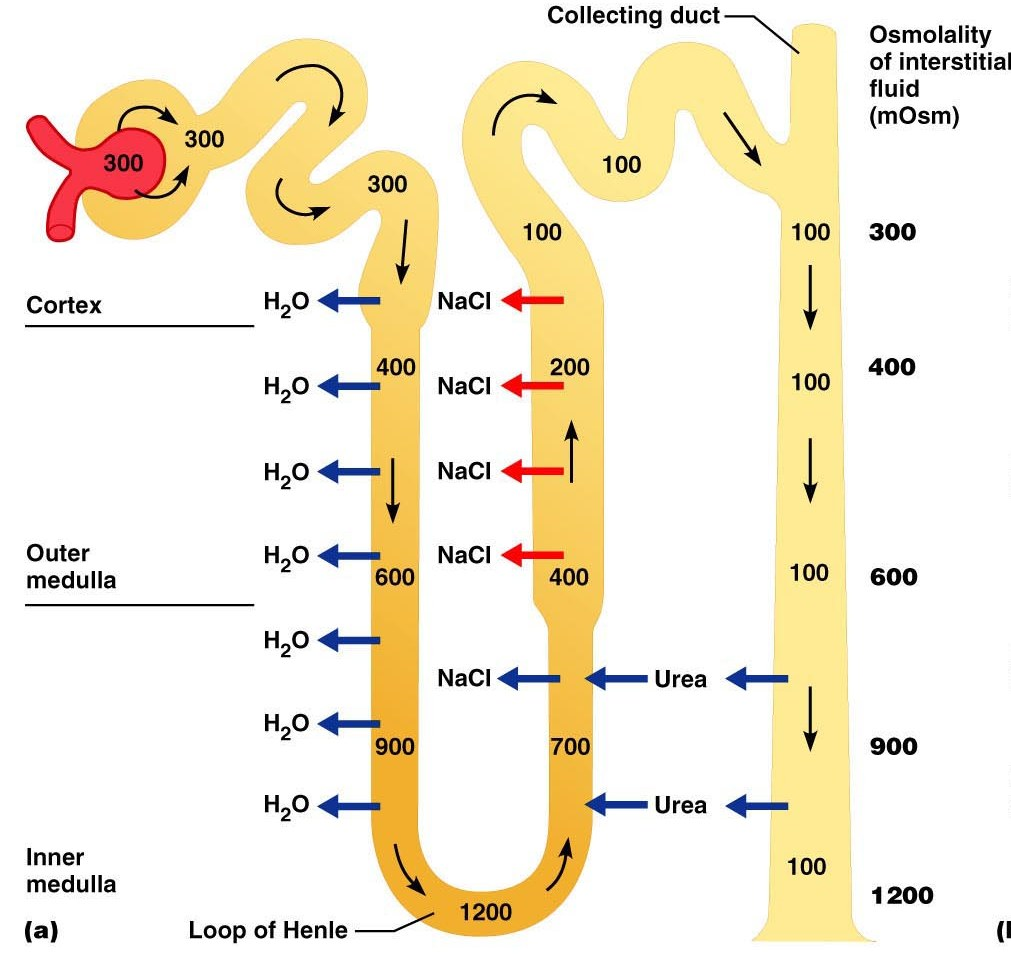
Draw a tubule and mark the osmolarity.
· Remember osmolality = measures the number of particles in solution
· Urine specific gravity measures the weight of the solution compared with water (1.000)
· Usually the two measures are roughly convertible (an osmolality of 300 mosmol/L corresponds to a USG of approx 1.007-9, USG rises by 0.001 for every 35 to 40 mosmol/L) however very large molecules in solution (like some antibiotic compounds and glucose) have a high molecular weight and can result in a higher than expected urine specific gravity reading at the same osmolality
· 300mosmol/L = 1.007/9, rises by 0.001 for every 35-40mosmol/L
· PT 300mosmol/L à 1.007USG
· LOH 1200mosmol/l à 0.023 + 1.007 à 1.03 USG
· DT and CD 100mosmol à 5 x 0.001 = 0.005, so 1.007 – 0.005 à 1.002 USG
How is urine that is more dilute (hyposthenuric) than that which leaves the glomerulus (isosthenuric) produced?
less solute being reabsorbed, so more solute in tubule so more water stays in, as less drawn out by the low solute concentrations.
How is urine that is more concentrated (hypersthenuric) than that which leaves the glomerulus (isosthenuric) produced?
more ADH
What is the normal range of cat and dog SG.
Cats: 1.001 -1.085,
Dogs: 1.001-1.075
Complete this table


Consider what Urine specific gravity range you would expect in the following animals:
A normal dog that is normally hydrated?
1.001-1.075
What do you need to assess in conjunction with urine specific gravity to determine anything about whether that USG is normal or not?
? Total protein? Glucose in the urine? Assess hydration – skin tent, sunken eyes, PCV (will be high if dehydration)
How is calcium processed in the kidney?
Half the plasma calcium is bound to proteins so it is only the ionised form which is available for filtration. Reabsorption of calcium occurs in the proximal tubule paracellulary however the regulation of how much is reabsorbed occurs in the ascending limb of the loop of henle, the distal tubule and collecting ducts.
What happens in the thin descending limb?
- Freely permeable to water
- Therefore passive transfer of water occurs
- Relatively impermeable to salt
- No active transport
- Simple squamous epithelium
What happens in the thin ascending limb?
- No active transport of salt
- Highly permeable to Sodium and chloride ions which cross the membrane via diffusion and enter the tubule
- Permeability to water very low
- Simple squamous epithelium
What happens in the thick ascending limb?
- Active transport of Na+, K+ and Cl- in a 1:1:2 ratio
- Using a co-transporter
- Impermeable to water
Simple Cuboidal epithelium
How does transport happen in the loop of henle?
· Transport of sodium, potassium and chloride from the tubule to the interstitium in the thick ascending limb is done using a Sodium/Potassium/2-Chloride co-transporter.
· 20% of the filtered sodium is reabsorbed thanks to the countercurrent multiplier from the thick ascending limb.
· Potassium leaks back into the tubule through special channels
· As with the Proximal Tubule:
· Na+ / K+ ATPases in the basolateral membrane move potassium into epithelial cells from the intercellular spaces in order to remove sodium
· Potassium is then cleared from the cells using a co-transporter with chlorine
· Cations (e.g. sodium, potassium, calcium and magnesium) can passively move paracellulary into the vasa recta
What happens in the glomerulus?
- Glomerular filtration produces a filtrate that must be modified by reabsorption and secretion in the rest of the nephron.
- Factors affecting GFR: Pressure favoring net filtration, influenced by: afferent/efferent arteriolar tone, colloid osmotic pressure, renal plasma flow (RPF), electrical charges across GBM
- What passes easily ? Neutral or +ve charged molecule, Small molecules, <8nm diameter, Round rather than ellipsoid molecules, Albumin is -ve charged thus does not freely filter
- NOTE: If drugs bind to proteins – not filtered, thus in body for longer
- Basically a protein free filtrate of plasma
What happens in the proximal tubule?
- For bulk reabsorption!
- Mostly in outer cortex (with cortical glomeruli)
- Extension of Bowman’s capsule, becomes loop of Henle
- Most reabsorption is coupled to Na ion movement, waste products retained.
o Basolateral Na, K ATPase maintains low Na concentrations
o Causing passive apical Na entry from the lumen and Na coupled transport.
o Solutes are gradually removed
o Concentrate in the interstitum and creates an osmotic potential for transport of water.
o Volume of filtrate gets less/osmolality remains stable (isosmotic)
- Highly water permeable
- Negatively charged ions build up in tubular fluid and are reabsorbed passively
- By the end of the proximal tubule
What happens in the loop of henle?
- Straight parts of the nephron
o Straight proximal
o Thin descending
o Thin ascending
o Thick ascending tubules
o Short cortical glomerular loops, and long juxtamedullary glomerular loops
- Use a counter current multiplier and counter current exchange, maintained by close apposition to vasa recta = high osmolarities
o Isotonic fluid enters loop of Henle
o Fluid becomes increasingly more concentrated as it flows down descending limb
o Fluid becomes progressively less concentrated as it flows up ascending limb
o Establishes vertical osmotic gradient in medulla to enable collecting duct to concentrate urine. Controlled by ADH.
-
o Descending loop, permeable to water not solutes
o Ascending loop, permeable to solutes not water.
o Interstitial osmolarity elevates (more ions) - draws water out of descending - solute concentration of the fluid in ascending limb is higher - causing more pumping – increases interstitial osmolarity more, more water drawn out of descending..etc..
- Vasa recta
o Get diffusion of solutes from ascending to descending blood capillary loop.
o Descending limb of vasa recta: As blood descends through areas of HIGH osmolarity (i.e. interstitium) water diffuses out of vessels and NaCl diffuses in to increase capillary plasma osmolarity
o Ascending limb of vasa recta: As hypertonic capillary plasma ascends towards cortex NaCl diffuse out and water back in
o Result: No net change in medullary gradient. The vasa recta preserves it.
- Urea recycling
o Impermable until inner medullary portion of CD.
o Passively reabsorbed
What happens in the distal tubule?
- Adjusting urinary volume, composition or pH.
- Has juxtaglomerular apparatus (RAAS) to aid
o Contact the efferent arteriole of glomerulus
- Early DT
o P cells (NaCl reabsorption and K secretion) and IC cells (acid base balance, H secretion, HCO3 reabsorption)
o NaCl reabsorption via aldosterone.
o Impermeable to water
- Late DT and CD
o Water via ADH, create aquaporin channels
o P cells (NaCl reabsorption and K secretion) and IC cells (acid base balance, H secretion, HCO3 reabsorption)
What is the function of aldosterone?
steroid hormone - works by altering gene transcription. Produced from adrenal cortex (‘mineralocorticoid’). Influenced by the renin-angiotensin-aldosterone system (‘The RAAS’).
o Important for fine-regulation of Na+ and K+ excretion
o Induces basolateral Na+ pump, new apical Na+ channels. Also influences K+ and H+ secretion in DT via apical K+ leak channels and H+ secretory proteins – ‘acid-base balance’ lectures)
What is the role of ADH?
peptide - works via increased intracellular cAMP to insert more existing (preformed) aquaporin channels in apical membrane of collecting ducts.
What is the renal regulation of urea and nitrogen?
- When vasopressin is present, urea which has been concentrated by water reaborption in cortical & medullary collecting duct (CD) diffuses out of the terminal inner medullar CD (UT-A1) into the interstitium.
- This urea can escape this region because it is taken up by blood perfusing the inner medulla and returned through the AVR toward more superficial layers of the medulla and the main veins at the cortico-medullar border.
- However the parallel and close arrangement of vessels and tubules in the medulla enable the urea flowing in the AVR to return to the inner medulla because it is reintroduced by counter-current exchange into the descending structures which have lower urea concentration, i.e. descending limbs (UT-A2) and arterial vasa-recta (UT-B1).
- This ensures that urea stays in the inner medulla contributing to osmotic forces extracting water from collecting ducts to concentrate urine.
- In addition, it ensures high urea concentration in the urine, with respect to its low concentration in plasma and enables a considerable saving in the use of water in the excretion of urea itself
What is the renal control of acid base?
- Metabolic processes yield 50-100mEq H+/day from the metabolism of proteins and lipids & 10-15 000 mmol of CO2 (removed by alveolar ventilation)
- The [H+] of body fluids must be kept constant so that detrimental changes in proteins, enzyme structure and cellular structure don’t occur
- The body has various buffers
o Bicarbonate (operates as an open system)
o Non bicarbonate buffers (proteins and phosphates)
-
- H+ cannot be excreted free – free [H+] in the urine is very low and must reabsorb virtually all filtered HCO3- as loss of is the same as adding H+ to the plasma. Secreted H+ is bound to filtered buffers such as phosphate or ammonia
o Extracellular pH is the primary physiological regulator of acid secretion
- 3 organs involved: lungs, liver, kidney
o Lungs remove 10-15 000mmol CO2 (volatile acid) by alveolar ventilation each day
o Liver metabolises amino acids from protein catabolism to glucose or triglyceride and NH4+ released
o Urea synthesis in liver (from NH4+ & CO2) produces H+ (and HCO3- is titrated)
o Kidneys excrete NH4+ and there is a net gain of HCO3- and net loss of H+
§ Kidneys must excrete 50-100 mEq of acid (noncarbonic) per day by H+ secretion
· Na/H exchange in the proximal tubule and bicarbonate reabsorbtion
·
· Active H+ ATPase pump in the collecting tubules
·
- Bicarbonate resorption is controlled by
o Luminal HCO3- concentration
o Luminal flow rate
o Arterial pCO2
o Angiotensin II (via decrease in cyclic AMP)
o An increase causes increased bicarbonate reabsorption
Would highly recommed opening the word doc for more pics and info which could not be FC.
k.
-
Evaluation of urinary tract disease54
-
Renal Physiology21
-
CKD & AKI26
-
Fluid Therapy9
-
Infectious Diseases7
-
Large Animal Toxicity9
-
Drug Choices and Therapeutics21
-
Blood Results28
-
Chronic kidney disease79
-
Acute Kidney Injury65
-
Urinary pathology98
-
Urinary Imaging112
-
Fluid therapy in urinary tract disease56
-
Diagnostic approach to polyuria and polydipsia (PUPD)48
-
Neoplasia of Urinary Tract62
-
Congenital And Neonatal Abnormalities82
-
Urinary tract infections39
-
Urinary Tract Disease in Reptiles and Birds85
-
Q and A with steve and jane3
-
Small Animal Urinary Tract Imaging Cases13
-
Interpreting Urinalysis Results48
-
Haematocrit stuff5
-
Crystal quiz9
-
Pu/Pd toolkit20
-
Lower Urinary Tract Disease60
-
Feline Lower Urinary Tract Disease, Calculi and Blocked Cats48
-
Urinary Tract Surgery11
-
Is It Incontinent?8
-
FLUTD7
-
Calculi in Dogs (and Other Pets)18
-
Equine Urinary Disease64
-
Hypertension/renal failure CR14
-
Practical urinary pathology14
-
Equine Urinary Tract9
-
FLUTD CR10
-
Cattle Urinary Disease23
-
Contrast Radiographs16
-
Fluid Therapy In Practice36
-
Urinary Incontinence32
-
Calculi in LA11
-
Principles of urinary surgery53
-
CR Billy the dalmation18
-
Formative MCQ20
-
Formative clinical reasoning6
