Changes in respiratory in pregnancy (6)
- airway anatomy: edema and friable; difficult intubation
- MV and alveolar vent: increases 50% by term 2/2 increase TV (40%) RR 15% (progesterone increases sesitivity to Co2)
- FRC: 20% decrease by term (ERV and RV decrease 20%), rapid desat
- IC increases by 15%
- increased V02 20% prediposes to rapid desat also decrease time required for inhalation induction & pre-oxygenation (de-nitrogen)
- ABG: 7.44/30/103/22
- P50 27 to 30
CV changes in prenancy (3)
- elevated CO predisposes to CHF (40% 1st, 50% term; labor 40% 75% delivery, 30% post 1 hr, , normal 2 weeks (HR 25% SV increases 40%)
- aortocval compresson 18-20 weeks–>compromise venous return (hydration and LUD essential)
- SVR decreases: Decrease BP diastolic>systolic
Heme changes in pregnancy (4)
- anemia: plasma volume increases 50% RBC volume 25% ~hct 35 Hbg 11 (15% decrease)
- Leukocytosis
- hypercoagulable state: 7,8,9,10, 12 increase, fibrinogen increases (11, 13, AT3 decrease)
- plasma protein decrease: total protein, albumin, including plasma cholinesterase (decrease colloid oncoitc pressure. unclear if this increases free fraction of drugs or contibute to edema. increased vascular permeability
gastrointestinal changes in pregnancy (2)
- gastric emptying slows during labor, volume increase pH decreases during labor (not gestation)
- decrease LES tone 2/2 progesterone (Aspiration risk 18-20 weeks)
renal changes in pregnancy (1)
RBF and GRF increases (creatine 0.5-.6) BUN 8-9
endocrine changes in pregnancy(2)
- impaired glucose tolerance
- TBG causes increase in total T3 and T4 levels with no change in free levels
Anesthesia changes in pregnancy (3)
- MAC decreases by 40%
- increase sensitivity to local (cardiac toxicity esp to bupi enhanced)
- decreased epidural space and venous engorgaement increase risk of IV injection and dural puncture
How to assess fetal well being preoperatively
- H&P focusing on prenatal care, last medical assessment, any prenatal problems
- ask about fetal body movements
- obtain FHR tracing (detect 16 weeks), look for rate (120-160) and variability-25-27 weeks (6-10bpm beat to beat varibility): ensure optimal uteroplacental blood flow and O2 delivery to fetus. if bradycardia occurs could promp search for materal condition like maternal hypotension and anemia
ddx of fetal tachycardia and bradycardia
tachycardia:
hypoxemia (sympathetic stimulation),
maternal fever #1, maternal thyrotoxicosis, terbutaline, atropine, arrythmia
bradycardia:
severe hypoxia/uretoplacental issues, uterine hypertonus, head compression,
hypothermia, complete heart block (SLE antibodies), paracervical block
What is significance of early decels
normal finding from fetal head compression causing parasympathetically induced bradycardia
Cause of late decels?
what would you do?
false alarms common, but can suggest urteroplacental insufficiency
- determine severity. FHR <100 prompts tx, <60 prolonged may require emergency obstectric intervention. Loss of varibility makes prognosis worse
- check mom ABC: 100% O2, well oxgengated, LUD, optimize hemodynamics (fluid/pressors
- determine the circumstance surrounding the change. recieve LA, oxytocin, pt sx,
- make sure OB aware and discuss tx
significance of loss of short term varaibility
ddx?
etio: sym and para sym interaction is lost consistent with asphyxia
benzos, narotics, absoption of local
mag, atropine, steriod
ancephaly/neurological ab/hypxoxia/ prematrity/ fetal sleep
When would you want scalp pH
to determine significance of nonreassuring FHR
late decels good varaibility >7.25 good <7.2 bad
significance of variable decal: rule 60s
umbiical cord compression. serious if <60 bmp >60 sec, decrease >60bmp
look at varaibility between decels and consider scalp pH
hypertensive dx of pregnacy and dx
- chronic HTN <20 weeks
- preeclampsia: >20 weeks, HTN >140/90 (2 6 hours apart), and proteinuria >300mg/day (1+ dipstick)
- chronic HTN with superimposed preeclampsia
signs severe preeclampsia
One of the following:
BP>160/110
proteinuria >5g/day
signs end organ effects:
neuro: visual disturbances, H/A AMS, seizures
cardiac: HTN
pulm: pulm edema
GI: epigastric/RUQ (disstension of Glisson capsule), hepatic rupture, impaired liver fxn,
renal: proteinuria >5g/day 3+ dipstick, oliguria (<400mL/day)
heme: thrombocytopenia, HELLP
fetus: IUGR, oligohyrammnios
goals with pt PIH
BP meds
preop: assess mom and baby
neuro: antiseziure ppx
cards: control BP (hydralazine and labteolol 1:7 most common), optimize fluid status
pulm: avoid overhydration, prone to pulm edema
renal: ensure adequate hydration and UOP(prone to hypovolemia),
heme: assess couagulation status
intraop: establish neuraxial for labor or c-section (try to avoid GA) try to avoid exaggerated BP response,
postop: monitor for pulm edema (more likely postpartum 2/2 increse in preload 2/2 decompression IVC), and seizures (30% post partum, continue mag 24 hr)
BP meds during pregnancy
Labetalol decreases SVR w/o increasing maternal HR or decreasing CO/uterine blood flow; faster onset than hydralazine
Hydralazine: up to 20mg, reflex tachycardia (give labetalol 1st)
NTG: readily crosses placenta, most useful for short term treatment (intubation)
SNP: short term treatment, risk of CN toxicity w/ greater than 4mcg/kg/min x several hours
Nifedipine CCB, dilates arterial smooth muscle (SE: flushing, H/A reflex tachycardia), caution w/ concurrent Mg (risk of myocardial depression/PEd
pathophys of PIH
- failure of trophoblasts to invade materal decidua and maternal ateries retain their adrenergic innvervation
- endothelium fails to produce prostacyclin (PGI2) and NO, excess thromboxane and endothelin
- platelets show increase aggregation increase TXA2/PGI2 ratio
PIH head to toe effects
neuro: AMS, H/A, visual, cerebral edema, seziure, intracranial hemorrage #1 cause death
cardiac: elevated SVR, hypovolemia, low colloid oncotic pressure and increase vascular perm predipose to edema and hypovolemia,
pulm: airway edema, pulm edema (increase PCWP, decreased CO, excess fluid admin)
GI: distention, hemorrage, rupture, HELLP
renal: oliguria (decrease GFR), proteinuria from increase glomerular perm
heme: plt activation <100K, hypocoag, increased fibrinolysis
fetal: IUGR, decreased uteroplacnetal perfusion (placental infarcts), premature, abruption,
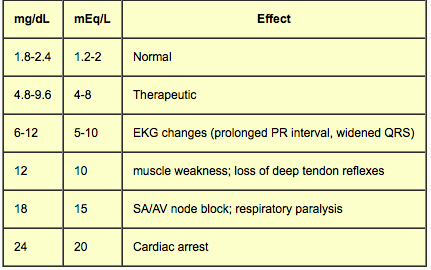
Effects of magnesium
How to treat mag toxicity
- potentiation of muscular blockade (inhibits presynaptic Ach release and motor end plate depolarization)
- decreased uterine tone/atony; prolonged labor
- decreased FHR variability and neonatal depression
- toxicity
normal 2 meq/L
theraputic 4-8
10 loss DTR, prolong QRS, QT, PR, hypotension, AMS
15: resp arrest, conduction block
25 cardiac arrest
tx: calcium, diuresis, dialysis
relative contraindications: MG, impaired renal fxn, CCB (potentiates cardiotoxic effect)
Why place an epidural for PIH
Pro con GA
- superior analgesia
- attenutate hypertensive response to pain
- reduce circulating catecholamines improving uteroplacental blood flow
- route to provide anesthesia for possible C/S
GA pro: faster?
GA COn: aspiration, airway, awareness
How will you treat seizure
- airway/breathing: bag/mask ventilate pt w crioid pressure. assess adequancy of oxygenation and ventilation. hypervent lowers seizure threshold, hypoxia, hypercarbia and acidosis exacerbate LAST
may need to intubate to control ventilation and prevent aspiration (call for difficult airway cart)
- Circulation management: control BP w fluids, pressors. (AFE)
- seizure control: assume eclampsia-tx mag 4-6g over 20 min, midaz for acute manageemnt, Intralipid for LAST
causes of antepartum bleeding, RF, pathophys,
placenta previa
pathophys: implantation placenta in LUS. bleeding from tearing of placenta, LUS contracts poorly unable to compress spiral arteries,
painless vaginal bleeding, confirm w ultrasound
RF: advanced age, prior section or uterine surgery, multiparity
complications: C/S/ through anterior placenta, failure LUS to contract, placenta accreta
delay delivery with tocolysis, blood transfusions, allow for fetal lung maturation at 37 weeks than elective c/s
placenta abruption
pathophys: premature seperation of placenta from decidua basalis, ruupture of spiral artery can lead to retroplacenta hematoma with blood that dissects decidua basalis causing futher seperation of placenta, placenta insufficiency, ineffective contractions (atony), consumption of clotting factors, increase in intrauterine pressure
RF: HTN, cocaine, smoking, stress
trauma (forceps, blunt abdominal trama), physical work,
advanced age, multiparity, low lying placenta, placenta previa, fibroids, prior abruption
signs: abdominal pain/uterine tenderness, coagulopathy (DIC), fetal distress, signs of hemorrhage may be concealed, change in uterine tone or contraction pattern
complications: hypotension, DIC, atony, sheehan syndrome (pit necrosis), RF, fetal demise
Uterine rupture
pathophys: fetal distress from hypotension or interrupton of placenta flow, 2/2 dehise of uterine scar (less pain and hemodynamic collase), forceful contraction (significant pain and collapse), trauma
RF: prior uterine surgery (VBAC), trauma, excess oxytocin (forceful contraction), multiparity, fetal macroscomia, malposition, uterine anomalies/tumors, percreata
signs: vaginal bleeding, abdominal pain(despite working epidural), hypotension, fetal distress
vaso previa
pathophys: umbilical vessels present agead of the fetus and place at risk of bleeding and tearing, and fetal hemorrhage
