You are counseling a couple who have been told their unborn child has probable Beckwith-Wiedeman syndrome. You discuss with them the various potential complications of the condition & they are particularly concerned about the risk of Wilm’s tumour.
Which of the following features of Beckwith-Wiedeman syndrome is most strongly associated with increased risk of Wilm’s tumour development in the future?
A. Hemihypertrophy
B. Macroglossia
C. Macrosomia
D. Omphalocele
E. Neonatal Hypoglycaemia
A. Hemihypertrophy
Risk of tumours is 4-7%, 60% are Wilms Tumours.
In Beckwith-Wiedemann syndrome the prevalence is about 1% of children with Wilms tumor.
Isolated hemihypertrophy prevalence is about 2.5% of children with Wilms tumor.
You are asked to review a child who can run, jump with 2 feet together & build a tower of 4-6 blocks. They are able to feed themselves with a spoon, combine words & name 6 body parts.
They have a developmental age of approximately:
A. 12 months
B. 18 months
C. 24 months
D. 30 months
E. 36 months
C. 24 months
Long acting β-agonists are not recommended as monotherapy in paediatric asthma management due to tolerance secondary to:
A. Depletion of secondary messengers
B. Increasing binding affinity for ß2 receptors
C. Internalization of ß2 receptor
D. Reduction of ß2 density
E. Upregulation of ß2 receptors
D. Reduction of ß2 density
14 year old boy who is cognitively stable developed left sided seizure (was it seizure or weakness, can’t remember). At 8 months old, he had right sided preference and developed clumsiness from left hand. MRI shows:
A. Band heterotrophia
B. pachygyria
C. Porencephalic cyst
D. Schizencephaly
E. lissencephaly
D. Schizencephaly
- Presence of unilateral or bilateral clefts within cerebral hemispheres due to abnormality of morphogenesis
- cleft fused or unfused (communicate between ventricles and extra-axial space) and, if unilateral and large, can be confused with porencephalic cyst
- borders of cleft often surrounded by abn brain esp micrgyria
- CT diagnostic
- Severe mental retardation, difficult to control seizures, microcephaly, spastic quadriparesis when clefts bilateral
- Unilateral schizencephaly – frequent cause of congenital hemiparesis
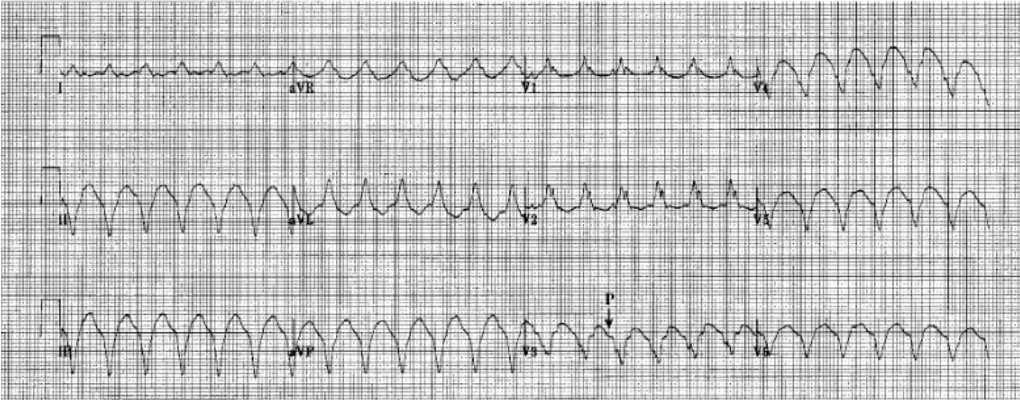
12y boy presents to ED pale and tachycardic with BP 90/60. ECG showed a regular, broad-complex tachycardia.
Normal cardiac exam, palpable pulse, possibly alert.
A. cardioversion
B. adenosine
C. amiodarone
D. vagal manouvre
E. lignocaine
A. Cardioversion
Broad complex tachy:
- Assume VT
- Stable – medical cardioversion with amidarone (DC shock or lignocaine considered after)
- Unstable – cardiovert (synchronous DC shock) – 0.5,1 then 2j/kg. can give amiodarone and lignocaine in between
Narrow complex
- likely SVT (can be sinus tachy)
- Stable – vagal manoeuvres, adenosine (medical cardioversion)
- Unstable – cardioversion (synchronous DC shock). Try above only if won’t delay cardioversion
34 weeks preterm, was diagnosed with capillary haemangioma located on right parietal area, at birth. On follow up after 2 weeks it has increased to 5 cm in size and has been bleeding, what would be the immediate management?
A. Intra-lesional steroid
B. Systemic/oral steroid
C. Propranolol
D. Laser surgery
E. Alfa Interferon

C. Propranolol
Propranolol now considered first line treatment
if rapidly growing/compromising vision.
Most rapid response seen with po steroids – reduce in size within 2wks.
Intra-lesional steroids can also be used.
Ulceration treated with meticulous wound care. If unsuccessful pulsed dye laser treatment may be a treatment option for ulcerations that do not respond to topical therapy.
A 2 month old girl presents with 2 days of fever and vomiting. Her temperature is 40C. Examination is unremarkable. She looks systemically well.
SPA results:
Micro:
Leukocytes: 100 x 106
Erythrocytes: 100 x 106
Epithelial cells: 0
Empiric treatment should be with:
A. Amoxycillin and Gentamicin
B. Cefotaxime and Gentamicin
C. Cefotaxime
D. Gentamicin
E. Trimethoprim and Sulphamethoxazole
A. Amoxycillin and Gentamicin
6 year old boy presents with six months of soiling. This occurs daily at home, but not at school. He has a low fibre diet. His parents are separated.
On examination he has a sad appearance and is overweight. Abdominal examination demonstrates fullness with palpable stool in the left iliac fossa.
What treatment would you institute first?
A. Cognitive Behavioural therapy
B. Family therapy
C. Laxatives
D. Dietary changes
E. Transcutaneous electrical stimulation
F. Anxiolytics
C. Laxatives
8 weeks old ex 35 weeks, presents with diarrhoea since birth. Serum tests show hyponatraemic, hypokalemia, hypochloremia and metabolic alkalosis. The diagnosis is
A. coeliac disease
B. barter syndrome
C. pyloric stenosis
D. sucrase isomaltase def.
E. congenital chloride losing diarrhoea
E. congenital chloride losing diarrhoea
Congenital Chloride Diarrhoea
- defect in Na+ independent Cl-/HCO3- exchanger within ileal and colonic epithelium – exchanger absorbs chloride from gastric acid and CFTR and secretes bicarb into lumen to neutralise acidity of gastric secretion
- prenatal sign – dilated small bowel, can be mistaken for BO
- severe life-threatening secretory diarrhoea during 1st weeks of life
- lab findings – metabolic alkalosis, hypochloraemia, hypokalaemia, hyponatraemia (high plasma renin and aldosterone), fecal Cl- >90mmol/L and exceeeds fecal sodium and potassium
- need lifelong KCL and NaCL substitution
- long-term complications – urinary infections, hyperuricaemia with renal calcifications, renal insufficiency, HTN
- febrile illnesses can exacerbate symtoms with severe dehydration and electrolyte imbalance
- PPIs, cholestyramine and butyrate to reduce diarrhoea
- Often symptoms regress with age
Sucrase isomaltase def
- rare, AR disorder
- complete absence of sucrase and reduced maltase digestive activity
- sucrase isomaltase is found in brush border of the small intestine. It catalyses breakdown of sucrose and starch/maltose to glucose and fructose
- note that sucrose is a non-reducing sugar and maltose is a reducing sugar
- symptoms – begin when exposed to sucrose of glucose polymer diet (eg non-lactose based formula, pureed food esp fruits)
- diarrhoea, abdo pain, poor growth
Pyloric stenosis
- hypochloraemic, hypokalaemic metabolic alkalosis secondary to vomiting due to thickened pylorus.
Bartter (and Gitelman syndrome)
- hypokalaemic metabolic alkalosis, hyperreninemia + polydipsia, polyuria
3 yo boy presents to GP with newly diagnosed murmur. The child is pink and has normal peripheral pulses. He has mild parasternal heave, normal 1st heart sound, split second heart sound with 3/6 ESM radiating to the back and loudest on the LUSE. ECG is shown - left superior axis, not much else…
A. Pulmonary stenosis
B. Primum ASD
C. Secundum ASD
D. Coarctation
E. Aortic stenosis
B. Primum ASD
ESM ULSE - mitral regurg
ECG - Left or superior axis deviation
Child undergoes induction for ALL and found to have cerebral venous thrombosis. Which of the following chemotherapy agent is associated with CVT?
A. Aspariginase
B. Daunorubicin
C. Dexamethasone
D. Methotrexate
E. Vincristine
A. Aspariginase
Drugs that enhance the risk of thrombosis include, most importantly, L-asparaginase and steroids. There have also been reports of CVT with vincristine.
Asparaginase-induced deficiency of antithrombin III, the most important endogenous anticoagulant, significantly increases the risk of sinovenous thrombosis in the brain.
It decreases protein synthesis, including synthesis of coagulation factors. About 2% of children treated with L-asparaginase develop hemorrhagic or nonhemorrhagic infarcts consequent to CSVT.
More common SE is anaphylaxis/allergic reaction and rarely pancreatitis.
The pedigree above is most likely due to which mode of inheritance
A. autosomal dominant with variable penetrance
B. chromosomal translocation
C. x-linked recessive
D. mitochondrial
E. not sure what the last one was - might have been autosomal recessive
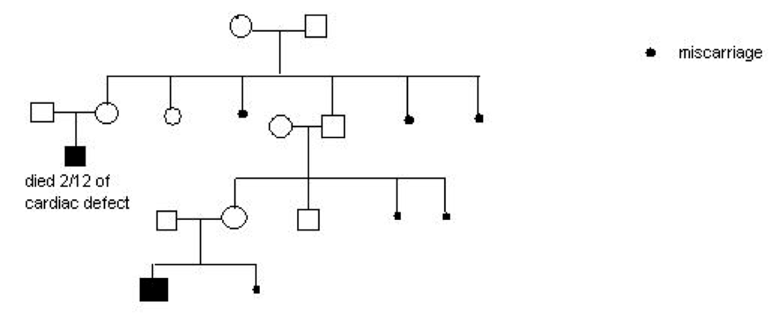
B. chromosomal translocation
Fracture of forearm – some thought its buckled, some thought is displaced. Q is on management.
Midshaft – angulated >10/displaced/bowing deformity need manipulation,
otherwise backslab
Distal 3rd –
Buckle – below elbow backslab
Greenstick - >10yrs/>10 degrees angulation/deformity refer ortho otherwise above elbow backslab
Complete without angulation – above elbow backslab
A young girl is brought in with ongoing wheeze and barking cough. As a baby she had a tracheo-oesophageal fistula repair. What is the likely cause of her current symptoms?
A. Laryngomalacia
B. Tracheomalacia
C. Asthma
B. Tracheomalacia
Occurs in 15% of cases in TOF repair
A 3 day old infant is admitted to the Special Care Nursery with feeding difficulties. On examination there is severe hypotonia but no respiratory distress and deep tendon reflexes are preserved. There is no obvious facial weakness and no dysmorphism.
The most likely cause is:
A. Congenital myotonic dystrophy
B. Myotubular myopathy
C. Prader-Wili syndrome
D. Spinal Muscular Atrophy
E. Zellweger syndrome
C. Prader-Willi Syndrome
Congenital myotonic dystrophy and Myotubular myopathy would have facial weakness.
SMA would have reduced/absent reflexes
Zellweger – dysmorphism at birth
Prader willi dysmorphism is not obvious at birth and diagnosis often missed in earlier life. Hypotonic with feeding difficulties, no facial weakness and preserved DTR.
Stem talks about comparing criteria for major depressive disorder between child and adolescents with adults. Which criteria or symptom is more common or is present in child/youth/adolescent but not in adults?
A. Hypersomnia
B. depressed mood
C. irritable mood.
D. psychomotor agitation
E. poor concentration
F. feelings of worthlessness
C. irritable mood.
Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
Note: Do note include symptoms that are clearly due to a general medical condition, or mood-incongruent delusions or hallucinations.
(1) **depressed mood. **Note: In children and adolescents, can be irritable mood.
(2) anhedonia
(3) Weight loss (or inadequate weight gain in children)
(4) insomnia or hypersomnia nearly every day
(5) psychomotor agitation or retardation nearly every day
(6) fatigue or loss of energy nearly every day
(7) feelings of worthlessness or excessive or inappropriate guilt
(8) diminished ability to think or concentrate
(9) recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide
Xray of a boy with a left-sided pneumothorax. Which of the following activities should be avoided for the next 6 months?
A. Playing the saxophone
B. Scuba diving
C. Snorkelling
D. Flying in an aeroplane
E. Flying in a helicopter
B. Scuba Diving
From Up to Date
Commercial air travel in pressurized airplanes is not thought to precipitate recurrence of pneumothorax. However, because the consequences of a spontaneous recurrence occurring during air travel may be serious, guidelines for adults suggest avoidance of air travel until at least one week after full resolution of the pneumothorax. In addition, most authorities suggest avoidance of sports that involve extreme exertion and physical contact until the pneumothorax is fully resolved.
Activities such as deep sea diving or flying in small, unpressurized aircrafts are associated with increased risk of pneumothorax and should be avoided in individuals who did not undergo pleurodesis.
3 year old child with CP, longstanding history of GOR. Normal swallow on video fluoroscopy. On Omeprazole. Which is the following an indication for fundoplication?
A. Abnormal pH probe
B. Delayed gastric emptying on NM scan
C. Reflux to mid oesophagus on barium studies
D. Growth of 3rd percentile
E. Recurrent aspiration
E. Recurrent aspiration
Indications for reflux surgery
- Esophageal stricture
- Barrett’s esophagus (an absolute indication as this may end up in cancer )
- Life-threatening apnea (cessation of breathing) and recurrent aspiration pneumonia
- Large hiatal hernia
- Failure of maximal medical therapy to reduce severe symptoms
- Severe esophagitis (esophageal inflammation)
- Recurrent pneumonia, chronic lung disease, bronchospasm
- Failure to gain weight
Thiopurine methyltransferase (TPMT) level is useful for what chemotherapeutic agent to adjust dose and reduce toxicity prior to use?
A. Azathioprine
B. Cyclophosphamide
C. Cyclosporin
D. Methotrexate
E. Mycophenolate
A. Azathioprine
TPMT is an enzyme encoded by TPMT gene. TPMT is best known for its role in the metabolism of the thiopurine drugs such as azathioprine, 6-mercaptopurine and 6-thioguanine. TPMT catalyzes the S-methylation of thiopurine drugs.
Defects in the TPMT gene leads to decreased methylation and decreased inactivation of 6MP leading to enhanced bone marrow toxicity which may cause myelosuppression, anemia, bleeding tendency, leukopenia & infection.
10% of population have low activity so should be checked prior to tx
Beta thalassaemia and other haemoglobinopathies are at risk of iron overload with repeated blood transfusions.
What is an important complication?
A. Annular corneal deposits
B. Cardiomyopathy
C. High frequency hearing loss (sensorineural deafness)
D. Malar hyperplasia
E. Pathological bone fractures
B. Cardiomyopathy
- Cardiac – hypertrophy and myopathy.
- Pulmonary hypertension
- Liver cirrhosis and hepatocelllar ca
- Endocine – almost all glands
- Neutrophils – inc ferritin, reduced phagocytosis – inc yersinia abdo infections and hepatic abscesses.
- Desferioxamine should be stopped during infection
In boys with Klinefelters syndrome (XXY) which of the following is most likely to be present:
A. Antisocial behaviour
B. Height greater than three standard deviations above mid parental height
C. Infertility
D. IQ greater than 30 points lower than siblings
E. Macroorchidism
C. Infertility
- Most common congenital cause of hypogonadism (decreased testosterone with increased LH and FSH) and associated microorchidism.
- 47XXY
- May have gynaecomastia
- Often tall
- Difficulties with social interactions and learning from adverse experience
A nine year old with pain in the shoulders and thighs upon waking up and high creatine kinase has the following lesion on the hands. What’s the most likely diagnosis?
A. Polymyosistis
B. Dermatomyositis
C. Duchenne Muscular Dystrophy
D. SLE
E. RA

B. Dermatomyositis
Gottron lesions, scaly erythematous eruptions or red patches overlying the knuckles, elbows, and knees are a characteristic feature of Dermatomyositis. Other skin manifestations involve periungual telangiectasias and a heliotropic (purple) rash over the upper eyelids.
An 11 year old boy is rescued from a house fire. He has had 2 seizures. Saturations are 100% on face mask oxygen.
Blood gas is shown, demonstrating mild acidosis
CO2 27
CO Hb - 23
What is the most appropriate treatment for this child?
A. Heliox
B. ECMO
C. Hyperbaric oxygen
D. Haemodialysis
E. Methylene blue
C. Hyperbaric Oxygen
HbCO levels often do not reflect the clinical picture, yet symptoms typically begin with headaches at levels around 10%. Levels of 50-70% may result in seizure, coma, and fatality.
Treatment of poisoning:
- 100% oxygen OR
- hyperbaric oxygen therapy,
Oxygen works as an antidote as it increases the removal of carbon monoxide from hemoglobin, in turn providing the body with normal levels of oxygen. Half-life of CO at room air temperature is 3-4 hours. One hundred percent oxygen reduces the half-life to 30-90 minutes; hyperbaric oxygen at 2.5 atm with 100% oxygen reduces it to 15-23 minutes.
Normal CO levels are around 2% but can be upto 5% in smokers/living in industrialised areas
Methylene blue – used for methaemoglobulinaemia
A 4 year old girl has developed a rash on her hands 17 days after a living related HSCT for high risk ALL. The rash is itchy. It has not spread elsewhere on her body. Her liver function tests are normal.
Picture shown of non specific erythematous rash on palmar aspects of both hands, including fingers.
What is the most appropriate initial treatment?
A. Mycophenylate mofetil
B. Methotrexate
C. Topical steroid
D. Infliximab
E. Antithymocyte globulin
C. Topical Steroid
In most patients, the first (and most common) clinical manifestation of acute GVHD is a maculopapular rash, usually occurring at or near the time of the white blood cell engraftment. Topical steroids are the most commonly used skin-directed therapy for acute GVHD. Antihistamines may be used as adjuvant therapy for patients with pruritus.
Topical steroids differ in their strength, vehicle (eg, ointments, creams, lotions), and method of application. In general, for cutaneous GVHD, mid- to high-potency topical steroids are applied twice daily to moist skin and covered with warm wet towels as an occlusive measure (“wet wrap”). The choice of topical steroid and duration of therapy must take into account the location of disease.
















-
Genetics54
-
Haematology33
-
Oncology35
-
Neonates32
-
Nephrology36
-
Cardiology58
-
Respiratory43
-
Neurology51
-
Developmental65
-
Emergency42
-
Gastroenterology52
-
Endocrinology34
-
Pharmacology31
-
Microbiology16
-
Evidence Based Medicine6
-
Immunology15
-
Infectious Diseases30
-
General2
-
Dermatology37
-
Metabolic11
-
Mental Health2
-
Rheumatology2
-
Cardiology Exam Qs 2004-199972
-
Neurology Exam Questions83
-
Gastroenterology Exam Questions60
-
Cardiology Exam Q's 2008-200549
-
Statistics and Ethics Exam Questions20
-
2008 Paper A70
-
2008 Paper B100
-
2010 Remembered Paper8
-
2013 Remembered86
-
2012 A Remembered69
-
2012 B Remembered89
-
2007 Paper A70
-
2007 Paper B100
-
2011 A Remembered63
-
2009 Remembered4
-
2011 B Remembered89
-
2006 Paper A70
-
2006 Paper B100
-
2005 Paper A70
-
2005 Paper B35
