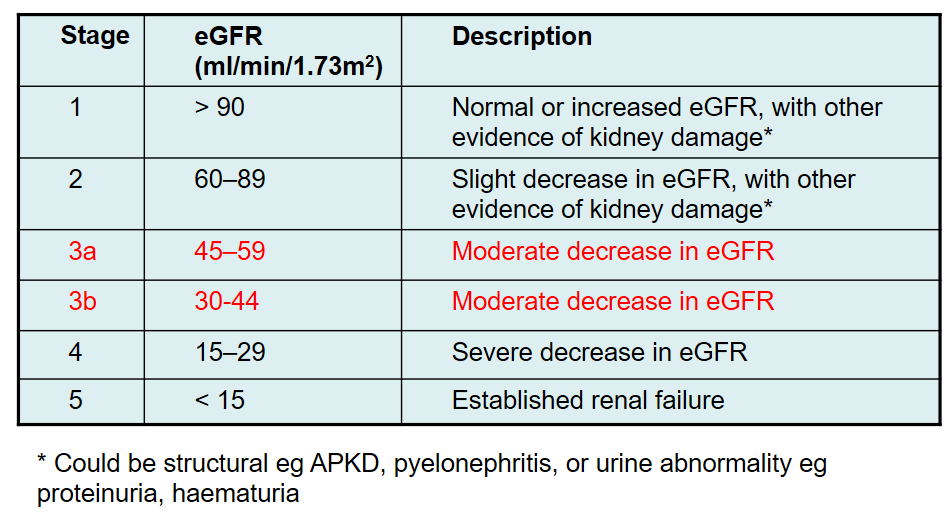
Define chronic kidney disease and a system to classify its severity
‘kidney damage or GFR <60ml/min per 1/73m2 for three months or more’
Classified based on eGFR
Describe haemodialysis and its potential complications
Aims to remove solutes (potassium, urea) by diffusion and fluid by convection
Blood is passed over a semi-permeable membrane against dialysis fluid flowing in the opposite direction
DIffusion of solutes occurs down the concentration gradient
Access is usually through an arteriovenous fistula
Most commonly hospital-based
Standard regimen is 4 hours, 3 times a week
Problems include access complications, hypotension, cramps, fatigue, infection, dialysis disequilibrium
State risk factors for UTI
Infancy (<1 yr)
Abnormal Urinary Tract (Congenital or Other)
Female Sex
Bladder Dysfunction/Incomplete Emptying
Foreign Body (Catheter, Stone)
Diabetes Mellitus
Renal Transplant
Immunosuppression
State the range of organisms that cause UTI
Usually anaerobes and gram -ve bacteria from bowel/vagina
E.coli is the most common community organism
Staphylococcus saprophyticus and klebsiella pneumonia are other organisms involved
Describe the pathophysiology, presentation and management of diabetic nephropathy
Hyperglycaemia leads to volume expansion, intra-glomerular hypertension, hyperfiltration, proteinuria, hypertension and renal failure
Diabetic disease induces structural changes, thickening of glomerular basement membrane, fusion of podocyte foot processes and loss of podocytes
Often presents after retinopathy with proteinuria as a hallmark
Mainstay of treatment is tight glycaemic control, good BP control (with ACEi/ARB) and SGLT-2 inhibitors
Describe the pathophysiology, presentation and management of SLE
Auto-immune disease with immune complex mediated glomerular disease
Multiple autoAbs, directed against DNA, histones etc.
Form intravascular immune complexes or attach to GBM
Complement is activated leading to renal damage
Can present with elevated creatinine, proteinuria, nephritic syndrome
Treated with immunosuppression - steroids, rituximab, cyclophosphamide
