where are the 3 locations of narrowing of the oesophagus?
- level of cricoid cartilage (C6)
- posterior to left main bronchus and aortic arch (T4)
- lower oesophageal sphincter (T11)
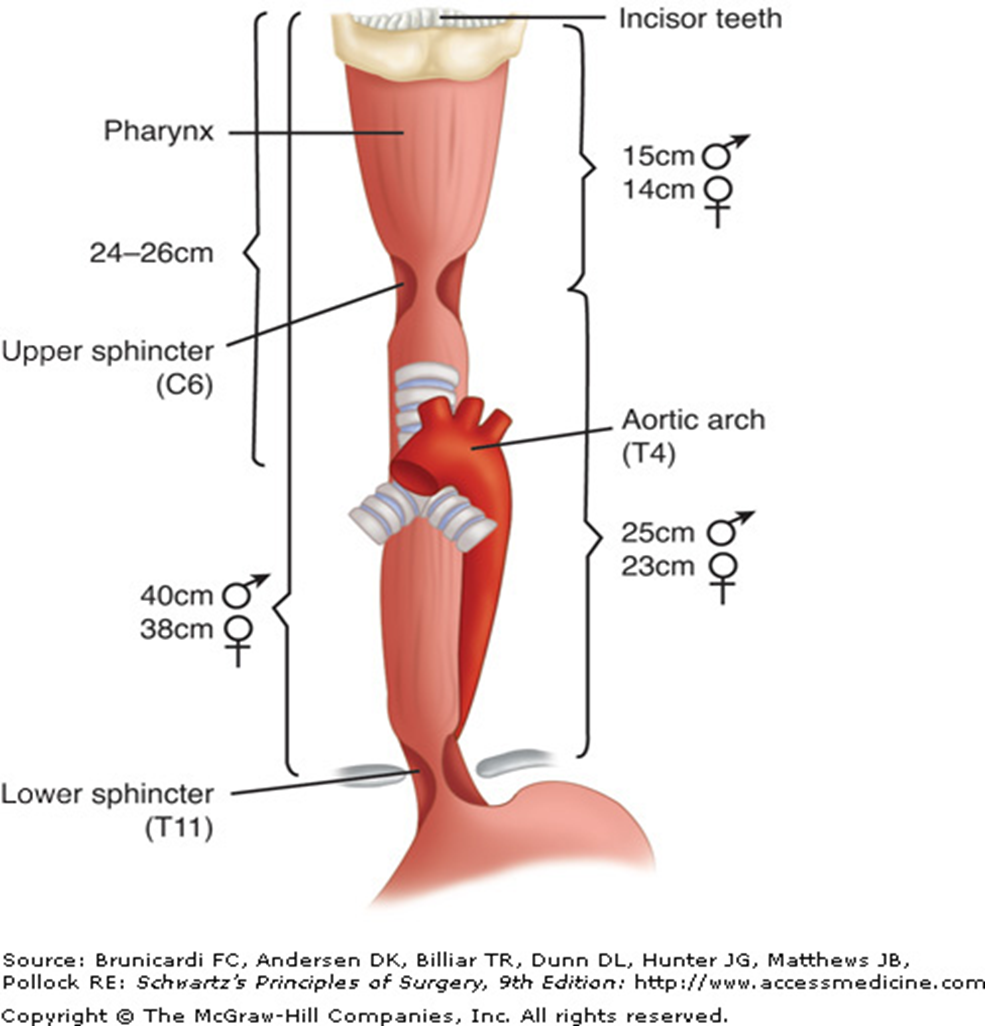
what is the z line in the oesophagus?
transition from squamous to gastric columnar epithelium
Ix for dysphagia
Upper GI endoscopy
Barium Swallow
Manometry (assess LOS fn)
projectile vomiting
child hungry after vomiting
failure to gain weight
dehydration/ constipation
Dx?
Pyloric stenosis
diagnosis of pyloric stenosis?
test feed- visible peristalsis
Abdo USS to visualize the hypertrophied pyloric sphincter
abdo xray - may reveal dilated stomach w minimum gas in bowel.
barium meal - reveals the pyloric obstruction w characteristic shouldering of the pyloric antrum
what is the metabolic abnormality with pyloric stenosis?
hypochloraemic hypokalaemic met alkalosis
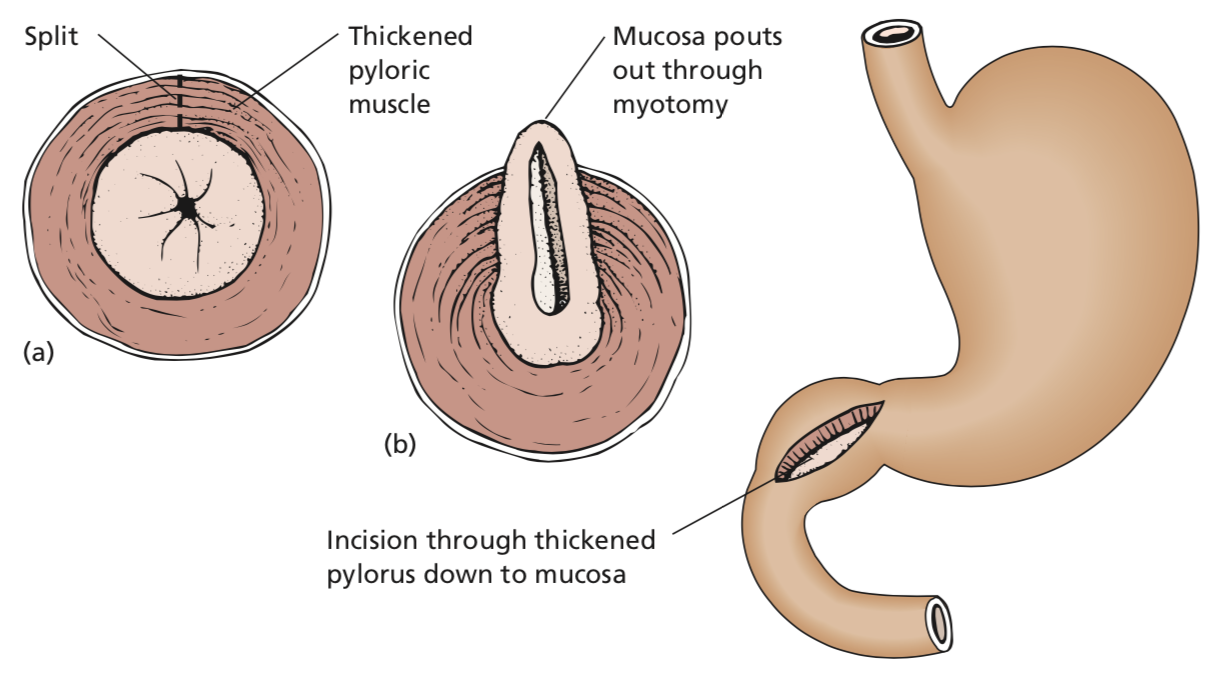
what is Ramstedt’s pyloromyotomy?
for pyloric stenosis
- a longitudinal incision is made through the hypertrophied muscle of the pylorus down to mucosa and the cut edges are separated.
commonly done laparoscopically.
infant is given glucose water 3h after op and followed by 3hrly milk feeds.
what medications predispose a pt to peptic ulceration and perforation?
steroids
NSAIDs (aspirin, indometacin, ibuprofen etc)
examination findings of a pt with perforated peptic ulcer
patient in severe pain
cold and sweating w rapid, shallow respirations
abdomen rigid and silent
pneumoperitoneum -> may lead to diminished liver dullness
presentation of peptic ulcer perforation on examination
in a delayed (>12h onset) presentation
if delayed (>12h) presentation
features of generalized peritonitis with paralytic ileus
distended abdomen
vomiting
pt extremely toxic and in oligaemic shock
Ix to order for suspected perforated peptic ulcer
CXR: erect.
- free gas below the diaphragm
CT abdo
- to detect free intraperitoneal gas and can exclude common differentials e.g. pancreatitis
DDx of perforated peptic ulcer
perforated appendicitis
acute cholecystitis
acute pancreatitis
myocardial infarction
tx of perforated peptic ulcer
NG tube: to empty stomach and decrease further leakage
Pain relief: opiates
IV fluid resus
ABx to contend w peritoneal infection
IV H2 blocker or PPI
Immediate operative repair of the perforation
what does surgery of perforated peptic ulcer involve?
suturing of omental plug to seal the perforation
+
lavage of the peritoneal cavity
+
biopsy of *gastric ulcer to exclude malignancy
Postoperative tx for perforated Peptic ulcer
H pylori eradication
omeprazole, amoxicillin, clari
profuse vomiting, non-bilious
may contain food particles
weight loss, constipation, weakness due to electrolyte disturbance
pyloric stenosis
Examination findings of pyloric stenosis
visible peristalsis seen, from L-R of upper abdomen
grossly dilated, hypertrophied stomach, full of stale food and fluid, can be palpated
gastric splash (succussion splash) can be elicited by shaking pt’s abdomen several hrs after a meal
Ix of pyloric stenosis
Gastroscopy - following decompression of stomach w NG tube
CT scan
ABG and electrolytes-> hypochloraemic, hypokalaemic alkalosis and uraemia
metabolic disturbances of pyloric stenosis
dehydrated, Hct raised
serum Cl, Na, K low
plasma bicarb and urea raised
alkalosis
DDx of pyloric stenosis
ca of pylorus
Other causes of pyloric obstruction are unusual
in the adult:
- scarring associated with a benign gastric ulcer near the pylorus;
- carcinoma of the head of the pancreas infiltrating the duodenum and pylorus;
- chronic pancreatitis;
- invasion of the pylorus by malignant nodes.
differentiating between benign ulcer-> pyloric stenosis vs carcinoma of the pylorus
- Length of history: a history of several years of characteristic peptic ulcer pain is in favour of benign ulcer. Cancer usually has a history of only months and indeed may be painless.
- Gross dilatation of the stomach favours a benign lesion, as it may take several years for this to develop.
- The presence of a mass at the pylorus indicates malignant disease, although, rarely, a palpable inflammatory mass in association with a large duodenal ulcer can be detected.
tx of pyloric stenosis
preop:
IV saline + K to correct dehydration/ electrolyte depletion
daily gastric lavage to remove debris from stomach
Vitamin C
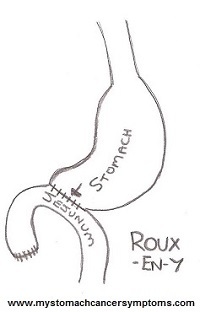
surgical correction:
usually an antrectomy w a Roux-en-Y gastroenterostomy
oesophageal causes of GI haemorrhage
- reflux oesophagitis (associated with hiatus
hernia) ; - oesophageal varices (associated with portal
hypertension)
- peptic ulcer;
- tumours (benign and malignant).
stomach causes of GI haemorrhage
gastric ulcer
acute erosions (assoc w aspirin, other NSAIDs, corticosteroids)
gastritis
Mallory-Weiss tear
vascular malformation (e.g. Dieulafoy lesion)
tumours (benign and malignant)






















-
Upper GI Surgery200
-
Lower GI Surgery253
-
Post Op Complications5
-
trauma and ortho342
-
Ophthalmology220
-
Ear, Nose and Throat256
-
Urology173
-
Vascular Surgery121
-
Breast Surgery62
-
Superficial Lesions131
-
Hernia40
-
Perianal surgery55
-
Fluids and Nutrition42
-
Trauma42
-
General Surgery272
-
Hepatobiliary71
-
PreOp Mx51
