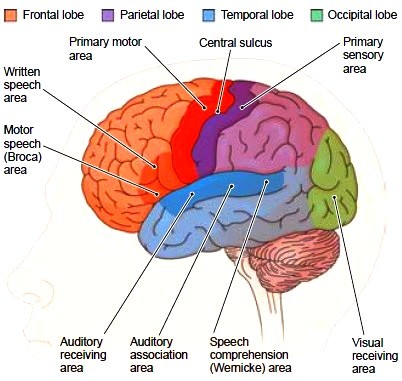
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Label the constituent portions of the cerebral cortex
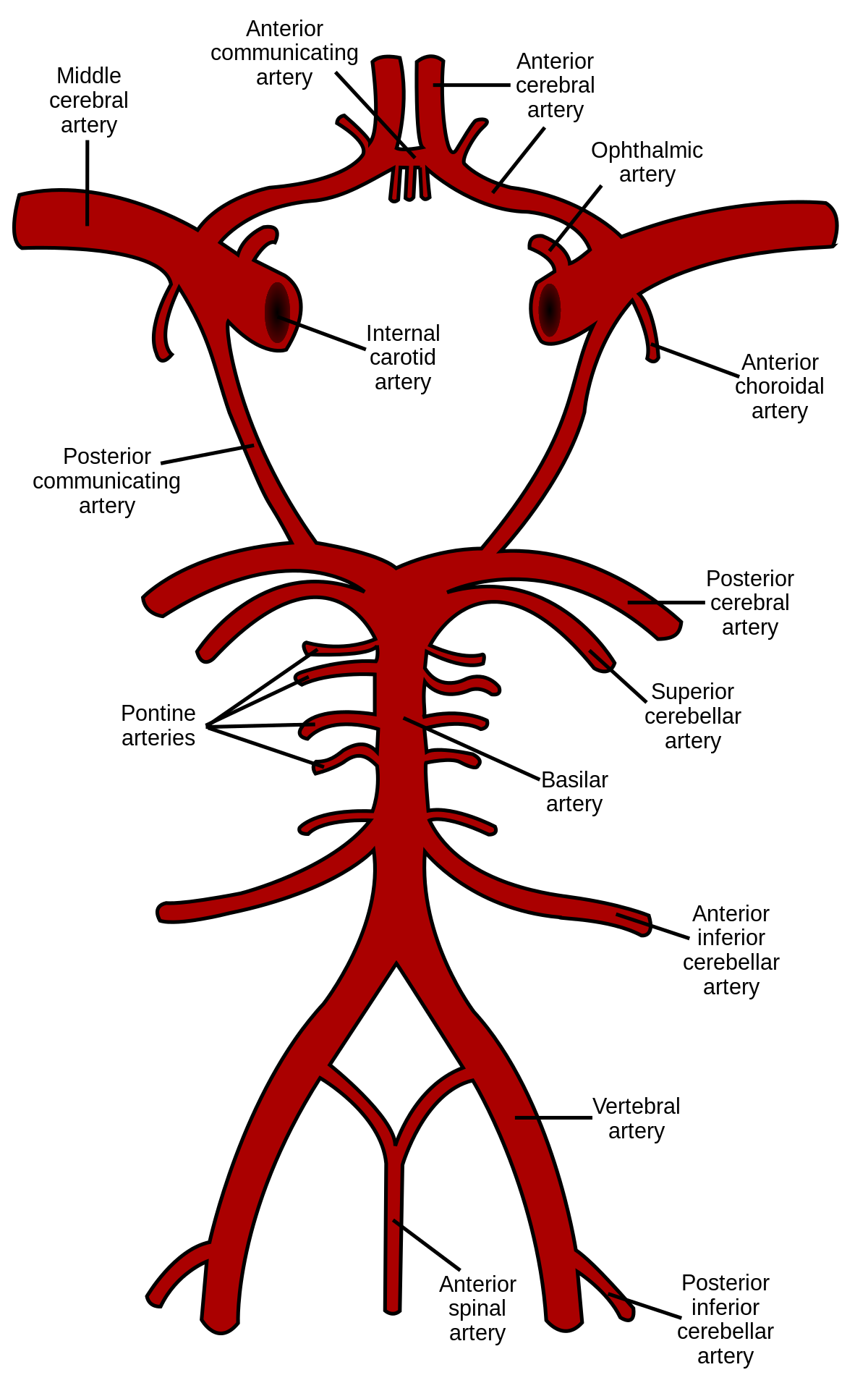
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Draw and label the circle of Willis and its branches
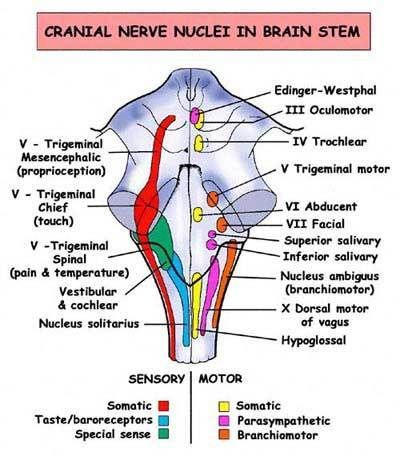
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: List the cranial nerve nuclei in each constituent of the brainstem
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Describe the syndromes which would arise due to a lesion in - cerebral hemisphere, brainstem, cerebellum and basal ganglia
Cerebral hemisphere - Bulbar palsy, stroke/TIA
Brainstem - Pseudobulbar palsy
Cerebellum -
Basal ganglia - Parkinsonism and movement disorders
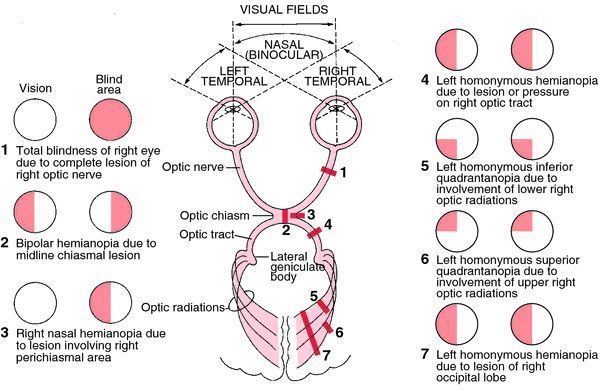
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Name the location of the causative lesion in; Homonymous hemianopia; Homonymous quadrantanopia; Bitemporal hemianopia; Monocular visual field defect
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Describe the location of Broca’s and Wernicke’s area and explain their function in language
Location:
- Broca’s - Frontal lobe of the left hemisphere
- Wernicke’s area - Temporal lobe of the left hemisphere
Broca’s area - Motor function in speech. Infarct in this area leads to expressive dysphasia
Wernicke’s area - Involved in understanding language. Infarct in this area leads to receptive dysphagia e.g. able to formulate words as normal but not able to generate a sentence
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: List the causes of dysarthria
Dysarthria: Occurs when there is a weakness in the muscles used for speech
- Congenital
- Cerebral palsy
- Acquired
- Stroke
- Head injuy
- Malignancy
- Progressive conditions e.g. Parkinson’s, MND
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Explain the difference between bulbar and pseudobulbar palsy
Bulbar palsy: A LMN lesion of cranial nerves VII, IX, X and XII.
Causes: Polio, MND, syringobulbia, cerebrovascular events of the brainstem, GBS
Pseudobulbar palsy: A UMN lesion of cranial nerves IX, X and XII. Lesions affecting the corticobulbar tracts. Bilateral tract damage must occur for clinically evident disease, as the muscles are bilaterally innervated.
Causes: Cerebrovascular events, demyelinating events (e.g. MS), head injury
Bulbar palsy symptoms:
- Absent/reduced gag reflex
- Loss of swallow - may begin to drool
- Fasciculations of the tongue
- Flaccid paralysis
- Absent/reduced jaw reflex
- Nasal speech
Pseudobulbar palsy symptoms:
- Brisk/normal gag reflex
- Constant dribbling
- Spastic paralysis of the tongue
- Brisk/normal jaw reflex
- ‘Donald Duck’ voice
- Bilateral UMN limb signs
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: List the causes of Horner syndrome
Horner’s syndrome: Unilateral facial anhidrosis, partial ptosis, pseudoenopthalmos and miosis. Congenital Horner’s see iris heterochromia.
Causes:
- Carotid artery aneurysm or dissection
- Posterior inferior cerebellar artery or basilar artery occlusion
- Pancoast tumour
- MS
- Cavernous sinus thrombosis
- Hypothalamic lesions
- Cervical adenopathy
- Mediastinal masses
- Pontine syringomyelia
- Aortic aneurysm
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Describe the clinical features of UMN and LMN facial weakness
UMN: Forehead sparing - due to bilateral innervation to CN VII
LMN: Forehead also affected
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Draw and label a cross section of spinal cord, with specific reference to spinothalamic pathways, corticospinal tracts and dorsal columns

BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Describe the clinical syndromes that would arise from cord transection at C3, T10, cord hemi-section and posterior cord lesion
Cord transection at C3: Quadraplegia
Cord transection at T10: Paraplegia
Cord hemi-section: Brown-Sequard syndrome (ipsilateral loss of proprioception and vibration sensations, contralateral loss of pain and temperature sensation alongside ipsilateral limb weakness)
Posterior cord lesion: Loss of proprioception, vibration and light touch. (e.g. subacute combined degeneration (B12 deficiency), tabes dorsalis)
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Describe the clinical difference between upper and lower motor neuron limb weakness, with specific reference to findings on inspection, tone, deep tendon reflexes and pattern of weakness
UMN lesions:
- Brisk reflexes
- Increased tone
- Spastic paralysis
- Presence of primitive reflexes e.g. Babinski
- Disuse atrophy
LMN lesions:
- Absent/reduced reflexes
- Reduced tone
- Flaccid paralysis
- Fasiculations
- Severe atrophy
BASIC NEUROANATOMY AND NEUROPHYSIOLOGY: Describe the clinical syndrome that would arise from S1 root lesion; C5 root lesion; Median nerve compression at the carpal tunnel; Ulnar nerve palsy; Peripheral neuropathy; Neuromuscular junction disorders; myopathy
S1 root lesion
- Lumbar radiculopathy: Unilateral ‘shooting’ pain down the dorsal aspect of the leg in a dermatomal distribution (impingement of the nerve root), with radiation to the foot or toes.
- There may be accompanying motor weakness in a corresponding myotomal distribution
- Causes include intervertebral disc herniation, spondylolithiasis, spinal stenosis, infection or malignancy (metastasis)
- Examination: Positive straight leg test
C5 root lesion
- Cervical radiculopathy: Neck pain, with radiation down the arm, and numbness due to impingement of the cervical nerve root. Dermatomal distribution of pain
- Causes include spondylosis, spondylithesis, disc herniation
Median nerve compression at the carpal tunnel
Carpal tunnel syndrome: Pain, tingling and weakness in the distribution of the distal median nerve. Pain may radiate up the forearm and wasting of the thenar eminence may be seen.
Phalen’s, reverse Phalen’s and Tinel’s test can be undertaken.
Ulnar nerve palsy
- Damage at the elbow: Can occur due to compression of the ulna nerve at the medial epicondyle or in the cubital tunnel
- Motor function: All muscle innervated by the ulnar nerve are affected. Wrist flexion can occur, but only with abduction. Loss of digit abduction and adduction, thumb adduction is impaired (positive Froment’s sign)
- Sensory function loss
- Wasting of hypothenar eminence
- Damage at the wrist: Such as due to laceration of the anterior wrist
- Motor function: Intrinsic muscle of the hand are affected
- Sensory loss: Only over the palm and fingers in the ulnar distribution. The dorsal branch is unaffected.
Peripheral neuropathy
- Loss occurs in the distribution of the nerve, not in a dermatomal distribution
- Diabetic neuropathy: Pain (typically burning) and loss of sensation in a ‘glove and stocking’ distribution
- Shingles
- Alcohol excess
Neuromuscular junction disorders
- Myasthenia gravis
- Botulism
- Lambert-Eaton syndrome: Autoantibodies targeted against acetylcholine. Associated with small cell lung carcinoma.
Myopathy
LUMBAR PUNCTURE: Name the main anatomical landmarks used in guiding lumbar puncture and the coincident level in the spin
Pt on side with knees fully flexed to the chest.
Identify the iliac plane of the iliac crest (L3/L4)
LUMBAR PUNCTURE: Describe the two different positions a patient may adopt to undergo a lumbar puncture, and advantages of each with respect to ease of success and measuring opening pressure
- Lying on side with knees flexed to chest
- Sitting on the edge of the bed
LUMBAR PUNCTURE: List the potential complications of LP
- Post-dural puncture headache (such as following a spinal block. Positional exacerbation - worse when upright)
- Infection at site
- Bleeding from site
- Cerebral herniation *check for signs of raised ICP before proceeding*
- Minor/transient neurological symptoms e.g. radiculopathy, paraesthesia
- Any lower body neurology after LP should be treated as cauda equina compression (haematoma, abscess) and an urgent MRI should be sought
LUMBAR PUNCTURE: List the contraindications to a lumbar puncture
- Raised ICP (papilloedema, very severe headache, reduced consciousness, rising BP, vomiting, focal neurology) - CT prior to LP if suspected
- Bleeding diathesis (prone to)
- Cardiorespiratory compromise
- Infection at site
LUMBAR PUNCTURE: List the acute clinical situations where a LP would be indicated
There are both diagnostic and therapeutic indications for LP:
- Cerebrospinal fluid analysis (i.e. meningitis, multiple sclerosis, subarachnoid haemorrhage, GBS)
- Spinal epidural (i.e. during labour)
- Spinal medications (i.e. analgesia, chemotherapy, antibiotics)
- Fluid removal (i.e. to reduce intracranial pressure)
LUMBAR PUNCTURE: Explain the term CSF xanthochromia
Xanthrochromia describes the yellow-ish appearance of CSF a number of hours (up to 12 hours) following bleeding. The yellow appearance is due to high protein levels within the CSF.
LUMBAR PUNCTURE: Explain the significance of CSF xanthochromia in a sudden onset headache
Highly suggestive of SAH, as bleeding occurs into the subarachnoid space.
The RBCs present in the CSF will also excite an inflammatory response, causing WCC to be raised (most marked after 48 hrs).
LUMBAR PUNCTURE: List the CSF findings that accompany multiple sclerosis
Raised protein content - oligoclonal bands, suggestive of intrathecal Ig production (which are not also present in the blood)
Paired CSF and serum samples are required for accurate interpretation.
- If oligoclonal bands (IgG) are found in CSF and serum this suggests that the Igs have crossed into the CSF, as seen in conditions such as GBS, HIV infection and chronic inflammatory states (autoimmune diseases).
CT AND MRI: List the important contraindications to MRI
- Metal implants or fragments
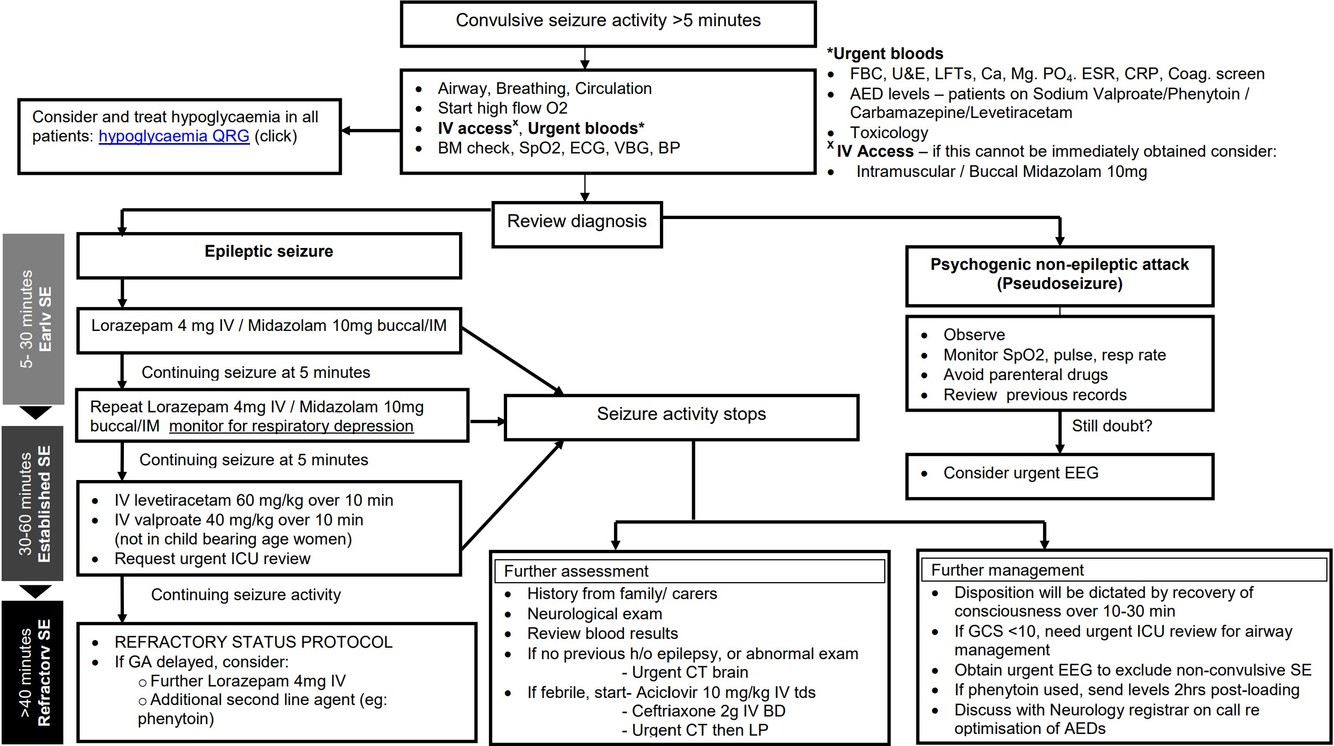
STATUS EPILEPTICUS AS A NEUROLOGICAL EMERGENCY: Define status epilepticus and describe initial investigations and components of management, including airway protection and use if anti-convulsants
Status epilepticus: A convulsive seizure lasting for 5 minutes in duration or recurrent seizures with no recovery in between (?3 seizures in 1 hour).
Initial investigations
- A-E approach
- Secure patency of the airway and give high flow oxygen
- Assess cardiac and respiratory function (ECG, SpO2)
- Check blood glucose levels
- Obtain IV access, fluid resuscitate is necessary
- Urgent bloods and VBG
Management
- Pharmacological treatment:
- 1st line: 4mg IV lorazepam. Repeat after 5 minutes if there is no response
- If no response within 20 minutes, IV levetiracetam, phenytoin or sodium valporate can be administered
- In the community: Buccal midazolam or rectal diazepam may be used