A 58-year-old woman presents to the emergency department (ED) with abdominal pain and distension. She has a history of spina bifida with a neurogenic bladder and chronic constipation, for which she takes an osmotic laxative on a daily basis. She has noted increasing abdominal pain for the week prior to presentation, and she has not passed any stool or gas for 4 days. She reports that she has had progressive abdominal distension and discomfort today, and now has nausea and vomiting, prompting evaluation. On exam, she is morbidly obese, has decreased bowel sounds, and tenderness throughout her abdomen, without guarding or rebound. Rectal examination reveals no palpable stool in the rectal vault. A computed tomography (CT) scan is done in the ED, with the results shown in the figure. Which of the following is the most likely diagnosis?
A. Ileus
B. Colonic malignancy
C. Bowel perforation
D. Diverticulitis
E. Sigmoid volvulus

This woman’s CT scan reveals a sigmoid volvulus, as evident by twisting displacement of the base of the sigmoid colon and mesentery, leading to significant upstream dilation of her colon, with her right colon measuring >15 cm in maximal dimension. Sigmoid volvulus is uncommon, and only accounts for 3-5% of intestinal obstructions, and patients tend to be older with chronic constipation who are institutionalized or have cognitive issues. Management includes urgent endoscopic detorsion, which can help to untwist the colon, and allows removal of air from the proximal distended colon with placement of a decompression tube, with a success rate of 60-80%. Surgery is often performed for patients after the colon has been decompressed in order to prevent recurrence, which is seen in up to 90% of patients. Although a colonic malignancy could cause a mechanical large bowel obstruction, the twisted appearance on the mid pelvis is more suggestive of a volvulus. There is no evidence of free air on the CT scan, so perforation is unlikely. The clinical and radiographic features are not typical for diverticulitis or ileus.
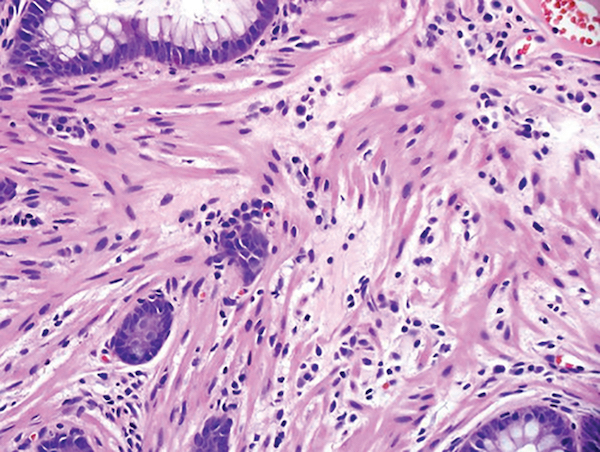
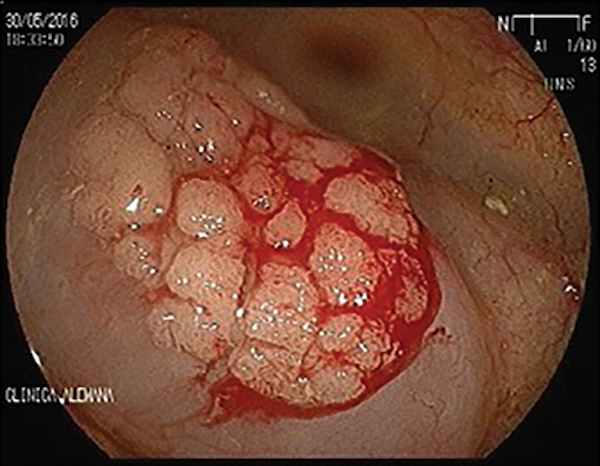
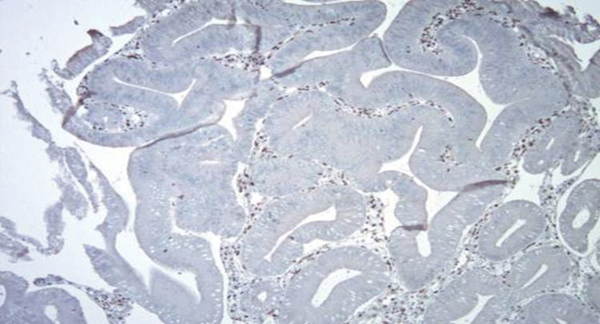
A 66-year-old woman is admitted to the hospital with a 1-day history of abdominal pain and hematochezia. Her prior medical history is notable for poorly controlled type II diabetes mellitus, hypertension, hyperlipidemia, osteoarthritis, glaucoma, and alcoholic cirrhosis. She drinks a half pint of alcohol per day and has done so for 30 years. She smokes 1 pack of cigarettes per day and uses cocaine 3-4 times per month. Her last cocaine use was 3 days prior to admission. She takes ibuprofen 400-800 mg 2-3 times a day as needed for pain. Admission laboratory tests results reveal WBC 9,500/µL, hemoglobin 10 g/dL, INR 2.1, hemoglobin A1c 13.4, FOBT positive, C. difficile negative. She is observed in hospital and prepared for colonoscopy, which reveals the lesion shown in FIGURE A. Biopsy of this lesion is shown in FIGURE B. Which of the following therapies is most appropriate for this condition?
A. Mesalamine suppositories
B. Psyllium
C. Acyclovir
D. Metronidazole

- Histo: characteristic findings of solitary rectal ulcer syndrome (SRUS)
- Dx: clincial, histo, enod.
- Sigmoidoscopy usually demonstrates a single 1-cm ulcer on the anterior rectal wall within 10 cm of the anal verge. The ulcer may have a polypoid appearance in 25% of patients. In a minority of patients, only erythema and hyperemia of the mucosa are seen. Multiple ulcers may be seen in 30% of patients. Histologic features of SRUS include mucosal thickening with elongation, distortion of the glands, edema of the lamina propria, fibrosis, and extension of smooth muscle fibers upwards between the crypts. The hypertrophy and disorganization of the muscularis mucosa are referred to as fibromuscular obliteration
- Treatment includes local agents, improving bowel habits, biofeedback, and surgery. Patients should be placed on a high-fiber diet along with laxatives. They should also be educated to avoid excessive straining and digital manipulation and to reduce the time spent on the toilet.
- Surgery is indicated in patients with severe disease who do not respond to medical or biofeedback therapy or in those with full-thickness rectal prolapse.
A 36-year old woman without significant past medical history presents for consideration of possible subtotal colectomy to address her refractory chronic constipation. She has had constipation for at least 12 years, during which time she has undergone trials of multiple different medications in succession including polyethylene glycol, bisacodyl, lubiprostone, and most recently linaclotide at therapeutic doses for several months each. She also has attempted tap water enemas as needed without relief. She is not on any other medications and denies any other neurologic symptoms.
At baseline, her stool consistency is hard (Bristol 1-2) and even on these laxative regimens, her stools remain solid (Bristol 2-3) and infrequent (every 8-12 days). She also reports bloating and straining with a sense of incomplete evacuation, but denies any issues with abdominal pain. Her prior evaluation includes a colonoscopy which noted retained stool throughout (Boston Bowel Prep Score=3) despite completion of a standard bowel prep, but an otherwise normal appearing colon; radiopaque marker study showed retention of all 24 markers, with 12 markers in the right colon and 12 markers in the left colon at day 6. A wireless motility capsule study revealed a whole gut transit time of 84 hours on her laxative regimen, and defecography demonstrated a small anterior rectocele without a dilated anorectum. Anorectal manometry was performed (bear down maneuver shown in the figure) and balloon expulsion testing yielded a failure to pass the balloon after 5 minutes. What therapeutic recommendation would you make for this patient?
A. Proceed with subtotal colectomy.
B. Repair anterior rectocele.
C. Trial of a tricyclic antidepressant.
D. Increase laxative regimen to include a combination of oral laxatives and suppositories.
E. Pursue biofeedback therapy and pelvic floor therapy program.
- This patient clearly has evidence of slow transit constipation with prolonged retention of radio-opaque markers and confirmed by delayed whole gut transit. She has no features of secondary constipation, and there is no evidence of bowel dilation to suggest mechanical obstruction or colonic pseudo-obstruction. She has failed multiple laxative regimens, decreasing the likelihood of a response to a complex laxative/suppository regimen. On this basis, subtotal colectomy seems a reasonable consideration; however, before proceeding, it is noted that the patient reports symptoms of dyssynergic defecation (straining, incomplete evacuation) and additionally, her anorectal manometry study and balloon expulsion testing suggest an overlapping pelvic floor dyssynergia, with failure to expel the balloon and paradoxical contraction during bear down maneuver. In light of these data, a biofeedback and pelvic floor therapy program should be initiated prior to pursuing a subtotal colectomy for slow transit constipation.
- The patient does not have pain as a predominant symptom, making irritable bowel syndrome with constipation unlikely, and accordingly the use of a tricyclic antidepressant a less attractive option. A small anterior rectocele is more likely a consequence (rather than a cause) of the patient’s defecatory issues.
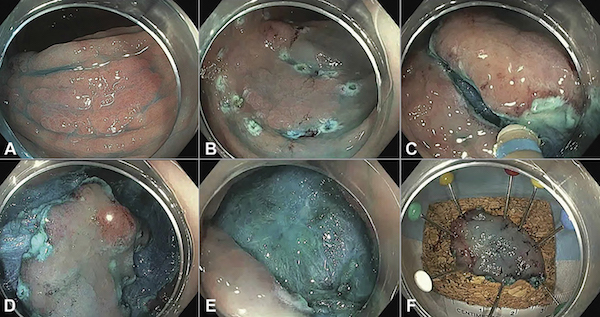
A 70-year-old woman with ulcerative colitis was scheduled for a surveillance colonoscopy. The endoscopist used chromoendoscopy and found a 16-mm sessile serrated polyp in the transverse colon. The endoscopist removed the lesion by hybrid endoscopic submucosal dissection en bloc as seen in the figure. Endoscopically resectable visible nonpolypoid dysplastic lesion removed using hybrid endoscopic submucosal dissection. A, Nonpolypoid superficial elevated serrated appearing lesion. B, The periphery of the lesion is marked, and the lesion is injected using dynamic submucosal injection. C, Circumferential incision. D, Some submucosal dissection. E, The lesion is ultimately resected en bloc using a stiff snare. F, The specimen is pinned for orientation and histologic assessment. Pathology reports indicated that the polyp is a sessile serrated adenoma without cytologic dysplasia. Which of the following is the recommended next step?
A. Schedule a 6-month follow-up colonoscopy.
B. Refer to a surgeon for hemicolectomy due to a high risk of CRC.
C. Schedule a surveillance colonoscopy in 3 years due to a low risk of CRC.
D. Schedule a surveillance colonoscopy in 1 month due to incomplete resection.
SCENIC guidelines recommend surveillance colonoscopy rather than colectomy after complete removal of nonpolypoid dysplastic lesions. Therefore, patients with IBD and large sessile serrated lesions without cytologic high-grade dysplasia removed via EMR, ESD, or in piecemeal fashion should be assigned a 3-6 month interval.
A 75-year-old man with a history of adenomatous polyps presented for a follow-up colonoscopy, 3 years after resection of 2 high-grade dysplastic adenomas. In the ascending colon, a 2-cm flat lateral-spreading tumor (LST), granular-type lesion was found [FIGURE A]. It was completely removed by en bloc endoscopic mucosal resection (EMR). There was prophylactic clipping of the EMR defect [FIGURE B]. No cancer was found in the resection specimen. Which of the following is true for this patient?
A. Prophylactic coagulation of the exposed superficial vessel in the EMR defect will decrease the incidence of delayed bleeding after EMR.
B. The patient should have annual stool-based surveillance by fecal immunochemical test (FIT).
C. The patient should have surveillance colonoscopy in 3 years.
D. The patient should have a right hemicolectomy.
- LSTs are superficial. More than 10 mm in diameter, lesions extend more laterally than vertically in the colonic wall. There are 2 sub-types: a) granular type and b) nongranular type. Granular type LSTs with big nodules or depressed areas have higher risk of submucosal invasion. Therefore, removal needs expertise and completeness.
- This patient who had a 2-cm LST without malignancy and had complete en-bloc endoscopic resection should undergo surveillance colonoscopy in 3 years.
- Recently, a study showed that prophylactic coagulation of the EMR defect did not impact delayed bleeding rates. No FIT is indicated. Surgery is an alternative in incomplete resection (appendix base invasion, nonlifting sign) or in lesions with submucosal invasive carcinoma
A 68-year-old woman with a history of hypertension, diabetes, and chronic obstructive pulmonary disease presents with 24 hours of cramping abdominal pain and bloody diarrhea. She notes that the symptoms started with the sudden onset of abdominal pain and was followed by 4 episodes of bloody diarrhea. In the emergency department, she is found to have a heart rate of 96 beats per minute and a blood pressure of 95/60. She receives 1 liter of normal saline and her vital signs improve to a heart rate of 75 beats per minute and blood pressure of 120/85. The patient has had no recent changes to her medications, sick contacts, or recent travel. Her last colonoscopy was 4 years ago and was remarkable for the presence of 2 tubular adenomas. She has a CT scan showing a segmental colitis. One week later, she has a colonoscopy with the finding shown in the figure. What is the most common segmental distribution for this patient’s disease?
single stripe sign seen
A. Cecum
B. Ascending colon
C. Transverse colon
D. Descending colon
E. Rectosigmoid colon
The patient has “colon ischemia” or “ischemic colitis.” This is clear from the description of the presentation, which is classic for this disease state. The patient also has the most significant risk factor for colon ischemia, which is COPD. Finally, the image shows the “single stripe sign,” the colonoscopic finding most commonly associated with colon ischemia. The most common distribution of colon ischemia involves the left colon, specifically the rectosigmoid colon. The disease distribution is also importantly associated with severity of disease. Patients with isolated right colonic disease distribution are at the highest risk for poor outcome.
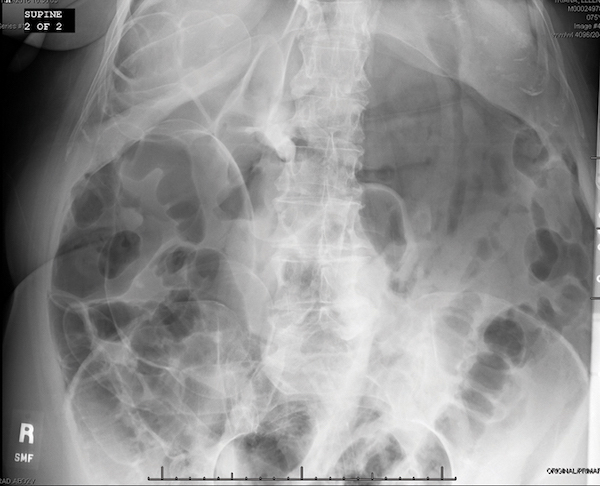
A 62-year-old man on clopidogrel with a history of hypertension, chronic obstructive pulmonary disease, and coronary artery disease with stent placement 2 years ago presents to the emergency department with acute onset of abdominal pain. He rates his abdominal pain to be 9/10 on a pain scale and describes it as a sharp band throughout his abdomen. He undergoes an initial x-ray [FIGURE]. What is the best next step in the management of this patient?
A. Ultrasonography with dopplers of the abdomen
B. Emergency laparotomy
C. Admittance to general medicine and intravenous fluids
D. CT angiography of the abdomen and pelvis

- The x-ray shows pneumatosis linearis lining the right colon. In this circumstance, there is concern for isolated right colon ischemia with possible necrosis.
- The most important next test is an angiographic study to delineate how to best treat the patient.
- Ultrasound with dopplers, and even CT of the abdomen and pelvis alone, might miss a vascular obstruction that requires immediate interventional radiology or vascular surgical intervention.
- Calling surgery for an emergency laparotomy might be best if there was clear evidence of a perforated viscus, but in this case, the vascular imaging is most important because that will triage the best methods to reverse the process.
- Admitting to medicine and treating with conservative measures would be a dangerous choice for this patient.
A 55-year-old woman, para 2, without any history of back trauma or injury presents with a 4-year history of progressively worsening fecal incontinence. She cannot sense stool coming out and wets her pants frequently, using 3 pads daily. She had a normal colonoscopy 1 year ago. She denies any bleeding. Her stools are mostly formed (Type 4 on a Bristol stool scale). The patient trialed on psyllium without any relief of her incontinence. To assess this patient further, an anal ultrasound study was performed [FIGURE]. Which of the following findings best describes the anal ultrasound image?
A. Decreased resting and squeeze anal sphincter tone
B. Large external anal sphincter defect but normal internal anal sphincter
C. Normal external anal sphincter but large internal anal sphincter defect
D. Decreased squeeze tone
E. Large external and internal anal sphincter defect
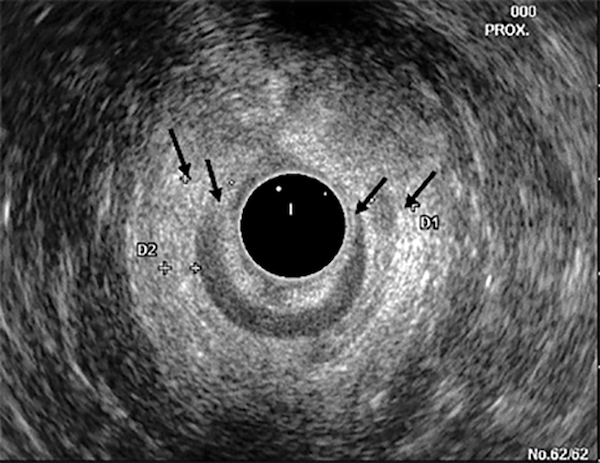
- The anal sphincter profile was obtained during rest with an anal ultrasound probe.
- Typically, one would observe an intact homogenous hypoechoic internal anal sphincter (IAS) ring and an intact hyperechoic external anal sphincter (EAS) ring. In a patient with anal sphincter trauma (often obstetrical), there is loss of continuity in one or more sphincters and sometimes presence of a dense scar, usually in the anterior sector.
- Responses B and C are incorrect, because the anal sphincter defect involves both the EAS and IAS. Responses A and D are incorrect because an anal ultrasound test does not provide manometric information but morphological information
A 56-year-old woman presents for screening colonoscopy. She has had 2 previous attempts at colonoscopy that were unable to be completed due to tortuosity of the colon. Those procedures were terminated in the transverse colon. Today, with the help of pressure, the scope is passed with ease to the cecum. She has three 1-2-mm sessile polyps resected with a cold biopsy forceps. Following the procedure, the patient feels well and is discharged. She calls you about 2 hours later stating that she is having excruciating abdominal pains. You return her call and advise her to go to the emergency department. In the ED, the abdominal x-ray reveals the following [FIGURE]. What segment of the colon is most likely involved with this complication?
A. Cecum
B. Ascending colon
C. Transverse colon
D. Descending colon
E. Sigmoid colon
The sigmoid colon has been shown to be the most common location for colonic perforation in multiple studies. The largest study that looked at this was a 16-year study with 30,366 colonoscopies. There were 35 perforations (0.12%) or 1 in 1,000. The most common location for perforation was the sigmoid colon with 26 perforations (74%).
A 59-year-old woman presents with iron-deficiency anemia. You perform colonoscopy. On examination, a 25-mm malignant appearing mass was detected in the transverse colon. You request your pathologist perform immunohistochemistry (IHC) for expression of mismatch repair proteins on the biopsy specimens you obtain from the tumor. The IHC result is shown in FIGURES A and B. IHC of MSH2 is on the left [FIGURE A] and of MLH1 on the right [FIGURE B]. What is the best next step in the management of this patient?
A. Send patient for genetic counseling and testing for Lynch syndrome.
B. Perform microsatellite instability (MSI) testing on the tumor.
C. Test the tumor for a BRAF mutation.
D. Recommend prophylactic TAH/BSO at time of colon cancer surgery.

All colorectal cancers should undergo tumor testing for assessment of mismatch repair (MMR) deficiency (also known as microsatellite instability) by either MSI or IHC testing. In the figure, IHC of the tubulovillous adenoma from which the cancer arises demonstrates intact expression of the MSH2 protein and lack of expression of the MLH1 protein. Lack of expression is an abnormal result and confirms MSI and the specific MMR protein defect. The latter may be due to promoter methylation of MLH1 in the tumor which occurs in cancers arising from a sessile serrated polyp (SSP) or a germline mutation in the MLH1 gene which occurs in Lynch syndrome. The next step in determining the etiology of the cancer and optimal patient management is tumor BRAF mutation or MLH1 promoter methylation testing. If either are present, Lynch syndrome is excluded and suggests a sporadic cancer arising from an SSP.
A 56-year-old man with no significant past medical history presented for screening colonoscopy. His examination was remarkable for a 1.8-cm laterally growing superficial area of irregular mucosa in the ascending colon that you suspect is a lateral spreading tumor (LST). What LST sub-classification [FIGURE] has the highest risk of submucosal invasive cancer?
A. Granular, homogenous
B. Granular, nonhomogenous
C. Nongranular, flat elevated
D. Nongranular, pseudodepressed
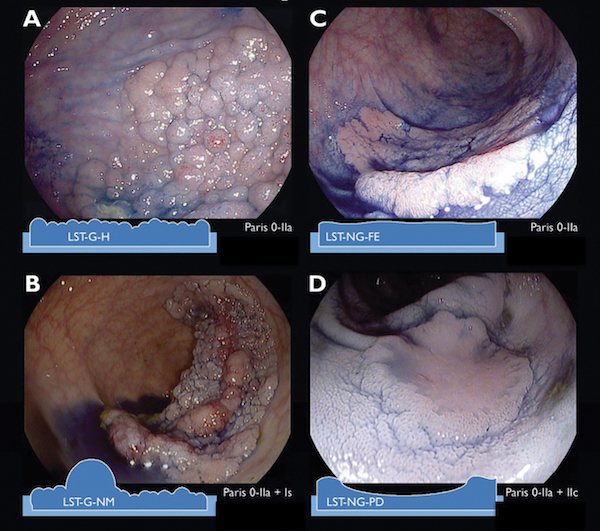
In one study of lateral spreading tumors (LSTs), submucosal invasion (SMI) was identified in 8.5% of cases and high-grade dysplasia in 36.7% of cases. Within this study, geographic region did not influence the SMI risk and nongranular LSTs were more frequently associated with SMI than granular LSTs: 11.7% vs. 5.9%. The prevalence of SMI in LSTs stratified by endoscopic LST subtype were: 31.6% in pseudodepressed nongranular LSTs, 10.5% in nodular mixed granular LSTs, 4.9% in flat elevated nongranular LSTs, and 0.5% in homogenous granular LSTs. Within that study, SMI was also more common in distal rather than proximal LSTs and the proportion of SMI increased with lesion size (10-19 mm, 4.6%; 20-29 mm, 9.2 %; ≥30 mm, 16.5%).
A 65-year-old woman comes in for her first screening colonoscopy. She is asymptomatic and has no family history of colorectal cancer (CRC). The endoscopist found 4 polyps in the recto-sigmoid ranging from 2-4 mm as shown in the figure [hyperplastic polyps, NBI]. What would be the recommended next step?
A. Leave polyps in place
B. Cold large capacity forceps polypectomy
C. Cold snare polypectomy
D. Hot biopsy forceps
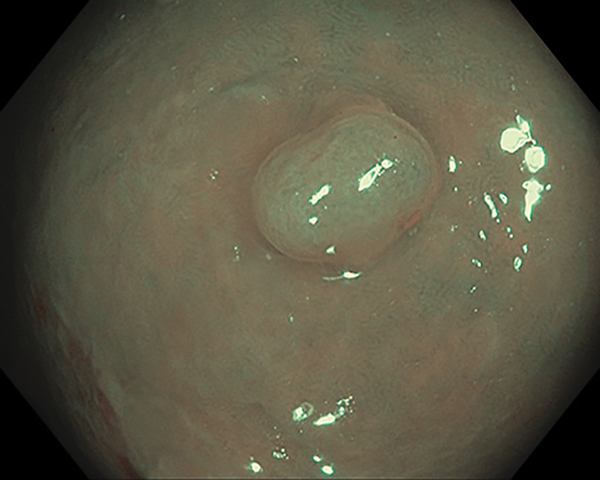
Using the NICE classification with narrow band imaging, these polyps can be diagnosed as hyperplastic with high confidence. It is recommended to leave hyperplastic diminutive polyps of the rectal and sigmoid colon in place. Using this classification, experienced endoscopists have achieved 93% concordance of surveillance intervals made by real-time optical diagnosis and pathology, and a >90% negative predictive value for rectosigmoid polyps when assessments were made with high confidence.
Which of the following colorectal cancer screening test(s) has been proven (with randomized controlled trials) to reduce colorectal cancer mortality?
A. Fecal occult blood testing
B. Sigmoidoscopy
C. Colonoscopy
D. Fecal occult blood testing and colonoscopy
E. Fecal occult blood testing and sigmoidoscopy
- There have been several randomized controlled trials (RCTs) demonstrating that guaiac-based fecal occult blood tests (gFOBT) reduce colorectal cancer mortality by 33% with annual screening and 15-18% with biennial screening.
- Fecal immunochemical testing (FIT) identify intact human hemoglobin in stool and are more sensitive than gFOBT, but have not been proven in RCTs to reduce cancer mortality.
- There have been 4 RCTs of sigmoidoscopy use and colorectal cancer mortality, and these have demonstrated reduced cancer mortality compared to usual care (approximately 27% mortality reduction, by meta-analysis).
- While there are several RCT’s underway that compare colonoscopy to either usual care or to FIT, there is only indirect evidence of the mortality benefit of colonoscopy. This indirect evidence includes prospective cohort studies and case-control studies.
A 60-year-old patient presented for a surveillance colonoscopy. He had a 35-mm flat granular type lesion removed by piecemeal resection. Coagulation forceps were used at the time of the EMR for bleeding hemostasis. Clips were placed to close the defect. The pathology showed tubular adenoma. Surveillance colonoscopy findings in 6 months show neoplastic recurrence at the site. What is the polyp feature most associated with higher risk of local recurrence?
A. Lesion size of 35 mm
B. Use of clips
C. Intraprocedure bleeding
D. Low-grade dysplasia
- Local neoplastic recurrence following endoscopic resection of large colorectal lesions has been reported in several longitudinal outcomes studies to be approximately 16%. It is typically unifocal and diminutive, and can be managed endoscopically.
- Risk factors associated with higher local recurrence rates include
- lesion >40 mm
- use of argon plasma coagulation to treat endoscopically visible residual lesion
- intraprocedure bleeding
- high-grade dysplasia
- A recursive partitioning analysis of patients who had endoscopic resection of advanced lesions and surveillance within 3 years showed the highest recurrence rate in those with a high-grade dysplastic lesion ≥15 mm.
- A recent recurrence prediction tool for lesions ≥20 mm was proposed to risk stratify patient surveillance intervals. Using a 4-point scale (size ≥40 mm = 2, intraprocedure bleeding = 1, high-grade dysplasia = 1), the cumulative incidence of recurrence in lesions with a score of 0 did not increase between 6 and 18 months (11.6%), where as the cumulative incidence of recurrence in lesions with a score of 1-4 increased from 23.0% at 6 months, 36.3% at 18 months, and 39.5% at 36 months.
- As such, low-risk lesions could potentially have first surveillance at 18 months, whereas high-risk lesions require intense early surveillance at 6, 18, and 36 months.
A 35-year-old female ICU nurse presents in outpatient consultation for chronic diarrhea and abdominal pain. She reports 3-5 watery, nonbloody stools a day with associated abdominal cramping pain over the past several months, and she has presented to the emergency room on several occasions for pain control and concern that she may have acquired C. difficile at work. Her previous evaluation has included a normal complete blood count and metabolic panel, and negative stool testing for C. difficile toxin B by PCR on 2 separate occasions. Stool microbiologic testing for enteric pathogens and parasites is negative. Upper endoscopy, colonoscopy, biopsies of small bowel and colon, abdominal CT, and MR enterography are all normal. Stool electrolyte testing is ordered following the consultation, with the following results: Stool sodium 30 eEq/L, potassium 70 mEq/L, and stool osmolarity was 100 mEq/L. What is the most likely explanation for this patient’s test results?
A. Gastrinoma
B. Stool specimen contamination or dilution
C. Idiopathic secretory diarrhea
D. Small intestinal bacterial overgrowth (SIBO)
- The osmolarity of stool under normal circumstances is similar to plasma osmolarity (290 eEq/L). In this particular case, the low osmolarity suggests that the stool has been diluted, perhaps with hypotonic urine or water.
- This dilution may be accidental or volitional (factitious diarrhea). Stool urea can be measured to confirm contamination with urine.
- Factitious diarrhea is more common in women, especially those in health care professions.
- The calculated osmotic gap is 290 – 2x (30 +70) is 290-200 = 90, which is not the low gap (less than 50 mEq/L) that you would see with a secretory diarrhea, such as a gastrin producing tumor or idiopathic secretory diarrhea.
- SIBO more typically leads to a stool gap in osmotic range (>125 mEq/L) and would not be associated with a low stool osmolarity.
A 70 kg patient is admitted to the hospital with presumed immune checkpoint inhibitor-induced colitis. The patient is having profuse watery diarrhea. Once fluid resuscitation is accomplished and other causes of diarrhea (C. difficile, CMV, etc.) have been ruled out, initial therapy should include which of the following?
A. Oral budesonide
B. Oral prednisone
C. IV methylprednisolone
D. IV Infliximab
Budesonide and oral prednisone are not consistently effective in patients ill enough to require hospitalization. While there are no large trials demonstrating the utility of IV steroids (typically 1-2 mg/kg dosing) for steroid refractory diarrhea, clinical experience to date supports a stepwise approach of oral steroid, IV steroid, and then anti-TNF therapy with uniformly good outcomes. For this inpatient, starting with intravenous steroid therapy would be most appropriate.
A 53-year-old woman with no co-morbidities undergoes screening colonoscopy. The Boston Bowel Preparation Score is 9 and the cecum is intubated and documented with a photograph of the appendiceal orifice. In the left colon, a 25-mm pedunculated polyp is removed and the area tattooed. The pathology demonstrates cancer within the head of the polyp. Which of the following pathologic findings would prompt you to refer this patient for surgical resection?
A. There is tumor at the resected margin.
B. No lymphatic or vascular invasion is observed.
C. The tumor is well differentiated.
D. The tumor involves 35% of the head of the polyp
When cancer is found within a resected polyp, several features (primarily histologic) may be used to predict the risk for locally advanced disease involving lymph nodes. Unfavorable features which would prompt surgical resection include tumor at the resected margin or extending into the stalk, lymphatic or vascular invasion, poor differentiation, and extension into the submucosa. When carcinoma is confined to the head in a pedunculated polyp, and no unfavorable features are present, the risk for metastatic disease is very small and treatment with polypectomy alone is adequate
What is the minimum performance target for overall ADR?
25%
Because some endoscopists perform colonoscopy for primarily male or female patients (e.g., endoscopists in Veterans Affairs hospitals or female endoscopists with largely female patient populations), an ADR target of 30% is recommended for men and 20% for women.
A 58-year-old woman is found to have adenocarcinoma of the ascending colon during routine screening colonoscopy. She is asymptomatic and otherwise in good health. There is no family history of colorectal cancer or polyps. She undergoes right hemicolectomy, and immunohistochemistry of the surgical specimen shows lack of expression of MLH1 protein. Subsequent testing reveals a BRAF mutation. Which of the following is appropriate?
A. No further testing
B. Referral for genetic counseling
C. Surgical referral for completion colectomy
D. Tumor testing for microsatellite instability
Universal testing of CRC for Lynch syndrome (LS) is strongly advocated by several professional organizations. Immunohistochemistry of CRCs utilizing antibodies to the Mutation Mismatch Repair (MMR) gene proteins MLH1, MSH2, MSH6, and PMS2 evaluates for the loss of MMR protein expression. This loss can be due to germline mutation (as in Lynch syndrome), or somatic due to epigenetic silencing of the MLH1 gene by methylation. To distinguish these 2 mechanisms, testing can be done for mutations in the BRAF oncogene. Mutations in BRAF are usually seen in sporadic (non-LS) CRC, and associated with the CpG island methylator phenotype (CIMP) and microsatellite instability (MSI). Given that the patient described has no concerning family history and the molecular features of the CRC are that of sporadic cancer, then referral for genetic counseling and additional surgery are not indicated. Testing for MSI when IHC has already been performed is not necessary, but is a reasonable alternative option to IHC if this was not done or is not available
An 18-year-old woman presents with 2 weeks of post-prandial epigastric pain and a 6-lb weight loss. The patient has no past medical problems or surgeries, and takes no medication. She is a senior in high school, does not use drugs or alcohol, and denies a history of abuse or an eating disorder. She is a thin, fit-appearing woman who is comfortable. She is 5’2”, 95 lb, BMI 17.4, P 72, RR 12, BP 96/67.
The following laboratory test results are within normal limits - CBC, TSH, metabolic panel, celiac panel, and lipase. An EGD is normal, and a gastric emptying scan with a semisolid meal has a gastric emptying time of 73 minutes (normal: 50-70 minutes). A CT scan of the abdomen with oral and IV contrast is performed and demonstrates narrowing of the aorta mesenteric angle measuring approximately 20 degrees. Further, these CT findings result in compression of the third portion of the duodenum between the SMA and aorta. The patient also undergoes an UGI series which demonstrates delayed passage of contrast past the duodenal bulb. The history and imaging support a diagnosis of SMA syndrome and you plan on treating the patient for this disorder. What do you recommend at this time?
A. Start low-dose metoclopramide after discussing the risks and benefits.
B. Start low-dose amitriptyline at bedtime after discussing the risks and benefits.
C. Refer the patient for surgery.
D. Start total parenteral nutrition.
E. Start nasojejunal tube feeds.
- While SMA syndrome is a controversial diagnosis, it is reasonable to consider in this patient. Consistent with this diagnosis are the radiologic findings of an aorta mesenteric artery angle of <25 degrees, compression of the duodenum, and delayed passage of contrast on an UGI series.
- First line therapy is conservative with nutritional support, and enteral is favored over parenteral when possible. Often, until patients are able to take enough calories orally, a nasojejunal feeding tube is utilized. Another option is a small bowel feeding tube distal to the duodenal obstruction. Once weight gain is achieved, patients become more reliant on oral intake. If enteral feeding fails or is not possible, then total parenteral nutrition can be tried.
- Finally, if several months of nutritional support is unsuccessful, then surgery should be considered and several surgical approaches to relieve the SMA obstruction have been described. However, most literature reporting the outcome of such surgery is limited to single institution retrospective studies and variable success is described.
- If there is concern for an eating disorder, a psychiatric consult should be recommended. Finally, there is no role for metoclopramide or amitriptyline in the treatment of SMA syndrome.
A 70-year-old man had one 35-mm tubular adenoma in the ascending colon discovered on a recent colonoscopy. The physician performed piecemeal endoscopic mucosal resection (EMR) and clipped the polypectomy site with 4 hemoclips. No other polyps were found in the colon. Which surveillance interval should be assigned to this patient?
A. 3 months
B. 1 year
C. 2 years
D. 3 years
It is recommended to repeat colonoscopy in 3-6 months to assess for local recurrence after piecemeal EMR.
A 45-year-old man has had watery diarrhea for many years. He typically has 5-6 stools daily, mostly in the mornings, but sometimes after lunch and dinner. He does not wake at night with diarrhea and has not lost weight. He saw a gastroenterologist before moving to your city 3 years ago and had a full work-up including stool studies, blood work, colonoscopy with biopsies, and upper endoscopy; all were normal, including CT of the abdomen and pelvis. You have him collect a 24-hour stool on 100 gram fat diet. It shows 560 grams of stool, 5 grams of fat. What is the best treatment option?
A. Subcutaneous octreotide weekly
B. Cholestyramine powder
C. Pancreatic enzymes
D. Gluten-free diet
- This is most likely functional diarrhea but may be due to primary bile acid diarrhea (BAD) and thus could respond to cholestyramine. BAD may account for up to 40% of diarrhea-predominant IBS or functional diarrhea and in some cases, is related to a genetic mutation in the normal regulation of bile acids, so that more bile acids reach the colon causing watery diarrhea.
- The volume of stool is not consistent with a secretory diarrhea so octreotide should not be given. The fat content is normal so treatment of pancreatic insufficiency or celiac disease is not indicated.
A 55-year-old woman is hospitalized with prerenal azotemia that responds to volume repletion. You are asked to see her in consultation. She tells you that she has been having voluminous diarrhea for months, following a trip to Crater Lake in Oregon. She traveled with several family members, and none of them are sick. She has 6-7 watery, nonbloody stools every day, and 1-2 times a night her diarrhea awakens her from sleep. She has been drinking ample water and sports drink, but still has a hard time staying hydrated and has now has lost 20 lb of weight. She does not have any abdominal pain. Stool cultures have been negative. CT imaging, colonoscopy, and upper endoscopy are all normal. You order a 24-hour stool collection and it shows 1,800 grams of stool, 12 grams of fat/24 hours, Na=119 eEq/L, and K=17 mEq/L, magnesium 17 mEq/L, osmolarity 285 mEq/L, and laxative screen is negative. Which of the following is the most likely diagnosis?
A. Pancreatic insufficiency
B. Factitious diarrhea
C. Idiopathic secretory diarrhea
D. Irritable bowel syndrome
This is a secretory diarrhea with large volume and the low osmotic gap is established by the equation 290 – 2x (Na + K) in stool. In this case, the stool osmotic gap is 290- 2x (119+17) = 3. The increased fat likely reflects the large volume of stool output, rather than maldigestion, as in pancreatic insufficiency or malabsorption, as in mucosal disease. The volume of stool collected is higher than typically seen with IBS, and weight loss and lack of abdominal pain are against IBS. Also, IBS is not typically associated with a sectretory pattern. Factitious diarrhea is less likely given the normal stool osmolarity and magnesium, as well as a negative laxative screen.
A 54-year-old man with a history of hypertension, diabetes, coronary artery disease, and recent myocardial infarction about 2 months prior to presentation with resultant left ventricular ejection fraction of 15% presents with the acute onset of severe abdominal pains. He rates the pain 8/10 and diffuse throughout his abdomen. His abdominal exam shows a soft abdomen with some mild tenderness, but no rebound or guarding. The patient undergoes a CT scan that shows mesenteric fat stranding with some ascites. What should be done next to help diagnose this patient?
A. Magnetic resonance angiography
B. Emergent exploratory laparotomy
C. Selective mesenteric angiography
D. Re-review of the portal venous imaging by radiology
This patient has a classic history and imaging of acute mesenteric ischemia (AMI). Given the recent myocardial infarction with reduced ejection fraction, he most likely has a nonocclusive mesenteric ischemia, but this is not completely clear from the history. The patient’s CT scan showed general findings consistent with mesenteric ischemia and his pain is “out of proportion on exam.” In patients who have signs of AMI and there is a CT scan with portal venous contrast already performed, there is evidence to show that calling the radiologist for further review of the original imaging can avoid delay in diagnosis and identify similar information compared to performing a CT angiogram. An MR angiogram is an accurate study, but the time required for this study is extensive and would delay diagnosis, increasing the likelihood of necrosis and a poor outcome. Calling a surgical consult could be helpful, but this patient does not have evidence of necrosis and therefore a surgical intervention is not indicated at this time. Selective mesenteric angiography also could be helpful in diagnosing the etiology of the AMI, but similar to the CT angiogram, a call to the radiologist to re-review the imaging to assess the SMA for patency would the most appropriate next assessment.




