RECOGNITION OF THE CRITICALLY ILL PATIENT: Describe the use and limitations of risk scoring systems for common critical illnesses such as GI bleeding, pancreatitis, and trauma.
GI bleeding - Glawgow Blatchford
Pancreatitis - Ranson
Trauma - Revised trauma score (GCS, BP and RR)
AF - CHADVASC
RECOGNITION OF THE CRITICALLY ILL PATIENT: Define the various grades of shock and their effects on the major organ systems
Shock: Describes circulatory failure that results in inadequate organ perfusion
Effects on major organ systems
Renal: Reduced urine output
Cerebral: Reduced consciousness
Cardiovascular: Increased HR with eventual reduction, eventual reduction in BP
Respiratory: Elevated RR
RECOGNITION OF THE CRITICALLY ILL PATIENT: Distinguish between hypovolaemic, septic, cardiogenic and anaphylactic shock
RECOGNITION OF THE CRITICALLY ILL PATIENT: Recognise acute severe exacerbation of COPD
Hx: Productive cough, general malaise, fever, chest pain, worsening dyspnoea
Examination: Widespread crackles, focal consolidation, reduced breath sounds
Investigations:
- CXR: Consolidation
- ABG: Acute on chronic type 2 respiratory failure. ABG in ‘health’ would show type 2 respiratory failure with metabolic compensation, allowing pH to be maintained within the normal range. In an acute exacerbation CO2 will increase and compensation will not be enough to keep pH within the normal range.
RECOGNITION OF THE CRITICALLY ILL PATIENT: Recognise clinical features in patients at risk of cardio-respiratory arrest (ILS)
- Respiratory rate < 8
- Obstructed airway
- Cardiac arrest reversible causes: 4Hs and 4 Ts (hypothermia, hypoxia, hypovolaemia, hypokalaemia/hyperkalaemia & tamponade, tension pneumothorax, thrombosis, toxins)
MANAGEMENT OF THE CRITICALLY ILL PATIENT: Describe the reasons for patient’s admission to ITU/HDU and the situations when it is inappropriate to refer a pt to ITU/HDU
Reasons for referral:
- Unable to maintain own airway
- Unable to maintain own BP
Inappropriate to refer:
- Ceiling of care set at ward based care
- Co-morbidities limit benefits
SKILLS IN MANAGING THE CRITICALLY ILL PATIENT: Safely prescribe and administer Emergency anti-microbial therapy in a variety of critical illness situations: meningitis, community and hospital acquired pneumonia, urinary sepsis, and abdominal sepsis.
Meningitis: Ceftriaxone
CAP: Co-amoxiclav
HAP:
- PO Co-amoxiclav for low severity
- IV Piperacillin with tazo for severe infections
Urinary sepsis: Metronidazole
Abdominal sepsis: Cefuroxime and metronidazole
Discuss the basic principles of emergency treatment of haemorrhagic shock; outline steps to be taken in fluid therapy of victims of haemorrhagic shock.
Identify each of the following common life threatening chest injuries (ATOMFC) and discuss their pathophysiology: Airways injuries, Tension pneumothorax, Open pneumothorax, Massive haemothorax, Flail chest, Cardiac tamponade
Describe the following potentially life threatening injuries and outline their initial management: pulmonary contusion, aortic disruption, tracheobronchial disruption, oesophageal disruption, diaphragmatic disruption, myocardial contusion
Outline diagnostic and supportive therapeutic actions for abdominal trauma including the indications and contra-indications for FAST (focused assessment with sonography for trauma).
Discuss the general management and initial investigation of the unconscious traumatised patient
Describe the pathology of head injury, classifying into focal and diffuse. Describe the delayed complications that can follow head injury, classifying into focal and diffuse, and outline the basic principles of rehabilitation in those with cognitive impairment
Describe the main causes, pathophysiological mechanisms and effects of increased intracranial pressure
Outline the therapeutic interventions that, when initiated in the early phases of management, can help to reverse or delay undesirable effects of raised intracranial pressure.
Specify the principles of acute management of the patient with spine or spinal cord injury.
Discuss the aetiology, presentation and emergency management of a compartment syndrome.
SKILLS IN EMERGENCY MEDICINE
- Conduct an initial assessment and management survey on a patient with multiple injuries, using the correct sequence of priorities and explanation of the management techniques for primary treatment and stabilisation.
- Conduct a neurological examination and determine the Glasgow Coma Scale on a patient with head trauma.
- Demonstrate the ability to immobilise the spine on a patient with a back injury.
- Demonstrate the ability to immobilise a fractured limb.
- Interpret the CXR in a patient with severe closed chest trauma.
- Interpret the pelvis and cervical spine radiographs in a trauma patient.
- Observe the performance of a FAST scan in a trauma patient and understand the interpretation of the results.
BURNS: List and differentiate the categories of burn injury; thermal, chemical, electrical, cold and irradiation
Thermal: Due to direct contact with a hot object/vapour.
Chemical: Alkali substances tend to cause worse burns. Can penetrate the skin and be difficult to remove
Electrical: Severity depends upon the strength of voltage and duration of contact
Cold:
Irradiation: May occur due to exposure to X-rays, UV radiation (sun)
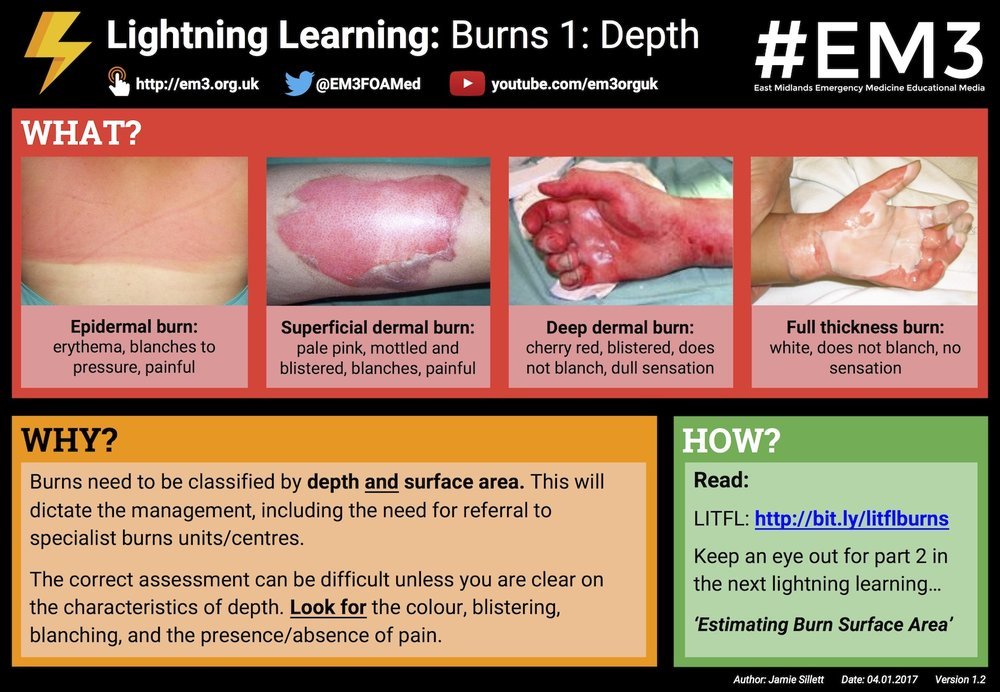
BURNS: Classify the depth of burn injury
Superficial burn: Erythema, branches
↓
Superficial partial thickness burn: Blistered, blanches, painful
↓
Deep partial thickness burn: cherry red, blistered, no blanching, dull sensation
↓
Full thickness burn: white, does not blanch, no sensation
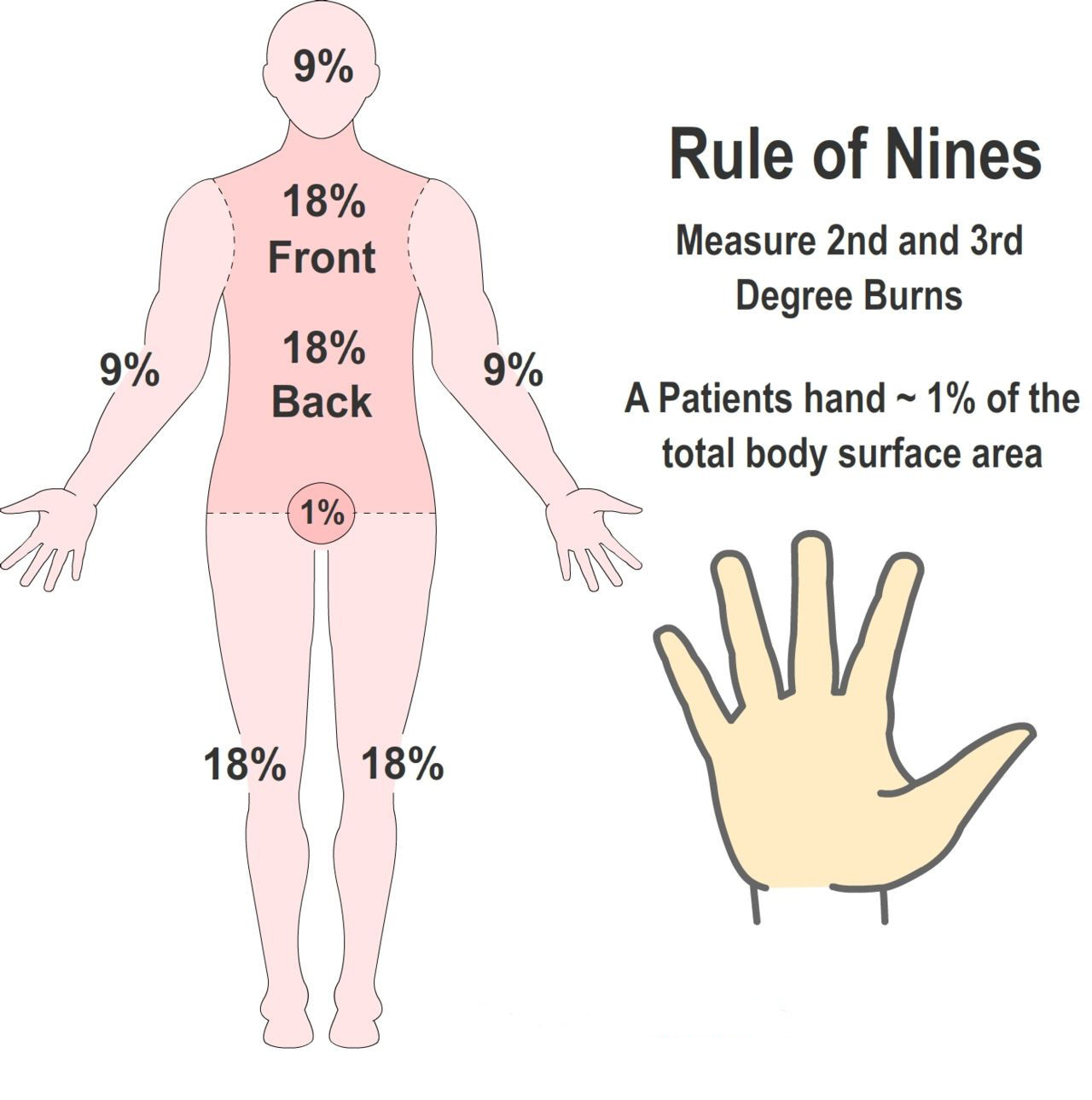
BURNS: Describe and apply the rules of nine
(which areas correspond to 9%)
1% = palm and fingers
BURNS: List the causes, symptoms and signs of inhalation injury
Causes:
- Inhalation of smoke
Signs and symptoms:
- Wheeze/stridor
- Dyspnoea
- Cough with discoloured sputum
- Hoarseness of voice
BURNS: Outline the fluid resuscitation of burns patients, including composition, volume and timing of fluid.
*The greatest loss of plasma occurs in the first 12 hours following the burn
Burns of > 15% in adults, 10% in children, warrant the need for fluid resuscitation.
Crystalloid fluids are used,
The Parkland formula is used to calculate fluid requirements within the first 24 hours:
- 4ml x total burn surface area/TBSA (%) x body weight (kg)
- 50% of the calculate volume should be given in the first 8 hours
- The remainder should be given over the next 16 hours
- Catheterisation to monitor urine output is also required
BURNS: List the other management steps in the initial 24 hours following a burn injury, including general support, wound management and antibiotics.
- Analgesia: Opioids
- Fluids
- Systemic abx if there is evidence of invasive infection
- Wound management
- Partial thickness burn: Use non-adherent dressing. Hands should be covered with sulfadazine cream (sulphonamide abx) and placed in a sealed polythene bag
- Full thickness burn: Total excision of the burn is required. Smaller burns may close primary but larger ones require grafts
*


