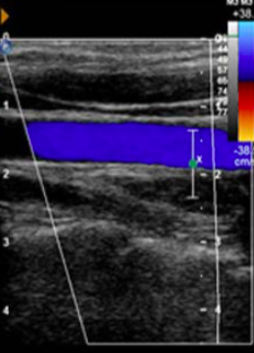
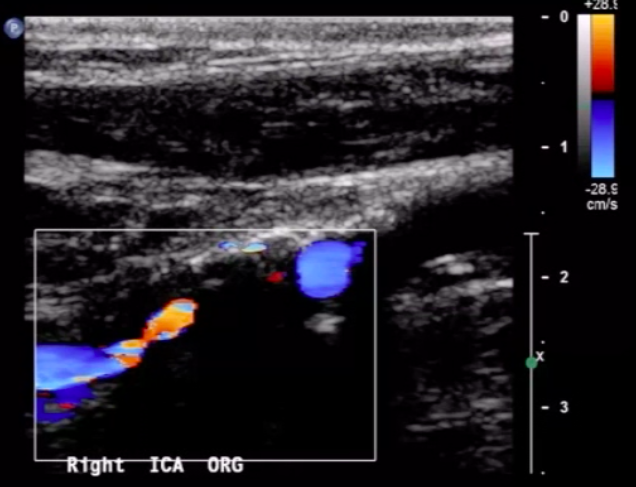
For the following arterial duplex US (DUS) image:
comment on the PRF setting
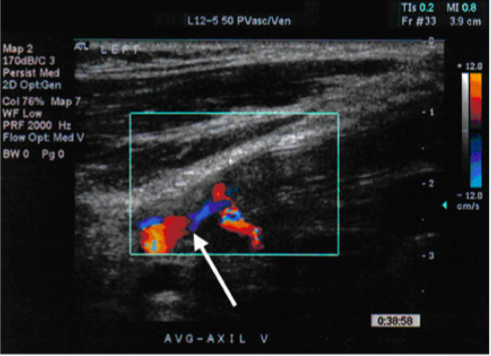
PRF is set very low
you can tell this based on the velocity range of the color bar (range of 12 cm/s, relatively low setting
recall that PRF value is directly-related to color doppler frequency parameters (and the associated blood velocity)
Name 7 indications for carotid duplex ultrasound (DUS) exam.
screening (primary prevention)
- asymptomatic bruit
- prior to CTS
monitoring known disease (2o prevention)
- f/u of known atherosclerotic carotid dz (ACaD)
- f/u after carotid revascularization
acute ischemic cerebrovascular event (r/o carotid etiology)
- r/o carotid dissection
- r/o carotid source of embolus (in setting of stroke or amaurosis fugax)
other → suspected subclavian steal
Where should CCA velocity ideally be measured?
a few cm proximal to carotid bifurcation
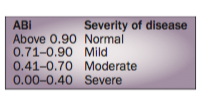
Give the range of ABI values that correspond to borderline, mild, moderate, and severe PVD.
ABI values:
- 0.91-0.99→borderline abnormal
- 0.71-0.90→mild PAD
- 0.41-0.70→moderate PAD
- _<_0.40→severe PAD
normal ABI range is 1.0-1.40
Pt with abdominal pain after eating has arterial duplex US images shown below. Most likely diagnosis?
*Note that left panel images were taken from supine position and right panel from sitting position.
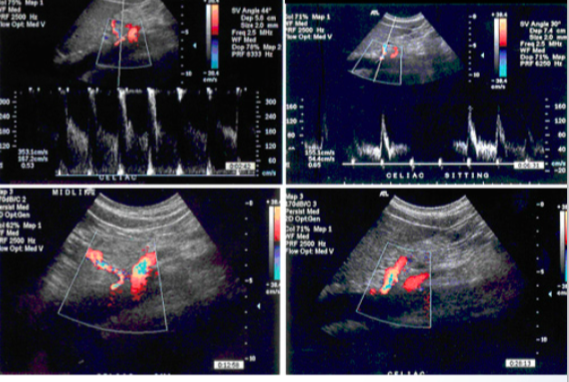
median arcuate ligament syndrome
- velocities increase with expiration in supine images only
- above occurs due to compression of celiac artery by median arcuate ligament
Carotid DUS images shown below. Diagnosis?
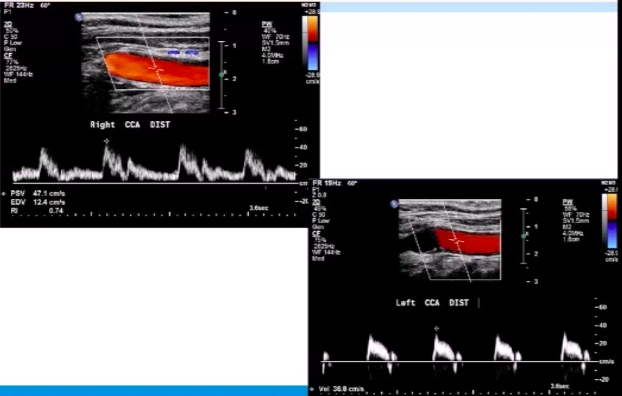
left ICA occlusion
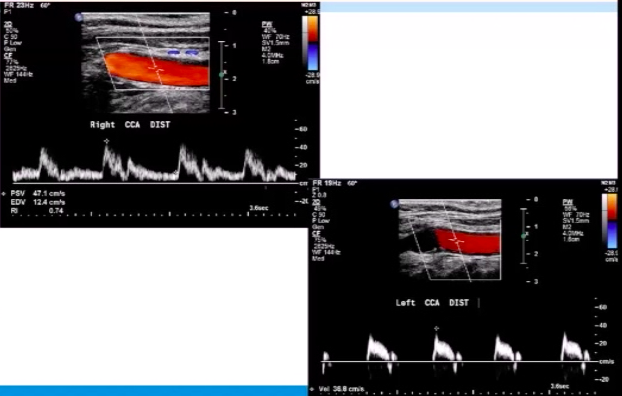
note the externalization* of the left CCA in the DUS image
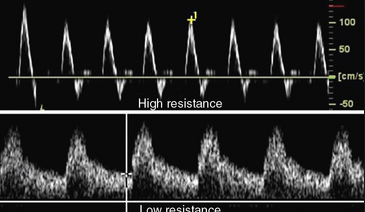
*occurs when CCA waveform has solely a low-resistance pattern (implies blockage of high-restistance ICA branch)
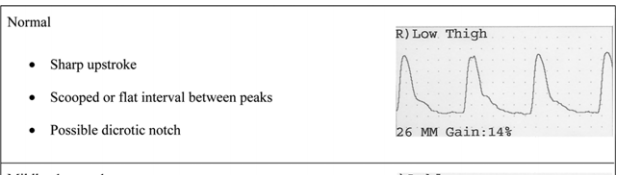
For the PVR tracing below, what is the severity of PAD?
normal PVR tracing ⇒ no vascular disease present
normal PVR contour looks like a handgun:
- brisk upstroke
- scooped/flat diastolic interval (+/- dicrotic notch)
- normal amplitude
Identify the 2 vessels* in the images shown below.
*the vessels with arrows pointing to them
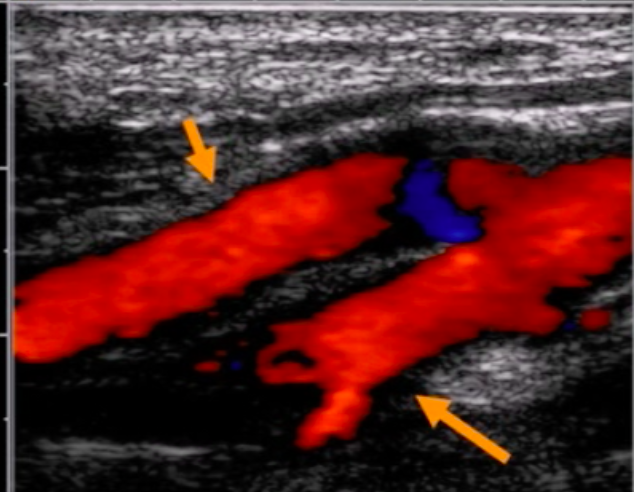
top vessel is ICA and bottom vessel is ECA
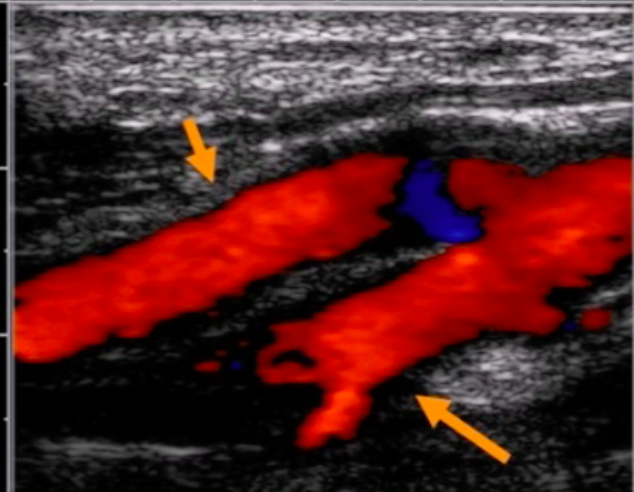
bottom vessel has branches ⇒ it is the ECA
Carotid DUS imaging shown below. Diagnosis?
near-total ICA occlusion
note significant ICA plaque with low velocities distal to lesion (“falling off spencer-reid curve”)
In which direction is blood flowing in the vascular duplesx US (DUS) image shown below?
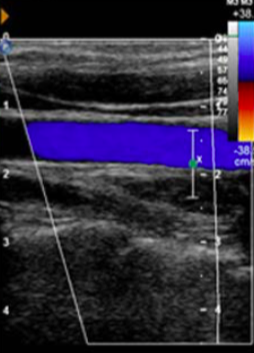
to the left
- image is steered to right ⇒ blood flowing to right will appear as (-) ðf* and blood flowing to left will be a (+) ðf
- color bar shows blue as (+) ðf
- blood is blue in image ⇒ blood is flowing to left
ðf = doppler shift
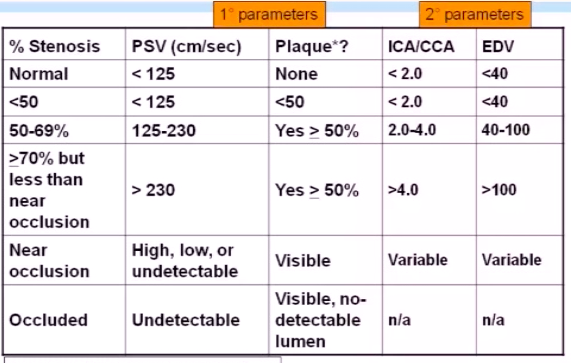
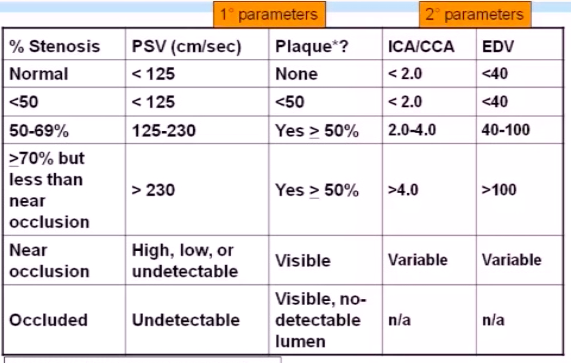
Give the algorithm for DUS grading of carotid stenosis (NASCET based, 4 steps).
step 1: assess PSV
- <125 cm/s → go to step 2
- 125-230 cm/s → go to step 3
- >230 cm/s → go to step 4
- undetectable → 100% occlusion
step 2: assess plaque burden
- < 50% ⇒ mild (<50%) stenosis
- >50% → indeterminate, go to step 3
step 3: assess EDV
- <40 cm/s ⇒ mild (<50%) stenosis
- 40-100 cm/s ⇒moderate (50-69%) stenosis
- >100 cm/s ⇒ indeterminate, go to step 4
step 4: assess ICA/CCA ratio
- >4.0 ⇒ severe (>70%) stenosis
- 2.0-4.0 ⇒ ⇒moderate (50-69%) stenosis
Name 7 carotid diseases that can be identified on carotid duplex imaging.
dysplastic - fibromuscular dysplasia
neoplastic - carotid body tumor
inflammatory - large vessel vasculitis (GCA and Takayusu’s)
degenerative
- carotoid aneurysm
- ACaD (Atherosclerotic Carotid Disease)
trauma
- carotid pseudoaneurysm/AVF
- carotid dissection
Name the 3 secondary parameters that are used in the NASCET (aka SRU) criteria for assesment of carotid stenosis.
- extent of plaque on 2D US
- PSVICA/PSVCCA ratio
- EDV
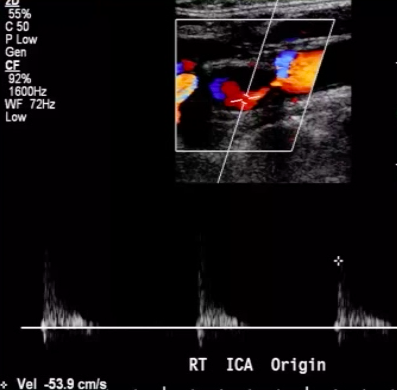
Patient has Lt ICA 100% occlusion. Rt carotid system shown below. PSV = 208 cm/s in proximal Rt ICA.
Most likely diagnosis?

mild Rt ICA stenosis (<50%)
since Lt ICA is 100% occluded, there should be elevated Rt CCA velocities (CCFA*)
plaque in proximal Rt ICA is <<50% ⇒ elevated velocities across Rt ICA are likely due to CCFA
*CCFA = compensatory carotid flow augmentation
What are the 3 descriptors that you should use when characterizing luminal plaque in your report?
- echodensity of plaque:
- hypoechoic (reference = blood)
- isoechoic (reference = sterncleidomastoid m.)
- hyperechoic (reference = bone)
- uniformity of plaque
- homogeneous - has uniform echogenicity
- heterogeneous - has both hypoechoic AND hyperechoic regions
- shape of plaque
- smooth
- irregular
- ulcerated
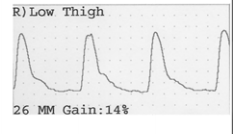
For the PVR tracing below, what is the severity of PAD?
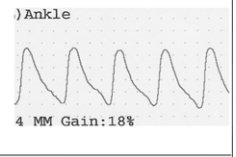
mild PAD
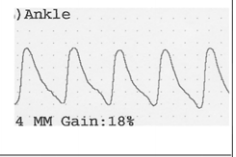
mild PVR contour looks like a capital N
- brisk upstroke
- gradual downstroke without flattening/scooping (and no dicrotic notch)
In which direction is this image steered?

to the left
steering color doppler imaging to left → diagonal border points to 6-9 o’clock region

Carotid DUS imaging shown below. Diagnosis?
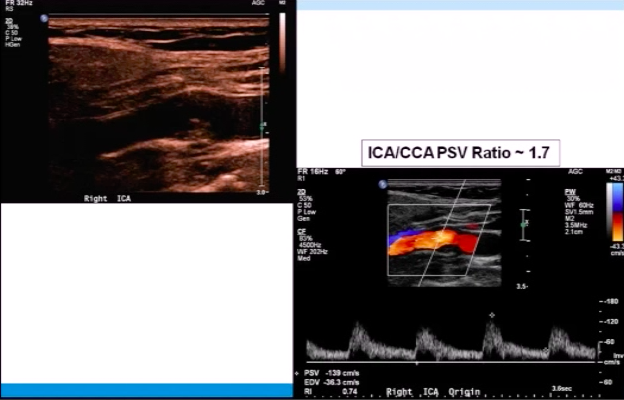
50-69% ICA stenosis
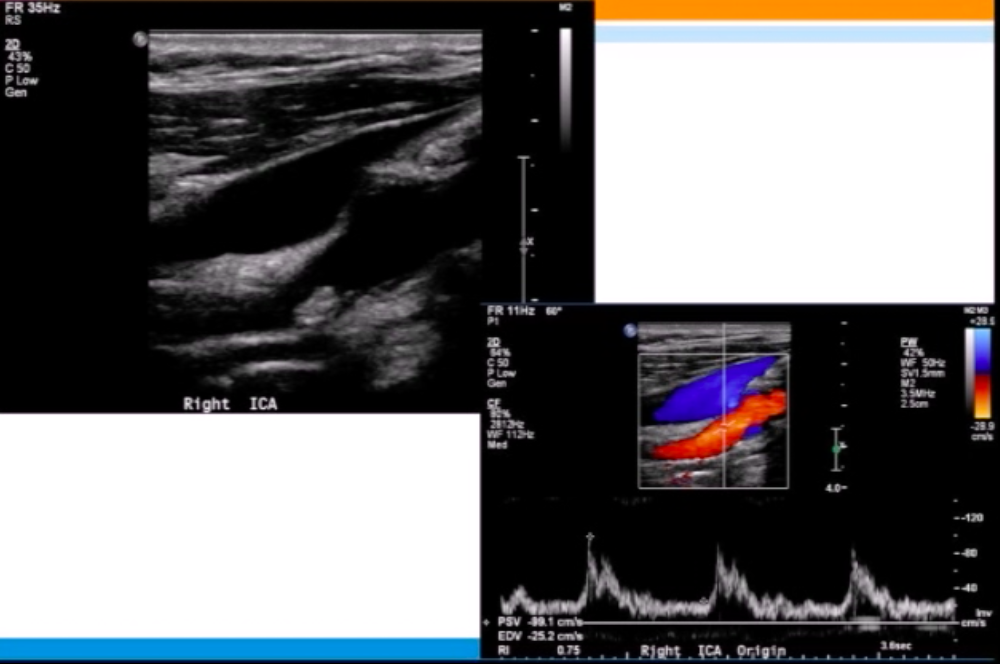
Carotid DUS imaging shown below. Diagnosis?
normal exam
Name the artifact and associated pitfall shown in this image.

artifact: acoustic shadowing due to calcific plaque
pitfall: blood velocity distal to calcium often cannot be assessed
*image shows ICA lesion
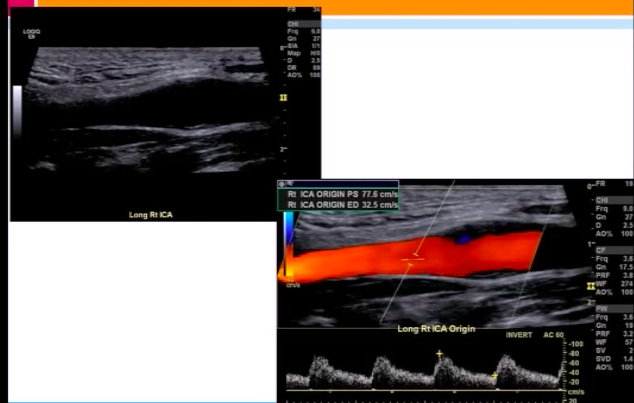
Carotid DUS imaging shown below. Diagnosis?
<50% stenosis
note the <50% atheroma in the proximal ICA with PSV ~80 cm/s
Tech calls you asking for your advice on the carotid DUS shown below. What to tell her?
try power doppler or changing the DIA*
image shows calcific lesion in right ICA → region of stenosis cannot be interrogated w/ color doppler due to acoustic shadowing
*DIA = doppler interrogation approach
With regard to vascular duplex US (DUS) imaging:
Positive doppler shifts (ðf) are encoded with which color?
whichever color is a/w plus sign on color bar
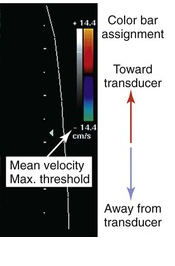
i. e. (+) sign on color bar ⇒ (+) ðf
note: if no sign is present on color bar, then whichever color is above the baseline (red in this example) is assigned (+) ðf
note: the mnemonic BART (blue away, red towards) does not always hold for vascular imaing
The external carotid artery has a _____ resistance wave form (on arterial dopple imaging).
The external carotid artery has a high resistance wave form.