A kg increase in bodyweight leads to what % increase in the risk of developing diabetes?
A kg of weight loss a year after a diagnosis of T2DM is associated with how many months of increased survival?
4.5%
3-4 months more survival
How is Lactic Acidosis classified?
Type A
- associated with tissue hypoxaemia e.g. infarcted tissue, cardiogenic shock, hypovolaemic shock
Type B
- may occur in liver disease
- may occur in leukaemic states
- associated with diabetes
What marker is used to screen for diabetic kidney disease?
Albumin Creatine Ratio (ACR)
In managing and preventing childhood obesity, what are the 1, 2, 3, 4 steps outlined in the SIGN and NICE guidelines?
- 1 hour of physical activity a day
- less than 2 hours a day of ‘sedentary time’ i.e. TV, computer screens etc.
- Food and drink - limit foods high in fat and sugar, discourage multiple snacks and moderate portion size
- keep child’s weight within a healthy range
Thiazolidinodiones (TZDs): what do they target? Why does this make them “messy” drugs?
What is the main side effect associated with TZDs?
TZDs e.g. pioglitazone targets PPAR gamma, which is involved in the regulation of transcription of many different genes.
Because TZDs are PPAR-gamma agonists, they therefore have numerous side effects
Main side effect is weight gain, which is almost inevitable and can be quite substantial
Metformin is the 1st line drug in treating T2DM, but if a patient is not coping on this alone what other drugs could be added on?
Sulphonylureas - cheap and effective, but weight gain is a possible side effect
SGLT-2 inhibitors - better tolerated with weight fluctuation, however are (very rarely) associated with DKA
GLP-1 agonists if the above don’t work - given as an injection either daily or weekly and slow gastric emptying
How is DKA diagnosed biochemically? 3 things
- Ketonaemia > 3 mmol/L, or significant ketonuria
- Blood glucose > 11.0 mmol/L, or known Diabetes
- Bicarbonate < 15 mmol/L, or venous pH < 7.3
What newer drugs are available for the treatment of T2DM?
How do they work?
Drugs targeting the Incretin Pathway
- Incretin = Intestinal Secretion of Insulin
- GIP from K cells and GLP-1 from L cells (Exenatide)
- promote insulin secretion from the pancreas without the risk of hypoglycaemia (unlike SUs)
- Suppress glucagon
- Decreases gastric emptying, resulting in earlier satiety
- Act on the hypothalamus to cause weight loss
- DPP-IV inhibitors
- -gliptins
- less potent than GLP-1 inhibitors,
SGLT-2 Inhibitors e.g. Dapagliflozin, Canagliflozin, Empagliflozin
- prevents reabsorption of glucose by the kidneys, causing it to be excreted in the urine
- Causes weight loss, reduces CV events, death and hospitalisation from heart failure
- Increased glucose in the urine can result in increased UTIs and Thrush
Glicazide, Glibenclamide and Glimepiride are 1st/2nd gen Sulphonylureas and are long/short acting
Glicazide is the most commonly used, but when would you use Glibenclamide over it? Why?
2nd gen (1st gen are rarely used now)
shorter acting
Glibenclamide can be used in pregnancy/gestational diabetes, as it does not cross the placenta
What are the two core defects seen in T2DM?
Insulin resistance
Beta cell dysfunction
The “metabolic syndrome” refers to a series of clinical features associated with central obesity - what are these features?
Central adiposity a.k.a. ‘apple shapes’ is associated with…
- High BP
- High triglycerides
- Low HDL
- Insulin resistance
What type of drug is Metformin?
What dosage is given?
Biguanide - acts as an insulin sensitiser, primarily acts on the liver to lower glucose production
Usually start at 500mg and titrate up to 1g
Name some sulphonylurea drugs
Glimepiride
Gliclazide
Glibenclamide
Glipizide
How is DKA managed?
Replace losses
- fluids
- insulin
- potassium
Address risks
- Naso-gastric tube?
- monitor potassium
- prescribe prophylactic LMWH
How might focal neuropathy present itself?
- Inability to focus
- Double vision
- Aching behind the eye
- Bell’s palsy
- Pain in thigh/chest/lower back
- Pain on the outside of the foot
Name some SGLT-2 inhibitors
Dapagliflozin
Empagliflozin
Canagliflozin
Ipragliflozin
When considering a diagnosis of T2DM, what other conditions need to be ruled out?
T1DM
Pancreatic disease
LADA
Medication induced
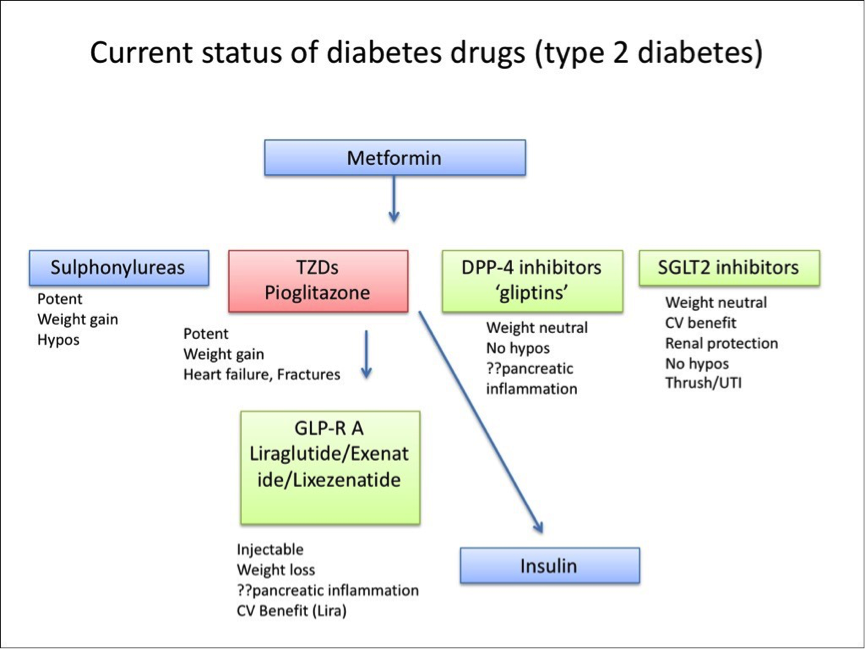
Outline the current progression of medications for T2DM
Metformin
SUs, TZDs, DPP-4 inhibitors, SGLT-2 inhibitors
GLP-1 agonists
Insulin (unlike T1DM, this is usually given as a basal injection without a pre-meal bolus)
By what features is HHS defined?
Hypovolaemia
Hyperglycaemia (blood glucose >30 mmol/L), without significant acidosis or ketonaemia
Hyperosmolar (osmolality >320 mosmol/kg)
What are the typical features of Hyperosmolar Hyperglycaemic State (HHS)?
Usually older individuals, but may be younger individuals in non-Caucasians
High refined CHO intake pre-event
Risk associations - cardiovascular events, sepsis, medications (glucocorticoids and thiazides)
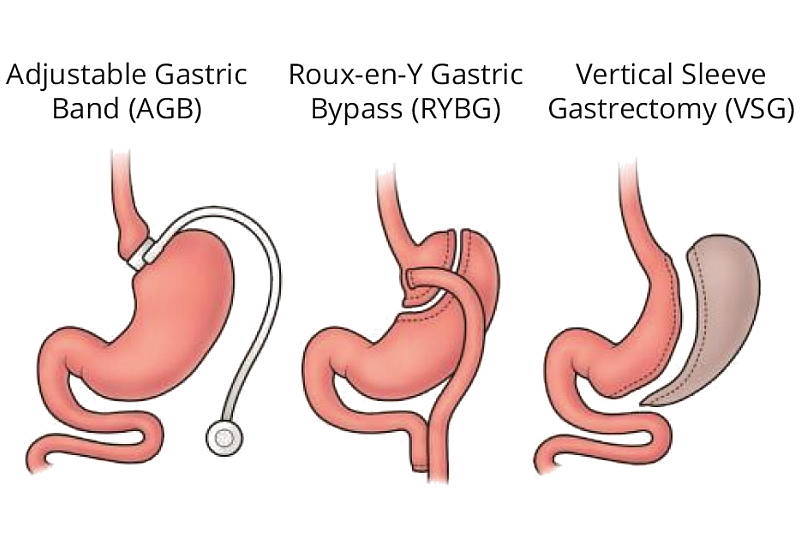
What are the three types of bariatric surgery that can be performed to tackle obesity? What are patients often prescribed following surgery?
Adjustable gastric band (lap band)
Roux-en-Y Gastric Bypass (RNY)
Verticle Sleeve Gastrectomy
Malabsorption disorders are common following these procedures, and patients are commonly prescribed vitamin supplements
HHS - typical biochemical picture
Raised blood glucose, higher than that of DKA (mean is 60 mmol/L)
Significant renal impairment
Na may be raised on admission
Significantly raised osmolality e.g. very dehydrated
What are some treatment options for painful neuropathy?
amitriptyline, duloxetine, gabapentin, pregabalin - combinations of these are not recommended
If the pain is localised and the patient wishes to avoid oral treatment, then Caspaicin cream can be applied topically
What is the Resting Metabolic Rate? How does it change in obesity and how does it contribute to maintaining weight loss?
Amount of energy expended at rest (i.e. minimum energy consumption)
Both fat mass (FM) and fat-free mass (FFM) contribute
RMR is higher in obese individuals and falls with weight loss, HOWEVER, the observed fall in RMR often exceeds that which was predicted (adaptive thermogenesis - body perceives weight loss as a threat to survival)
This makes it harder to maintain weight loss, because the lower the RMR, the harder it is to lose weight


