What is bowel obstruction?
The term bowel obstruction typically refers to a mechanical blockage of the bowel, whereby a structural pathology physically blocks the passage of intestinal contents.
Briefly describe the pathophysiology of bowel obstruction
Once the bowel segment has become occluded, gross dilatation of the proximal limb of bowel occurs, resulting in an increased peristalsis of the bowel. This leads to secretion of large volumes of electrolyte-rich fluid into the bowel (often termed ‘third spacing’). Urgent fluid resuscitation and careful fluid balance is required.
What is functional obstruction or paralytic ileus?
When the bowel is not mechanically blocked but does not work properly, for example because of inflammation, electrolyte derangement, or recent surgery, this is known as functional obstruction or paralytic ileus.
What is a closed loop obstruction?
If there is a second obstruction proximally (such as in a volvulus or in large bowel obstruction with a competent ileocaecal valve) this is termed a closed-loop obstruction.
This is a surgical emergency as the bowel will continue to distend, stretching the bowel wall until it becomes ischaemic or perforates.
What are the most common causes of small and large bowel obstructions?
Small bowel: adhesions and herniae
Large bowel: malignancy, diverticular disease and volvulus
Give examples of intrluminal causes of bowel obstruction
Gallstone ileus, ingested foreign body and faecal impaction.
Give examples of mural causes of bowel obstruction
Cancer, inflammatory strictures, intussusception, diverticular strictures, Meckel’s diverticulum and lymphoma.
Give examples of extramural causes of bowel obstruction
Hernias, adhesions, peritoneal metastasis and volvulus.
What are the clinical features of bowel obstruction?
Note: signs and symptoms
The cardinal features of bowel obstruction are:
- Abdominal pain
- Colicky or cramping in nature (secondary to the bowel peristalsis)
- Vomiting
- Occurring early in proximal obstructions and late in distal obstructions
- Abdominal distension
- Absolute constipation
- Occurring early in distal obstruction and late in proximal obstruction
What are the clinical freatures of bowel obstruction?
Note: on examination
On examination, patients may show evidence of the underlying cause (e.g. surgical scars, cachexia from malignancy, or obvious hernia) or abdominal distension. Ensure to assess the patient’s fluid status, as third-spacing can occur in bowel obstruction.
Palpate for focal tenderness (including guarding and rebound tenderness on palpation). Percussion may reveal a tympanic sound and auscultation may reveal ‘tinkling’ bowel sounds, both signs characteristic of bowel obstruction.
Patients with bowel obstruction may have abdominal tenderness, however should not have features of guarding or rebound tenderness, unless ischaemia is developing.
What investigations should be ordered for bowel obstruction?
Note: laboratory
All patients with suspected bowel obstruction require routine urgent bloods on admission, including FBC, CRP, U&Es, LFTs and a Group and Save (G&S); important to monitor for electrolyte changes and third-space losses.
A venous blood gas can be useful to evaluate the signs of ischaemia (high lactate) or for the immediate assessment of any metabolic derangement (secondary to dehydration or excessive vomiting).
What investigations should be ordered for bowel obstruction?
Note: imaging
A CT scan with IV contrast of the abdomen and pelvis is the imaging modality of choice in suspected bowel obstruction and a shift in modern practice is moving towards CT scanning as the initial imaging used where possible.
A plain abdominal radiograph (AXR) is still used in some settings as the initial investigation for bowel obstruction.
Water soluble contrast study (also termed contrast fluoroscopy, typically using gastrograffin) can also be useful in small bowel obstruction caused by adhesions from previous surgery.
Why are CT scans the imaging of choice rather than AXR?
CT imaging is more useful than AXRs as they are:
- More sensitive for bowel obstruction
- Can differentiate between mechanical obstruction and pseudo-obstruction
- Can demonstrate the site and cause of obstruction (hence useful for operative planning)
- May demonstrate the presence of metastases if caused by a malignancy (which is likewise useful in operative planning).
How does small bowel obstruction present on AXR?
Small bowel obstruction:
- Dilated bowel (>3cm)
- Central abdominal location
- Valvulae conniventes visible (lines completely crossing the bowel)
How does large bowel obstruction present on AXR?
Large bowel obstruction:
- Dilated bowel (>6cm, or >9cm if at the caecum)
- Peripheral location
- Haustral lines visible (lines not completely crossing the bowel, ‘indents that go Halfway are Haustra’)
Briefly describe the conservative management of bowel obstruction
In the absence of signs of ischaemia or strangulation, initial management is essentially conservative and is often referred to as a ‘drip and suck’ management:
- Make the patient nil-by-mouth (NBM) and insert a nasogastric tube to decompress the bowel (‘suck’)
- Start IV fluids and correct any electrolyte disturbances (‘drip’)
- Urinary catheter and fluid balance
- Analgesia as required with suitable anti-emetics
Briefly describe the management of adhesional small bowel obstruction
Adhesional small bowel obstruction resulting from previous surgery is treated conservatively in the first instance (unless there is evidence of strangulation / ischaemia), with a success rate of around 80%.
A water soluble contrast study should be performed in cases that do not resolve within 24 hours conservative management. If contrast does not reach the colon by 6 hours then it is very unlikely that it will resolve and the patient should be taken to theatre.
When is surgery indicated in bowel obstruction?
Surgical intervention is indicated in patients with:
- Suspicion of intestinal ischaemia or closed loop bowel obstruction
- A cause that requires surgical correction (such as a strangulated hernia or obstructing tumour)
- If patients fail to improve with conservative measures (typically after ≥48 hours)
What are the complications of bowel obstruction?
The complications of bowel obstruction include:
- Bowel ischaemia
- Bowel perforation leading to faecal peritonitis (high mortality)
- Dehydration and renal impairment
What differentials should be considered for bowel obstruction?
The differential diagnoses for bowel obstruction include pseudo-obstruction, paralytic ileus, toxic megacolon and constipation.
What is shown in the image?
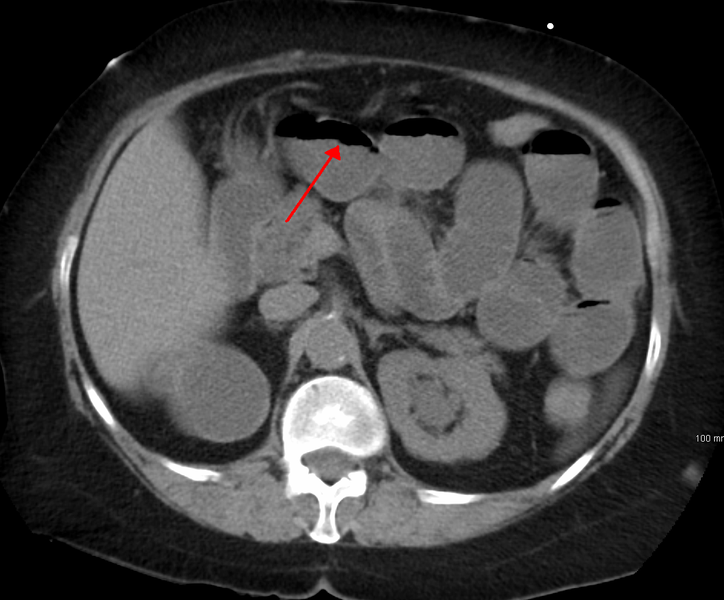
CT scan demonstrating features of small bowel obstruction.
What is shown in image 1?
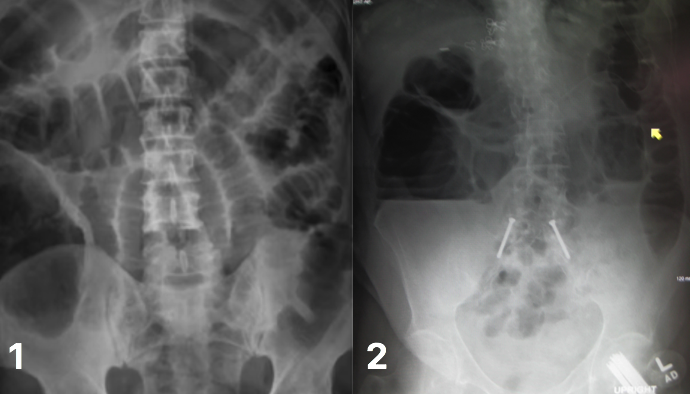
Bowel obstruction on AXR; small bowel obstruction, showing valvulae conniventes crossing a dilated, centrally-located bowel.
What is shown in image 2?
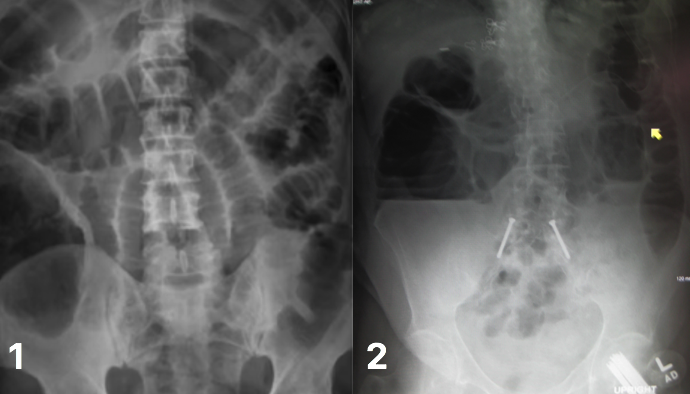
Bowel obstruction on AXR; large bowel obstruction, with peripherally located dilated bowel segments.
-
Abdominal Incisions8
-
Acute Abdomen10
-
Acute Appendicitis24
-
Anal Fissure9
-
Anorectal Abscess9
-
Barrett's Oesophagus17
-
Bowel Obstruction23
-
Colorectal Cancer30
-
Crohn's Disease33
-
Diverticular Disease18
-
Dysphagia8
-
Femoral Hernia17
-
Gastroenteritis9
-
GORD20
-
Haematemesis14
-
Haemorrhoids19
-
Hiatus Hernia20
-
Inguinal Hernia23
-
Oesophageal Cancer17
-
Oesophageal Motility Disorders0
-
Oesophageal Tears22
-
Peptic Ulcer Disease24
-
Perianal Fistula10
-
Pilonidal Sinus11
-
Pseudo-Obstruction9
-
Ulcerative Colitis34
-
Volvulus13
